
Abstract
Background:
Nationwide, the incidence of thyroid cancer is lower among American Indian/Alaska Native (AI/AN) people than among U.S. whites (USW). However, little is known about the incidence of thyroid or other endocrine cancers specifically among Alaska Native (AN) people.
Methods:
Data were examined from the National Cancer Institute's Surveillance, Epidemiology, and End Results Alaska Native Tumor Registry on endocrine cancers diagnosed among AN people from 1969–2013, with a specific focus on thyroid cancers. Frequencies of endocrine cancers by site and also of thyroid cancers by histology, size, and stage at diagnosis were evaluated. Distributions were compared to USW (Surveillance, Epidemiology, and End Results 9 Registries) using the chi-square test. Five-year average annual age-adjusted incidence rates of thyroid cancers were calculated, stratified by histology, age, and five-year period of diagnosis, and compared to those observed among USW. Five-year cause-specific survival was evaluated using cause of death data from the National Death Index Plus from the National Center for Health Statistics.
Results:
During the 45-year period (1969–2013), 224 endocrine cancers were diagnosed among AN people, of which 210 (94%) were thyroid cancers. Compared to USW, AN people were diagnosed at a slightly younger age, had a higher proportion of thyroid cancers diagnosed with a size of 20–40 mm, and a larger proportion of patients with regional metastases. More than 85% of AN thyroid cancers were of papillary histology. The incidence of thyroid cancers was similar between AN people and USW, and appeared to increase among AN people over the period of surveillance. Finally, five-year cause-specific survival rate was 100% for papillary carcinoma patients and 86.3% [confidence interval 54.7–96.5] for follicular thyroid cancer patients.
Conclusions:
This study is the first report of endocrine cancers and the first detailed examination of thyroid cancer among AN people. The incidence of thyroid cancer was similar among AN people and USW. However, compared to USW, AN people appear to be at risk for diagnosis at a younger age, larger size, and higher stage. Further research is needed to explore the causes of these differences.
Introduction
T
Endocrine cancers were examined among AN patients recorded by the Alaska Native Tumor Registry (ANTR), with a specific focus on thyroid cancers. The goals of this analysis were to describe the epidemiology of endocrine cancers among AN people. For thyroid cancers, characteristics examined included patient and tumor characteristics, stage of disease at time of diagnosis, and survival. Finally, the study sought to describe trends over time in incidence of thyroid cancer among AN people.
Methods
The ANTR was used to identify all cases of endocrine cancers diagnosed during the 45-year period between January 1, 1969, and December 31, 2013. The ANTR is a population-based central cancer registry that records cancer information on AI/AN people who meet eligibility requirements for Indian Health Service benefits, and who were resident in the state of Alaska at the time of their cancer diagnosis. Because almost 90% of AI/AN people residing in the state of Alaska identify as AN (11,12), hereafter, all patients recorded in the ANTR are referred to as AN. The ANTR has been collecting cancer information according to National Cancer Institute (NCI)'s Surveillance, Epidemiology, and End Results Program (SEER) standards since its inception, and it has been a full member of the SEER Program since 1999. Institutional Review Board approval and informed consent were not required for the current study because SEER Program data are publicly available and all surveillance data were de-identified. Appropriate tribal review was obtained for publication of this study.
As part of the ANTR's standard surveillance process, cases were identified through a variety of sources, including tumor registry and pathology files of the Alaska Native Medical Center and other Native and non-Native healthcare facilities throughout the state, linkage to the Alaska State Cancer Registry and the Washington State Cancer Registry, and death certificates (<1% cases). The registry collects information on patient demographics, primary cancer site, histology, tumor size, basis of confirmation of the diagnosis, treatment, and vital status. Stage at diagnosis was defined using the SEER Summary Stage 2000 variable (local, regional, distant) (13). Summary Stage 2000 and tumor size variables were available only for the period 2004–2013. Cause of death data were obtained from the National Death Index Plus from the National Center for Health Statistics.
Classification of cancer site of origin, histologic cell type, behavior, and grade coding followed the International Classification of Diseases for Oncology (ICD-O) second and third editions (14). Cancers coded as arising from the thyroid (C73.9) and other endocrine sites (C37.9, C74.0–74.9, C75.0–75.9) were selected for inclusion in this study. Only invasive malignancies are described (behavior code 3); benign and in situ tumors were excluded from this analysis (ICD-O behavior codes 0 and 2, respectively), as were tumors of uncertain or unknown behavior (ICD-O behavior code 1). More than 99% of cases were histologically confirmed. Thyroid cancers were further classified by histology: papillary (8050, 8260, 8340, 8341, 8342, 8343, 8344), follicular (8290, 8330, 8331, 8335), medullary (8510, 8512), anaplastic (8021), and other (8190, 8430). Although Nikiforov et al. have recently proposed reclassifying noninvasive encapsulated follicular variant of papillary thyroid cancer as noninvasive follicular thyroid neoplasm with papillary-like nuclear features (15), all cases were retained in the present study, since all cases were diagnosed before the proposed reclassification.
Statistical methods
Cancer rates and counts for AN people were compared to USW rates from the SEER Program's SEER*Stat database, based on nine registries (five states: CT, HI, IO, NM, UT; four metropolitan areas: Atlanta, Detroit, San Francisco, and Seattle) (16). Data from the SEER 9 Registries were available only for the years 1973–2013. Cancer incidence rates were expressed as average annual rates over five-year periods, expressed per 100,000 population and age-adjusted to the U.S. Census 2000 standard population using the direct method. Denominators for rate calculations were derived from population estimates from the U.S. Bureau of the Census and National Center for Health Statistics for AN people (bridged estimates) and USW, available from the NCI's SEER Program (17). Incidence rates, confidence intervals (CI), and cause-specific survival measures were calculated using version 8.3.2 of the SEER*Stat software (
Results
During the period 1969–2013, there were 224 malignant endocrine cancers diagnosed among AN people (Table 1), of which 94% (210) were thyroid cancers. Other sites included the adrenal gland (n = 11), the thymus (n < 5), and the pineal gland (n < 5). The distribution of endocrine cancers by site was not statistically different between AN people and USW (p = 0.54). The mean age (SD) at diagnosis for AN people was 43.5 (17.5) years, and the mean age (SD) at diagnosis for USW was 48.2 (17.5) years (p < 0.001). More than 75% of AN endocrine cancers were diagnosed among women. The sex distribution of endocrine cancers was not significantly different between AN people and USW (p = 0.17).
Data for AN people are from the SEER Alaska Native Tumor Registry for the period 1969–2013.
Data for USW are from the SEER 9 Registries for the period 1973–2013.
ICD-O-3 codes: thymus (C37.9), thyroid (C73.9), adrenal gland (C74.0, C74.1, C74.9), parathyroid gland (C75.0), pituitary gland (C75.1), pineal gland (C75.3), other endocrine (C75.2, C75.4, C75.5, C75.8, C75.9).
AN, Alaska Natives; USW, U.S. whites; SEER, Surveillance, Epidemiology, and End Results Program.
As thyroid cancers accounted for the vast majority of endocrine malignancies, the rest of the analyses focused only on these cancers. More than 80% of thyroid cancers in AN people were diagnosed among women (Table 2), and the distribution of thyroid cancers by sex was not different between AN people and USW (p = 0.058). The mean (SD) age at diagnosis was 44.2 (17.5) years, which was slightly lower than that observed among USW (48.4 [16.6] years; p = 0.0002). Size distribution was different between AN people and USW (p = 0.030). AN people had a smaller proportion sized <10 mm and a larger proportion sized 20–40 mm. Stage distribution was also different between AN people and USW (p = 0.027). Compared to USW, AN people had a lower proportion of thyroid cancers diagnosed limited to the thyroid (local disease) and a higher proportion of cases with lymph node involvement (regional disease).
Data were compared using the Wilcoxon rank-sum test (means) and the Mann–Whitney U-test (medians) or the chi-square test for categorical variables.
Data for AN people are from the SEER Alaska Native Tumor Registry for the period 1969–2013.
Data for USW are from the SEER 9 Registries for the period 1973–2013.
Tumor size and Summary Stage 2000 variables only available for cases diagnosed 2004–2013 (AN and USW).
SD, standard deviation; IQR, interquartile range.
The distribution of thyroid cancers by histologic type was different among AN people compared to USW (p < 0.001). The vast majority (85%) of AN thyroid cancers were papillary (n = 180), followed by 11% follicular (n = 23). Few undifferentiated tumors were observed, with only 1% medullary cancers (n < 5), 0% anaplastic (n < 5), and 2% “other” (n < 5). Due to small cell sizes for undifferentiated cancers, the distribution of differentiated (papillary and follicular cancers) only between AN people and USW were also compared. Here, no statistically significant difference was found (p = 0.53). The distribution of thyroid cancers by stage and histology is given in Table 3. Stage distribution only differed between AN people and USW for papillary cancers (p < 0.0001). A lower proportion of papillary cancers limited to the thyroid and a higher proportion diagnosed with regional lymph node involvement among AN people were observed compared to USW.
Information is only given for papillary and follicular histologies due to the small case numbers of medullary and anaplastic cases.
Table 4 gives age-specific incidence rates for thyroid cancers diagnosed among AN people between 1973 and 2013 stratified by sex and shown compared to USW. Although data were available for AN people from 1969 to 2013, SEER 9 data are only available from 1973 to 2013. So, analyses presented in Tables 4 and 5 were restricted to this time period to ensure comparability of rates. The incidence of thyroid cancers increased with age for both men and women. However, this pattern was more pronounced among men. The incidence of thyroid cancer was typically lower among AN people than it was among USW at all ages. The exception to this was females aged >80 years, where the rate was slightly higher among AN women. However, due to the large CI around the AN estimate, this difference was not statistically significant.
Rate is not given where <5 cases diagnosed.
CI, confidence interval.
Rate is not given where <5 cases diagnosed.
Trends in five-year average annual thyroid cancer incidence among AN people stratified by sex are shown in Figure 1 and Supplementary Table S1. It was not possible to analyze trends by histology due to small numbers of case counts for all histologies except papillary, which were very similar to those of total thyroid cancers. Five-year average annual incidence rates were fairly steady between 1969–1973 and 1994–1998, after which time incidence increased, almost doubling between 1999–2003 and 2009–2013. Over the course of the 45-year period of surveillance, the incidence increased from 4.4 [CI 2.1–9.2] per 100,000 (1969–1973) to 13.7 [CI 10.3–17.7] per 100,000 (2009–2013). Rates were different between the beginning and end of the 45-year time period, but not between intermediate time periods. The pattern was very similar among USW: the five-year average annual incidence remained similar from 1974–1978 to 1994–1998, after which time incidence began to increase, almost doubling between 1999–2003 and 2009–2013.
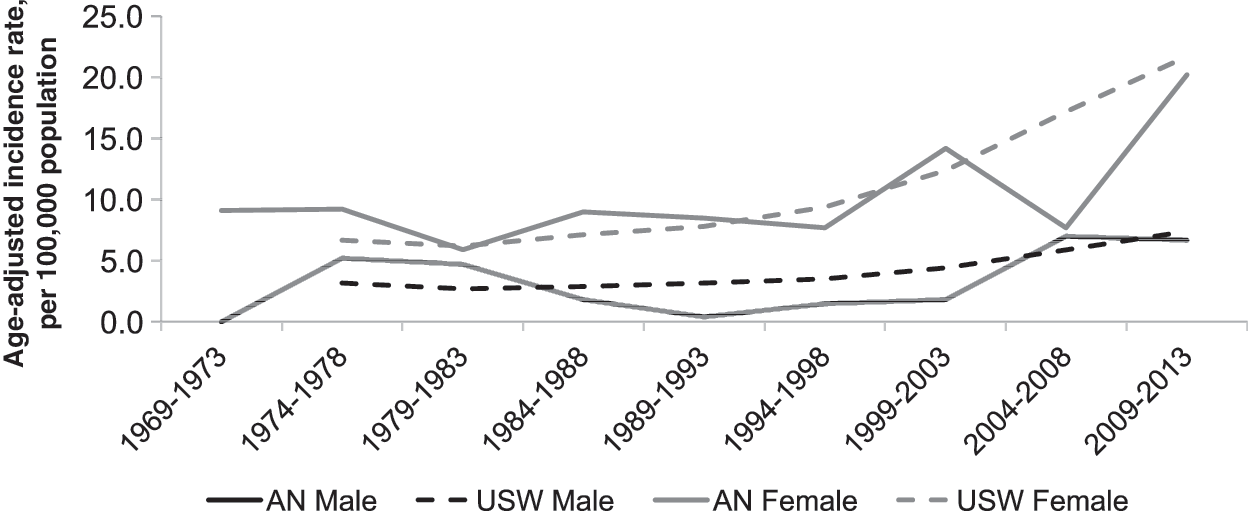
Trends in incidence of thyroid cancer, stratified by sex, among Alaska Native people (1969–2013) and U.S. whites (1973–2013).
Table 5 gives the age-adjusted incidence rates for thyroid cancers stratified by histology and sex among AN people and compared to USW for the period 1973–2013. The incidence of thyroid cancer was higher among AN females (11.3 [CI 9.5–13.3] per 100,000) compared to males (3.6 [CI 2.5–5.1] per 100,000). These rates were similar to those observed among USW. When stratified by histology, the highest rates were observed for papillary cancers, as expected (6.4 [CI 5.4–7.5] per 100,000), followed by follicular cancers (0.9 [CI 0.5–1.5] per 100,000). Due to small numbers of cases (n < 5), rates for medullary and anaplastic cancers were not calculated for AN people.
Finally, cause-specific survival was examined among thyroid cancer patients diagnosed 1992–2013. During this period, five-year cause-specific survival was 100% for those with papillary cancers and 86.3% [CI 54.7–96.5] for those with follicular cancer. Because of the small number of medullary and anaplastic cancers (n < 5), survival was not examined among these patients.
Discussion
This study is the first to describe endocrine and thyroid malignancies specifically among AN people. It presents information on all such cancers diagnosed 1969–2013. As among USW, the vast majority of endocrine cancers diagnosed among AN people were located in the thyroid. Compared to USW, thyroid tumors among AN people occurred at a slightly younger age, and tended toward a larger size at diagnosis, with a larger proportion sized 20–40 mm versus <10 mm. Also, a larger proportion of thyroid malignancies among AN people were diagnosed at regional versus local stage compared to USW. Incidence of total thyroid cancer, as well as papillary and follicular thyroid histologies, was similar among AN people and USW, while the number of medullary and anaplastic cancer cases was too small among AN people to calculate incidence rates reliably, despite the long period of surveillance. Thyroid cancer trends were also examined. Five-year average thyroid cancer incidence rates more than tripled over the 45-year period between 1969 and 2013. Similar increases were observed among USW and have been previously reported nationwide (5,19,20). Finally, survival from thyroid malignancies was examined, noting that similar to observations among USW (4), five-year cause-specific survival was high at 100% and 86.3% for papillary and follicular malignancies, respectively, during the period 1992–2013.
Sparse data have previously been available on the incidence and clinical characteristics of endocrine and thyroid cancers specifically among AN people. The present data indicate that the incidence of thyroid cancers, including papillary and follicular subtypes, was similar among AN people and USW, but that a higher proportion of thyroid cancers among AN people were diagnosed at a slightly younger age, and a more advanced size and stage. Previously published data, also using data from the NCI's SEER program, suggest that thyroid cancer incidence and clinical characteristics do vary by racial/ethnic groups, and that incidence may be lower among the combined AI/AN population than USW. For example, one recent study reported a 23% and 20% lower incidence of thyroid cancer among AI/AN men and women, respectively, relative to USW, although the difference was only statistically significant for females (2). To the authors' knowledge, there has been no published study comparing clinical characteristics of thyroid cancer diagnoses among AI or AN people to those of USW or other racial/ethnic groups. Thus, despite small case numbers, these data provide information on clinical characteristics of thyroid cancers among AN people that were previously unreported.
Several studies have examined differences in thyroid cancer incidence trends by race and ethnicity (7,20,21). The largest increases in incidence have been observed among non-Hispanic whites (average annual percent change [AAPC] 5.6% per year), with the lowest among Hispanic whites (AAPC 3.3% per year), AI/AN people (AAPC 3.2% per year), and Asian/Pacific Islanders (AAPC 2.3% per year) (7). Unfortunately, the small case numbers in this study these analyses from being recreated with confidence for AN people. However, the data do show a substantial increase in incidence over the 45-year period of surveillance. A possible explanation for this finding among this relatively remote-living population is an increase in access to care over past decades. Specifically, improvements in the ease of in-state transportation, as well as access to specialty care at the Alaska Native Medical Center, may have resulted in the detection of a reservoir of previously undiagnosed disease. Furthermore, some studies have concluded that the national increase in thyroid cancer incidence reflects increased detection of very small (<1 cm) cancers (19). Yet, more recent data showing increases in both papillary thyroid cancer incidence and mortality suggest a true increase in the burden of this disease (6). Unfortunately, due to small case counts, it was not possible to determine whether the increase in thyroid cancer incidence among AN people was due to small, subclinical tumors or larger, clinically relevant cancers.
As discussed above, it is possible that increases in the detection of small, subclinical thyroid cancers observed nationally may be a result of improved detection methods (22,23). This phenomenon, termed “overdiagnosis,” may be especially prevalent among USW who are more likely to be insured, with easy access to care, than their black, Hispanic, Asian Pacific Islander, and AI/AN counterpart (24,25). In theory, all individuals included in this study have access to healthcare through the Alaska Tribal Health System. Yet, in practice, ease of access to medical services, including care that may result in thyroid cancer detection and diagnosis, is likely to vary with location of residence in Alaska. Although ease of in-state transportation and access to in-community physicians, nurse practitioners, and physician assistants has increased over the period of surveillance, many AN people still have to travel, often by small plane or boat, for such medical care. This may decrease the potential for overdiagnosis and/or contribute to possible late or “under-diagnosis,” which would be consistent with the finding that a larger proportion of thyroid cancers diagnosed among AN people were of larger size and diagnosed at higher stage relative to that observed among USW. Importantly, despite this potential delay in diagnosis, the incidence of papillary and follicular histologies was similar to that among USW, the proportion of cancers diagnosed at “distant” stage was similar among AN people and USW, and five-year cause-specific survival among AN people was as high as that observed in previous national reports (26). Other potentially contributing factors to the differences observed between AN people and USW include differences in the burden of other thyroid diseases that may contribute to the etiology of these malignancies, as well as differences in the distribution of other life-style, environmental, and genetic risk factors. Further research is needed to examine the cause of these differences in clinical presentation among AN people.
The primary limitation of this study is the small number of thyroid cancer cases diagnosed among AN people, even during the long period of surveillance (45 years). This limitation was particularly important for subgroup analyses, for example by histology, where incidence rates for medullary and anaplastic cancers were not calculated due to small case numbers. In addition, CIs around the incidence estimates were sometimes wide, which limited the ability to detect statistically significant differences between groups or over time. Finally, the small sample size substantially limited the analysis of trends in thyroid cancer incidence. Combining multiple years of data is often required to produce more reliable estimates in small populations (27). However, despite data aggregation over time, the five-year incidence estimates remained variable, which minimized the ability to detect any short-term changes in trends. Furthermore, although it was possible to see a distinct change in thyroid cancer incidence among AN people over the entire 45-year period, it was not possible to assess trends formally with methods such as the Joinpoint Regression Program.
This study describes the clinical characteristics and incidence patterns for endocrine and thyroid cancers among AN people and how these patterns compare to those reported for USW. Very little information has previously been described regarding these malignancies among AI/AN populations. Therefore, this study provides much-needed data on this underserved minority population. It is anticipated that these data will be of interest to those involved in clinical care and disease prevention among AI/AN people, as well as to those with a general interest in thyroid cancer.
Footnotes
Acknowledgments
The Alaska Native Tumor Registry is supported by the NCI's Surveillance, Epidemiology, and End Results Program, NCI contract number HHSN26120130010I, Task Order HHSN26100005.
Author Disclosure Statement
No competing financial interests exist.