
Abstract
Background:
Iodine, an essential micronutrient, plays a critical role in normal growth and development, especially during the first two years of life. This systematic review and meta-analysis is among the first to evaluate breast-milk iodine concentrations and infant iodine status in countries characterized by iodine sufficiency or deficiency.
Methods:
PubMed, Web of Science, Cochrane Library, Google Scholar, and other relevant databases, as well as reference lists of previous reviews, were searched for relevant studies published between 1986 and 2016. Mean or median breast-milk and infant urinary iodine concentrations, along with other relevant data, were extracted from eligible studies. Each study was assessed for quality and risk of bias.
Results:
Of the 496 identified studies, 57 met the criteria for inclusion in the meta-analysis. The mean (confidence interval [CI]) iodine concentrations in maternal colostrum were 152.0 μg/L [CI 106.2–198.7 μg/L] and 57.8 μg/L [CI 41.4–74.1 μg/L] in iodine-sufficient and -deficient countries, respectively, indicating a significant difference between the two iodine statuses. By contrast, the corresponding values in mature milk did not differ significantly between mothers in iodine-sufficient and -deficient countries (71.5 μg/L [CI 51.0–92.0 μg/L] and 28.0 μg/L [CI −13.8 to 69.9 μg/L], respectively]. The weighted urinary iodine levels [CIs] of breast-fed infants in iodine-sufficient countries were significantly higher than those in iodine-deficient countries (164.5 μg/L [CI 116.4–212.7 μg/L] vs. 70.4 μg/L [CI 46.2–94.6 μg/L]). Similarly, a significant difference was observed in the pooled estimates of urinary iodine levels [CIs] among formula-fed infants in iodine-sufficient versus iodine-deficient countries (310.3 μg/L [CI 287.4–342.1 μg/L] vs. 38.3 μg/L [CI 23.4–53.2 μg/L]).
Conclusion:
The meta-analysis reveals that in iodine-sufficient countries, the mean iodine concentrations in colostrum and mature breast milk corresponded to iodine sufficiency among infants. The results are thus compatible with the international recommendation that lactating women and infants younger than two years of age who reside in iodine-sufficient countries do not require iodine supplementation.
Introduction
I
Previous international studies have provided evidence of considerable variation in the iodine concentrations of breast milk between regions classified as iodine sufficient and those considered iodine deficient (6 –9). However, mean or median breast-milk iodine concentrations (BMIC) have been reported to vary widely (range 5.4–2170 μg/L), even in populations considered iodine sufficient (6 –9). In addition, a scientific consensus on the normative range of BMIC has not been reached, and therefore cutoff values indicative of a sufficient BMIC and the provision of adequate iodine to meet the requirements of infancy have not yet been determined (10 –13). In a study by Bazrafshan et al., a cutoff of 50 μg/L was used to indicate a sufficient BMIC (14), whereas in a review by Azizi et al., values >75 μg/L were suggested to indicate sufficient iodine intake (6). In some studies, a range of 150–180 μg/L has been proposed to indicate an adequate BMIC (9), whereas others have suggested a BMIC of ≥100 μg/L to ensure a sufficient supply of iodine to full-term breast-fed infants (8).
Currently, the main indicator of iodine intake in a population is the median urinary iodine concentration (UIC). The WHO, Iodine Global Network (IGN; previously the International Council for the Control of Iodine Deficiency Disorders [ICCIDD]), and the United Nations Children's Fund (UNICEF) have declared a median UIC of ≥100 μg/L in lactating women and infants as indicative of iodine sufficiency (15). Data from different countries have shown that under the circumstances of both iodine sufficiency and mild deficiency, an infant's demands for iodine and thyroid hormones are sufficiently provided by breast milk via a compensatory mechanism in the mammary gland and an upregulation of the sodium–iodide symporter (NIS) to transfer iodine from the mother to the infant. Accordingly, the BMIC, rather than the maternal UIC, may be a promising marker of iodine nutrition in breast-fed infants. However, few studies have investigated this parameter, which makes it difficult to reach a firm conclusion (16 –18).
Currently, the use of median UIC to measure the iodine status in infants is complicated by the difficulty of sample collection, and accordingly the best criteria for assessing an infant's iodine status have not yet been established (19). In addition, whether the infant iodine status can be reflected by the BMIC remains uncertain, given the wide variations in BMIC among different countries. Hence, to the best of our knowledge, this systematic review and meta-analysis is the first to explore the iodine nutrition status of infants in relation to the BMIC of mothers residing in iodine-sufficient or -deficient countries.
Methods
Search strategy
A systematic literature search was conducted of all studies published between March 1986 and April 2016 in the following electronic databases: MEDLINE, Cochrane Library CENTRAL, and Scopus. Other relevant databases, such as those maintained by the WHO (
Study selection and data extraction
Two investigators conducted the search independently. Once the search was completed, the titles and abstracts of the identified studies were scanned to exclude obviously irrelevant material. The full texts of the remaining studies were retrieved, and all relevant articles were identified. The criteria for inclusion in the systematic review were as follows: all articles related to human studies; inclusion of healthy lactating mothers and their healthy full-term newborns and infants younger than two years of age as target participants; and reported BMIC and infant UIC data. The following exclusion criteria were applied: animal studies; non-English language studies; studies in which mothers and/or infants had been exposed to environmental factors (e.g., perchlorate, tobacco smoking, and iodine overload via iodine-containing contrast media, radioactive iodine, or povidone-iodine disinfection) that may have influenced the BMIC or UIC; studies of lactating mothers with thyroid diseases and/or pre-term, low birth weight (LBW), and unhealthy infants; duplicate publications; and potentially relevant articles lacking full texts.
Data from the included studies were extracted independently by two investigators using standardized forms developed for this review. Any identified discrepancies were resolved by consensus. The following data were extracted: first author, year of publication, country or location of study, type of iodine fortification, level of iodization, numbers of mothers and infants, postpartum interval and/or infant age, type of infant feeding, and mean or median BMIC and infant UIC data.
Quality assessment
Study quality was assessed using the Newcastle–Ottawa scale, and each study was scored based on three different criteria: selection of the study samples, comparability of the groups, and ascertainment of the outcome of interest. Each study received zero, one, and/or two stars for each criterion, and an overall quality score was calculated as the sum of the individual stars. For descriptive purposes, we used Newcastle–Ottawa scores of 2–3, 4–6, and 7–10 to indicate a low, moderate, and high quality, respectively.
Data synthesis
The mean values and standard errors (SEs) of the BMIC and infant UIC were calculated based on the median, lower and upper interquartile range (IQR), upper and lower range, standard deviation (SD), lower and upper SE of the mean, or lower and upper confidence interval (CI) (20) if the mean and SE were not directly mentioned. The results of different arms were pooled in some studies, and these pooled results were considered as one arm in the final analysis if clinical or methodological heterogeneity was not observed. Additionally, the results of studies conducted in different regions of the same country were pooled as for a single study. If BMICs were reported at different stages of lactation (colostrum or mature samples) in a single study, these were included as two separate studies in the analysis. If studies reported the BMIC in different time points from each stage of lactation, the results corresponding to each stage were pooled as a single study. The iodine status of each country was defined based on the median UIC of the general population at time of the study when the study of lactating mothers and infants was conducted. School-age children were used as a proxy for the iodine status of the general population, with median UIC values ≥100 and <100 μg/L indicating iodine sufficiency and deficiency, respectively.
Statistical analysis
The mean BMIC and infant UIC values and CIs were estimated for different subgroups based on the national iodine status (iodine sufficiency vs. iodine deficiency) and type of feeding (breast-feeding vs. formula feeding). For the analysis, a fixed/random effect model based on the absence/presence of heterogeneity was used. Statistical heterogeneity was evaluated according to Q Cochrane (heterogeneous in p-value <0.1) and the I 2 index (>50%) (21). To evaluate publication bias, Begg and Egger tests (significant for a p-value <0.1) and funnel plots were used (22). In relevant cases, the trim and fill method was used to overcome publication bias. Corrected results were expressed after trimming if they differed significantly from the situation where publication bias was present. A Forest plot was used to demonstrate the mean BMIC and infant UIC values and corresponding CIs of different subgroups. Stata v12.0 (Stata Corp, College Station, TX) was used for all analyses.
Results
Study characteristics
The flow chart for this review is given in Figure 1. A total of 496 titles and abstracts were screened after the electronic search. Of these, 71 appeared potentially relevant, and the full text was assessed for inclusion. Twenty-one of these potential studies were excluded because they failed to meet the inclusion criteria; of these, most failed to report BMIC data of lactating mothers or UIC data of infants younger than two years of age. Seven additional publications were included after a screen of the reference lists, yielding a total of 56 studies for inclusion in the present systematic review. Among these, 28 studies were conducted in iodine-sufficient countries. Of these, 20 were from iodine-deficient countries (Tables 1 and 2), and eight assessed BMIC and UIC associated with mothers who had undergone iodine supplementation (Tables 3 and 4). Twenty studies assessed the iodine status in both breast milk and infant urine samples, 26 reported only the iodine concentration in breast-milk samples, and 11 measured only UICs in infants.
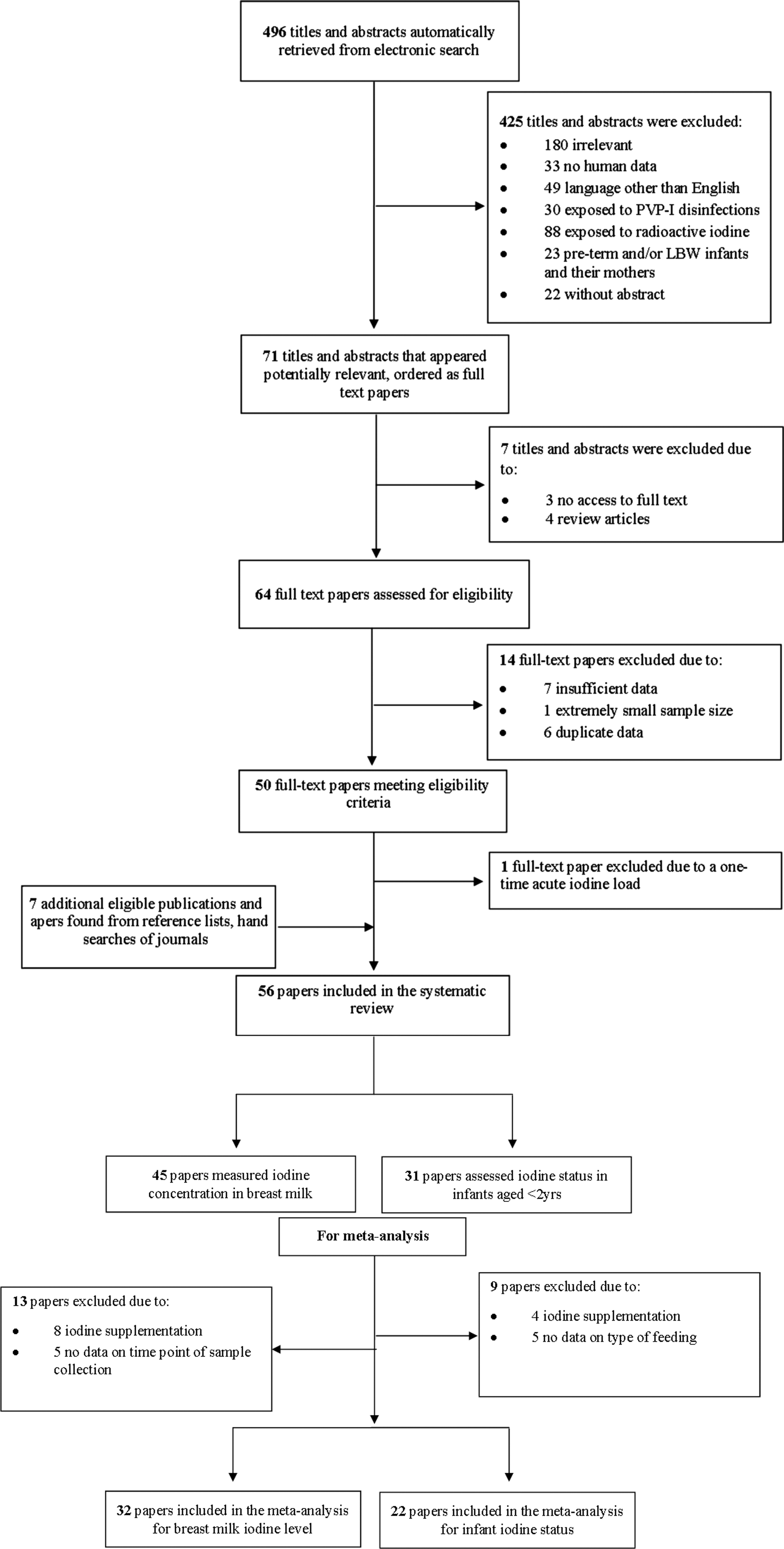
Flow chart for selection of eligible studies for the present systematic review and meta-analysis. PVP-I, povidone iodine; LBW, low birth weight.
Results from different regions of a country with different iodine status.
Results from different regions of a country.
Median.
Median (interquartile range).
Median (minimum–maximum).
Mean.
Mean ± SD.
Mean ± SEM.
Mean (SEM range).
Mean [CI].
IS, iodized salt; ppm, parts per million; NS, not stated; SD, standard deviation; SEM, standard error of the mean; CI, confidence interval.
Results from different regions of a country with different iodine status.
Results from different regions of a country.
Median.
Median (interquartile range).
Median (minimum–maximum).
Median [CI].
Mean ± SD.
Mean (SEM range).
Mean (CI).
BF, breast-feeding; EBF, exclusive breast-feeding; EFF, exclusive formula feeding; PFF, partial formula feeding.
Median.
Median (interquartile range).
Median (minimum–maximum).
Median [CI].
Mean ± SD.
BF, breast-feeding; EBF, exclusive breast-feeding; EFF, exclusive formula feeding; PFF, partial formula feeding.
Median [CI].
Median (interquartile range).
Median.
Median (minimum–maximum).
Regarding the BMIC, after excluding the studies in which mothers were supplemented with iodine (n = 8) and those without data corresponding to the time point of sample collection (n = 5), 32 studies remained eligible for inclusion in the meta-analysis. These included 11 studies that reported iodine concentrations in colostrum collected generally at 2–10 days postpartum, 17 that assessed iodine levels in mature milk samples collected at ≥10 days postpartum, and four that measured iodine in both colostrum and mature milk samples. Regarding the infant iodine status, after excluding studies in which mothers were supplemented with iodine (n = 4) and in which the type of feeding was not reported (n = 5), 22 studies remained eligible for the meta-analysis. These included six studies that measured urinary iodine levels in both breast-fed and formula-fed infants, and 16 that assessed the iodine status in only breast-fed infants. The quality scores of the studies included in the meta-analysis ranged from 6 to 9 (Table 5). Twenty-nine studies received high-quality scores, and 13 received moderate scores.
The asterisks denote the score(s) for each criterion. One asterisk denotes a score of 1, and two asterisks denote a score of 2.
Newcastle–Ottawa scores 2–3, 4–6, and 7–10 were considered as having low, moderate, and high qualities, respectively.
Colostrum iodine concentrations in lactating mothers residing in iodine-deficient versus -sufficient countries
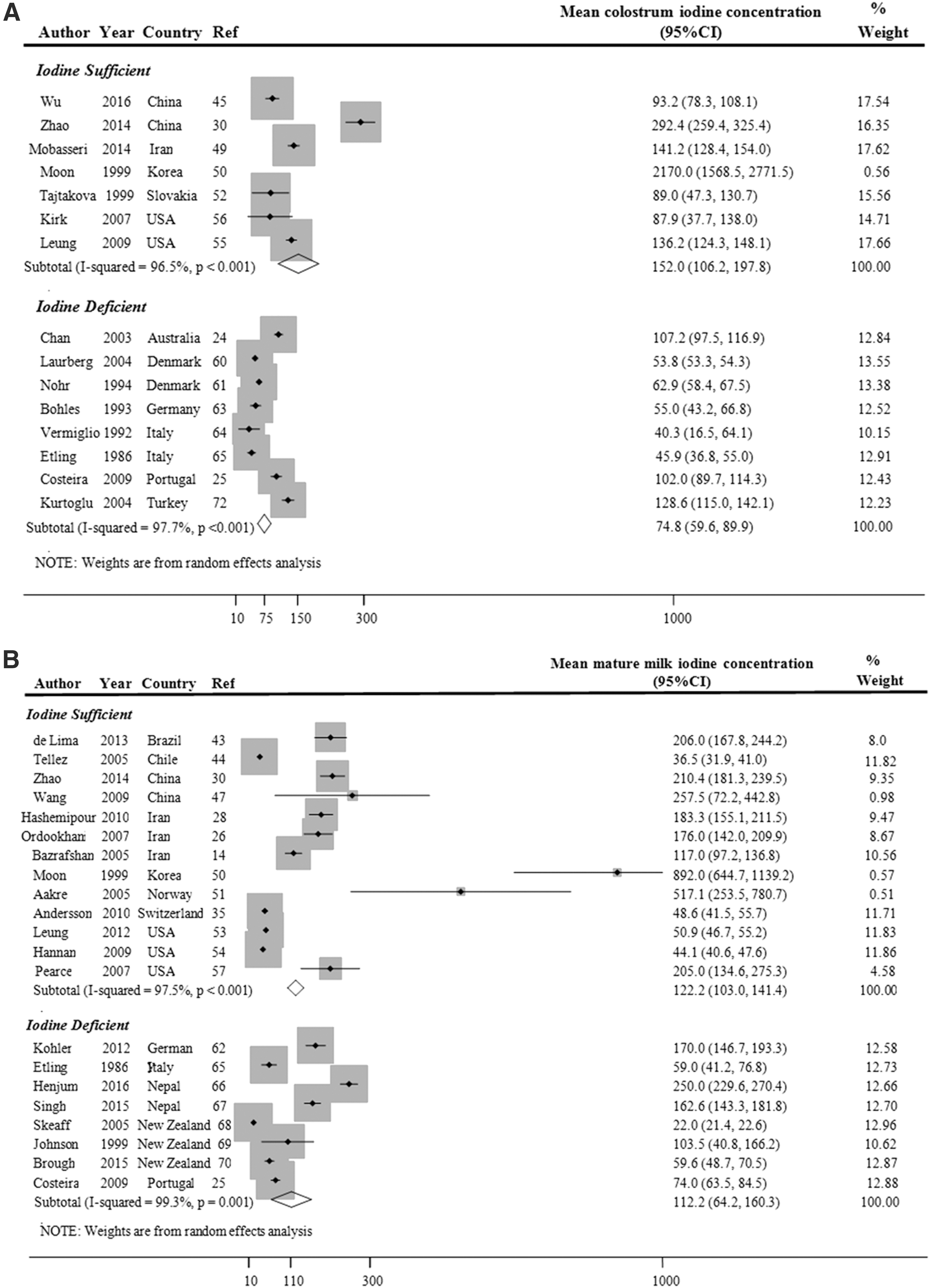
The Forest plot, with mean values and CIs, and the pooled estimates for the mean iodine concentrations in the colostrum of lactating mothers residing in iodine-sufficient and -deficient countries are illustrated in Figure 2A. This plot revealed substantial heterogeneity between the study-specific estimates (test for heterogeneity: I 2 = 96.5% and 97.7%, respectively; p < 0.001 for both), and hence the random-effect model was considered to provide a more appropriate estimate. The mean iodine concentrations of colostrum were higher in mothers residing in iodine-sufficient countries compared to those in iodine-deficient countries, and a comparison of the CIs revealed a significant difference between the two iodine states (152.0 μg/L [CI 106.2–198.7 μg/L] vs. 74.8 μg/L [CI 59.6–89.9 μg/L]). Following the use of the trim and fill method to correct publication bias in the iodine-deficient subgroup (p = 0.081), the mean iodine concentration of colostrum in mothers residing in iodine-deficient countries was 57.8 μg/L [CI 41.4–74.1 μg/L]. This difference between the two iodine status subgroups remained statistically significant, even after bias correction.
(
Iodine concentrations of mature milk samples in lactating mothers residing in iodine-deficient versus -sufficient countries
In Figure 2B, the Forest plot depicts studies with mean values and CIs, as well as the pooled estimates for the mean iodine concentrations of mature milk in mothers residing in countries with a different iodine status. The study-specific estimates exhibited substantial heterogeneity between studies (I 2 = 97.5% and 99.3%, respectively; p < 0.001 for both). The mean iodine concentrations of mature milk samples from lactating mothers residing in iodine-sufficient and -deficient countries were 122.2 μg/L [CI 103.0–141.4 μg/L] and 112.2 μg/L [CI 64.2–160.3 μg/L], respectively, and a comparison of the CIs found no significant difference. Here, publication bias in both subgroups (p = 0.007) was corrected using the trim and fill method, and the subsequent mean iodine concentrations in mature milk from iodine-sufficient and -deficient countries were adjusted to 71.5 μg/L [CI 51.0–92.0 μg/L] and 28.0 μg/L [CI −13.8 to 69.9 μg/L], respectively. Again, this difference was not statistically significant.
Taken together, the weighted iodine levels [CIs] in colostrum and mature milk samples from mothers in iodine-sufficient countries were 152.0 μg/L [CI 106.2–198.7 μg/L] and 71.5 μg/L [CI 51.0–92.0 μg/L], respectively, whereas the corresponding values in iodine-deficient countries were 57.8 μg/L [CI 41.4–74.1 μg/L] and 28.0 μg/L [CI −13.8–69.9 μg/L], respectively. In iodine-sufficient countries, a significant difference was found between the iodine levels in colostrum and mature milk samples.
Iodine nutrition status of breast-fed and formula-fed infants in iodine-sufficient versus -deficient countries
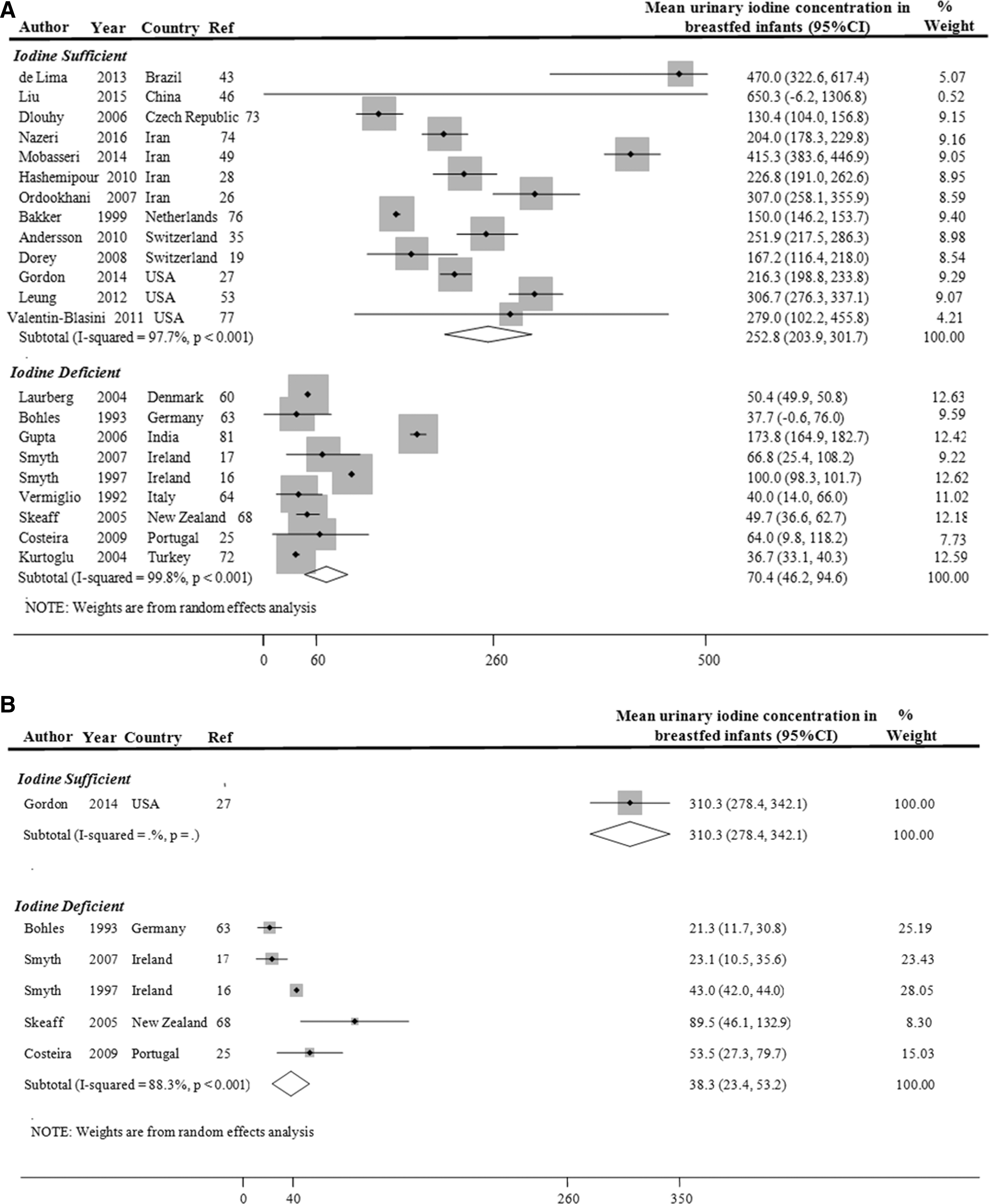
The pooled UICs [CIs] of breast-fed infants in iodine-sufficient and -deficient countries are given in Figure 3A. Substantial heterogeneity was observed between the two subgroups of studies (I 2 = 97.7% and 99.8%, respectively; p < 0.001 for both). The mean UICs of infants living in iodine-sufficient and -deficient countries were 252.8 μg/L [CI 203.9–301.7 μg/L) and 70.4 μg/L [CI 46.2–94.6 μg/L], respectively, and a comparison of the CIs revealed a significant difference between these values. After publication bias in the iodine sufficient subgroup (p = 0.008) was corrected using the trim and fill method, the mean UIC in iodine-sufficient countries was corrected to 164.5 μg/L [CI 116.4–212.7 μg/L]. However, the difference between the two subgroups remained statistically significant.
(
As shown in Figure 3B, the mean values and CIs and the pooled estimates of UICs of formula-fed infants living in iodine-sufficient countries were significantly higher than those of infants in iodine-deficient countries (310.3 μg/L [CI 287.4–342.1 μg/L] vs. 38.3 μg/L [CI 23.4–53.2 μg/L]). However, the sample size from iodine-sufficient countries was small, and the results may therefore be inconclusive. Generally, however, the UICs [Cis] of breast-fed and formula-fed infants in iodine-sufficient countries were 164.5 μg/L [CI 116.4–212.7 μg/L] and 310.3 μg/L [CI 287.4–342.1 μg/L], respectively, whereas the corresponding values in iodine-deficient countries were 38.3 μg/L [CI 23.4–53.2 μg/L] and 70.4 μg/L [CI 46.2–94.6 μg/L], respectively.
Discussion
The present systematic review and meta-analysis is the first to explore the BMICs and infant iodine statuses in iodine-deficient and -sufficient countries. In the current study, meta-analysis of the available studies indicates that the mean breast-milk iodine concentrations at two different stages of lactation (i.e., colostrum and mature milk) ranged between 71.5 and 152.0 μg/L among mothers residing in iodine-sufficient countries, and between 28.0 and 57.8 μg/L among mothers in iodine-deficient countries. Furthermore, despite the small sample of formula-fed infants residing in iodine-sufficient countries, the findings reveal that the UICs of both breast-fed and formula-fed infants in iodine-sufficient countries were significantly higher than those of infants in iodine-deficient countries. Interestingly, significant differences in infant UICs were not observed with respect to feeding type (breast-feeding vs. formula feeding) in either iodine-sufficient or -deficient countries.
Breast-milk iodine concentration as a reliable indicator of the infant iodine status
In their latest recommendation (15), WHO/ICCIDD/UNICEF proposed a median UIC of >100 μg/L as indicative of iodine sufficiency in both lactating mothers and breast-fed infants. These UICs are lower than the daily iodine requirements of 290 and 250 μg recommended by current dietary allowances and the WHO, respectively, because iodine is excreted in breast milk. However, several studies have reported a discrepancy between the maternal UIC and BMIC (14,23 –26), suggesting that the former may not truly reflect the iodine status of a breast-fed infant. By contrast, however, some studies have reported a positive association between the infant UIC and maternal BMIC (27 –29). However, there is insufficient evidence to confirm the reliability of BMIC as an indicator of the iodine status of an infant.
Mineral analyses of breast milk have found that the patterns of trace elements differ markedly among different stages of lactation (30), and a few studies have suggested that BMICs tend to be higher during the first few days postpartum, followed by a decrease over time. In a study by Chierici et al., a decline in the BMIC was reported over a 90-day period postpartum, with values ranging from 270 μg/L at 3 days to 150 μg/L at 30 days and 110 μg/L at 90 days (31). A similar pattern was observed in a study conducted in New Zealand, which reported a 40% decrease in the BMIC during the first six months postpartum (32). Consistent with these earlier studies, the present findings demonstrate that the iodine levels were significantly higher in colostrum than in mature breast-milk samples collected in iodine-sufficient countries; by contrast, no significant difference between these types of breast milk were observed in iodine-deficient countries. Given the broad range of BMICs in countries with different iodine states (6 –9), no consensus has been reached regarding the optimal cutoff value indicative of a sufficient BMIC. In the current meta-analysis, iodine concentrations of 152.0 μg/L [CI 106.2–198.7 μg/L] and 71.5 μg/L [CI 51.0–92.0 μg/L] in colostrum and mature breast milk, respectively, were accompanied by iodine sufficiency among breast-fed infants residing in iodine-sufficient countries. The findings are compatible with a recent study by Dold et al., which suggested a BMIC reference range of 60–465 μg/kg as indicative of an adequate iodine status in both lactating mothers and breast-fed infants in iodine-sufficient populations (33).
Infant UIC as a criterion indicative of infant iodine status
The main challenges encountered when determining the median UIC in young children are the difficulty of sample collection and a small, non-representative sample size. Hence, sufficient urinary iodine data are lacking in this age group, and the best criteria for assessing the degree of iodine deficiency in this age group remain to be established. The WHO recommends a median UIC >100 μg/L when assessing the iodine status of infants younger than two years of age (15). The results reveal that in iodine-sufficient countries, the UICs of either breast-fed or formula-fed infants ranged between 164.5 μg/L [CI 116.4–212.7 μg/L] and 310.3 μg/L [CI 287.4–342.1 μg/L], whereas these values ranged between 38.3 μg/L [CI 23.4–53.2 μg/L] and 70.4 μg/L [CI 46.2–94.6 μg/L] in iodine-deficient countries. Although almost all reports from the latter countries reported median UICs in full-term infants of <100 μg/L (34), Dorey et al. (19) reported the following median UICs in infants younger than two years of age from iodine-sufficient countries: Canada (n = 81), 148 μg/L; Netherlands (n = 64, n = 36), 162 and 150 μg/L, respectively; Sweden (n = 39, n = 61), 112 and 96 μg/L, respectively; Switzerland (n = 237), 62–70 μg/L; and Czech Republic (n = 181), 92–109 μg/L. In other words, the iodine intakes of some infants may be suboptimal, even in countries classified as iodine sufficient.
Type of feeding and infant iodine status
The supply of iodine to a neonate or infant and the corresponding iodine status is entirely dependent upon the iodine content of breast milk and/or formula. Despite the importance of iodine intake during these critical periods, few studies have compared the iodine nutrition statuses of breast-fed and formula-fed infants, and the existing studies have reported inconclusive results. For instance, in the United States, similar iodine statuses were observed among infants who were exclusively breast-fed, exclusively formula-fed, or mixed fed (27). However, in China and Ireland, the median UIC of infants who were exclusively formula-fed was significantly lower than that of infants who were exclusively breast-fed, emphasizing the greater bioavailability of iodine in breast milk compared to formula (16,29). Another study conducted in Switzerland, which is considered iodine sufficient, indicated that infants fed with both breast milk and formula had higher UICs than did those who were exclusively breast-fed, and this result was attributed to higher iodine concentrations in infant formula relative to breast milk (35). However, the results of the current meta-analysis suggest that different feeding methods had no significant effects on the UICs of infants residing in either iodine-sufficient or -deficient areas.
Iodine supplementation to ensure iodine sufficiency among infants
To ensure adequate iodine intake during pregnancy and infancy, the American Thyroid Association and the Endocrine Society recommend that pregnant and lactating women ingest 150 μg of iodine in daily vitamin/mineral supplements (36,37). However, the present results indicate that the UICs of both breast-fed and formula-fed infants born in iodine-sufficient countries were within optimal levels, and this finding is compatible with the WHO/ICCIDD/UNICEF statement that pregnant and lactating mothers and infants younger than two years if residing in countries with effective and sustained salt iodization programs do not require iodine supplements (38). It is further noted that the thyroid glands of fetuses and newborns are more susceptible than those of adults to the inhibitory effects of high iodine doses, leading to concerns of vulnerability to excessive iodine exposure. Thyroid disturbances, (e.g., subclinical and overt hypothyroidism) have been reported in some studies of newborn and infants exposed to excessive iodine intake (39). For instance, in Japan and China, a transient increase in thyrotropin levels was observed in some neonates born to mothers who consumed iodine-rich foods (e.g., seaweed, kelp) and who drank water during pregnancy or lactation (40,41). In a study in Nepal, prevalence rates of 7.4% for subclinical hypothyroidism and <1% for overt hypothyroidism were reported among infants aged 6–24 months who were exposed to excessive iodine intake (42). Therefore, the amount of iodine stored in the infant thyroid at birth, when added to the iodine intake via breast milk, is likely sufficient to meet a child's iodine requirements for at least the first six months of life, and possibly the first 24 months.
The main strength of the present study is its designation as the first systematic review and meta-analysis to evaluate the iodine levels in breast milk collected during two stages of lactation, as well as the iodine statuses of breast-fed and formula-fed infants residing in iodine-sufficient or -deficient countries. However, some of the infant subgroup sample sizes were small, and may not have provided reliable estimations of the iodine status. In the current meta-analysis, studies reporting maternal or infant iodine fortification or supplementation were excluded, but note that some studies did not mention this factor. Another potential limitation is related to the existence of several factors that may influence the BMIC and infant UIC, such as the maternal iodine status, recent maternal iodine intake, length and stage of lactation, time of sampling (i.e., fore-, mid-, and hind-milk samples). These factors may have been the source of heterogeneity observed across the included studies. Given the small sample size of studies within different subgroups, however, the source of heterogeneity could not be determined using a meta-regression analysis. Lastly, the limited number of studies implies it was not possible to include the above-mentioned influential issues in the analysis, which makes the interpretation of the results difficult.
In conclusion, the findings of the meta-analysis reveal that the iodine concentrations detected in colostrum and mature breast-milk samples from iodine-sufficient countries indicated the provision of adequate iodine to breast-fed infants residing in these countries. Although an effect of the type of feeding on the iodine statuses of infants residing in either iodine-sufficient or -deficient countries was not observed, both breast-fed and formula-fed infants in the former countries had significantly higher UICs. However, these data should be interpreted cautiously, given the limited number of studies of urinary iodine levels in formula-fed infants, particularly in iodine-sufficient countries. Finally, the findings confirm the WHO/ICCIDD/UNICEF declaration that the iodine intakes in countries with effective and sustained salt iodization programs are generally sufficient to meet iodine requirements, and hence pregnant and lactating women and infants younger than two years of age do not require iodine supplementation. However, further investigation of this subject is recommended.
Footnotes
Acknowledgments
This study was supported by a financial grant from the Research Institute of Endocrine Sciences, Shahid Beheshti University of Medical Sciences.
Author Disclosure Statements
None of the authors has any personal or financial conflicts of interest.