
Abstract
Objectives:
To determine the impact of subclinical hypothyroidism (SCH) on the risk of cardiovascular disease (CVD) and all-cause mortality, a comprehensive meta-analysis was performed according to the age or coexisting CVD risk status of the participants.
Methods:
Studies regarding the association of SCH with all-cause mortality from PubMed and Embase databases were included. The pooled relative risk (RR) of CVD and all-cause mortality was calculated using the Mantel–Haenszel method. A subgroup analysis of participants with high CVD risk was conducted, including history of coronary, cerebral, or peripheral artery disease; dilated cardiomyopathy; heart failure; atrial fibrillation; venous thromboembolism; diabetes mellitus; or chronic kidney disease.
Results:
In total, 35 eligible articles incorporating 555,530 participants were included. SCH was modestly associated with CVD and all-cause mortality (RR for CVD = 1.33 [confidence interval (CI) 1.14–1.54]; RR for all-cause mortality = 1.20 [CI 1.07–1.34]). However, the association was not observed in participants aged ≥65 years. Subgroup analysis showed that participants with SCH and high CVD risk showed a significantly higher risk of all-cause mortality (RR for CVD = 2.20 [CI 1.28–3.77]; RR for all-cause mortality = 1.66 [CI 1.41–1.94]), whereas those with SCH and low CVD risk did not. Additional subgroup analysis of six studies with a mean participant age of ≥65 years and high CVD risk showed a significant high risk of all-cause mortality in the SCH group (RR = 1.41 [CI 1.08–1.85]; I 2 = 0%).
Conclusions:
SCH is associated with an increased CVD risk and all-cause mortality, particularly in participants with high CVD risk.
Introduction
S
Therefore, an updated comprehensive meta-analysis was performed to clarify the association of SCH with CVD with all-cause mortality according to the age of participants as well as the presence of CVD risk.
Materials and Methods
Search strategy
This meta-analysis follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Checklist (19). A literature search of PubMed and Embase databases was conducted from their inception (January 1, 1990) to November 26, 2017. Two independent investigators (S.M. and M.J.K.) selected articles with a combination of the following relevant terms: “subclinical,” “thyroid,” “hypothyroidism,” “cardiovascular disease,” “heart failure,” “myocardial infarction,” and “mortality.” Only articles published in English were considered.
Study selection
The literature search yielded 2781 potentially relevant articles, of which 238 were screened for further review after excluding duplicate studies (n = 498) or those with a different topic of interest (n = 2045). If studies had multiple reports, the latest or most complete article was used. All articles were electronically downloaded and screened for inclusion using a two-step method. After evaluation of the titles and abstracts according to predefined criteria, 189 articles were further excluded for the following reasons: (i) there was no information on TSH, fT4, or all-cause mortality; (ii) the study was published in the form of an abstract, expert opinion, letter, conference article, or review; or (iii) it was not a cohort study. Subsequently, the full texts of 49 selected articles were reviewed by two independent investigators (S.M. and M.J.K.), and any disagreement was resolved by a third investigator (Y.J.P.). Because the data of 14 of these articles were insufficient for the analysis, 35 articles were finally selected for the meta-analysis (Supplementary Fig. S1; Supplementary Data are available online at
Data extraction and quality assessment
The following variables were independently extracted by the two investigators based on the same rules: first author, publication year, country, number and characteristics of study participants, number of men and women, mean age, coexisting diseases potentially associated with CVD risk, follow-up duration, and mortality. All disagreements were discussed with the third investigator. The Newcastle–Ottawa Scale (NOS) was applied to evaluate the methodological quality of the eligible studies. Accumulated scores ranged from 0 to 9 points; scores from 6 to 9 points were considered to suggest high quality, thus representing a lower risk of bias.
Data analyses and statistical methods
The pooled relative risks (RR) with confidence intervals (CIs) were calculated using the Mantel–Haenszel method. The Higgins' I 2 statistic was used to test for heterogeneity. When I 2 was ≤50%, the included studies were considered to have little heterogeneity, and a fixed-effects model was used. When I 2 was ≥50%, the included studies were considered to have significant heterogeneity, and a random-effects model was used. The potential for publication bias was assessed using a funnel plot analysis. To examine the strength of the outcome, a sensitivity analysis was conducted. Subgroup analyses were used to determine the cause of heterogeneity stratified by age (cutoff 65 years) and CVD risk. High CVD risk was defined as the presence of any disease that could increase CVD risk, including history of coronary, cerebral, or peripheral artery disease; dilated cardiomyopathy; heart failure; atrial fibrillation; venous thromboembolism; diabetes mellitus; or CVD risk factors based on the World Health Organization criteria (20). Participants with chronic kidney disease were also classified as a high CVD risk group based on the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines (21). Population-based studies of the general population were classified as having a subgroup with low CVD risk because they included mainly healthy participants.
All statistical analyses were performed using the statistical program R v3.1.0 (
Results
Characteristics of selected studies
In total, 35 articles underwent meta-analysis (14 –18,22 –51), and their main characteristics are summarized in Table 1. In total, 555,530 participants were enrolled, and 21,176 (mean 5.7%; range 1.6–28.8%) had SCH. Sample sizes of these studies ranged from 229 to 228,357 participants. Among them, 14 studies showed a mean age of <65 years, and 18 had a mean age of ≥65 years. Three studies reported age-based subgroup data with a cutoff age of 65 years (29,34,35). A total of 11 studies were defined as studies with participants at high CVD risk based on predefined criteria. Twenty-three studies were population-based studies with participants from a general population. One study reported subgroup data stratified by preexisting CVD (17). All of the included studies were judged as being of relatively high quality according to the NOS assessment tool, with scores ranging from 6 to 9.
Median.
Interquartile range.
Range (min–max).
EU, euthyroidism; SCH, subclinical hypothyroidism; CVD, cardiovascular disease.
Effect of SCH on CVD risk and all-cause mortality
In total, 13,415 fatal or non-fatal CVD events occurred in patients among 283,578 participants from 27 studies (15,16,18,22,24 –26,30,32 –41,43 –51). The pooled RR of CVD was 1.33 ([CI 1.14–1.54]; Fig. 1 and Supplementary Fig. S2), with high heterogeneity (I 2 = 73%) among studies. Since analysis with the funnel plot was asymmetric, the trim-and-fill method to adjust for publication bias was conducted by adding one estimated missing study (RR = 1.25 [CI 1.05–1.49]; Supplementary Fig. S3). In the sensitivity analysis to identify heterogeneity, the pooled RR barely changed, remaining statistically significant after omitting each study (Supplementary Fig. S4); the pooled RR range was 1.25–1.36.
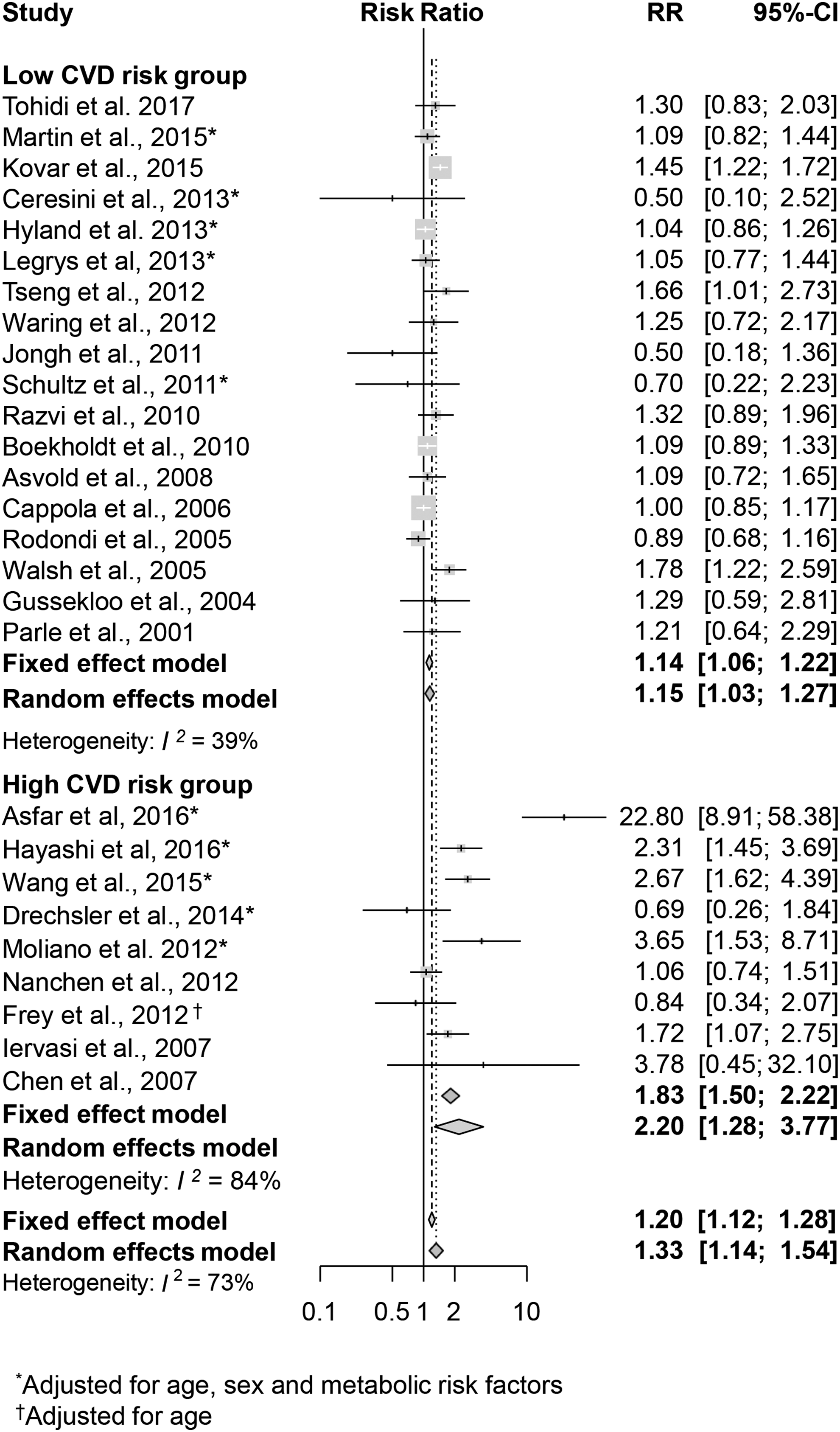
Age- and sex-adjusted relative risk (RR) of combined fatal and non-fatal cardiovascular disease (CVD) associated with subclinical hypothyroidism (SCH) compared to euthyroidism according to CVD risk.
Twenty-nine studies with 532,332 individuals and 68,100 events analyzed all-cause mortality (14 –18,23,27 –32,35 –51). In all participants, a significantly higher risk for all-cause mortality was found in participants with SCH than in those who were euthyroid (RR = 1.20 [CI 1.07–1.34]), with significant heterogeneity (I 2 = 84%; Fig. 2) among studies. The funnel plot showed no publication bias (Supplementary Fig. S3). In the sensitivity analysis to identify heterogeneity, the pooled RR barely changed, remaining statistically significant after omitting each study (Supplementary Fig. S4); the range was 1.16–1.22.
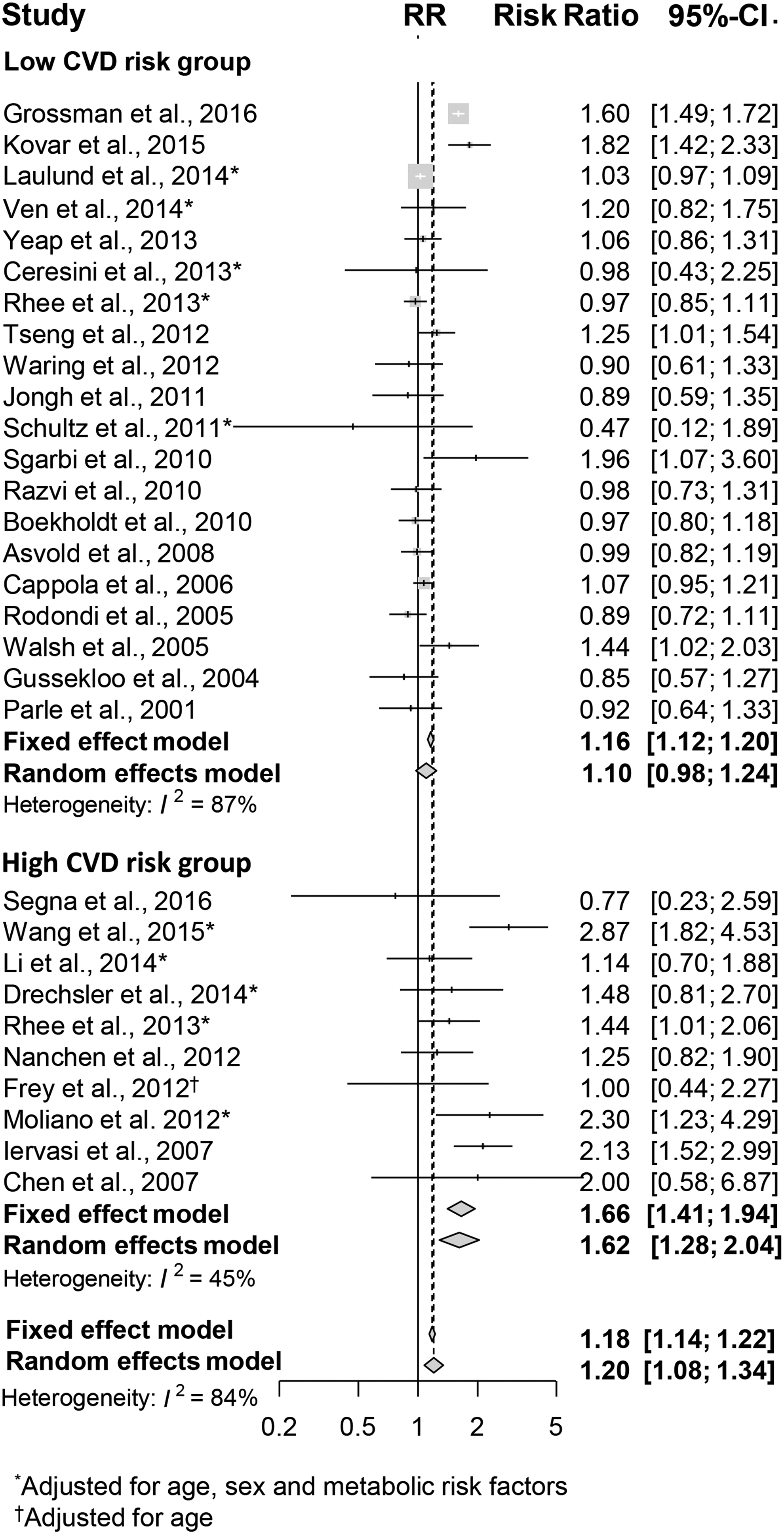
Age- and sex-adjusted RR of all-cause mortality associated with SCH compared to euthyroidism according to CVD risk.
When the subgroup analysis was performed according to location (Table 2), a significant association of SCH with CVD risk and all-cause mortality was found in Asia (RR for CVD = 1.90 [CI 1.50–2.40]; RR for all-cause mortality = 1.60 [CI 1.28–2.00]) and Europe (RR for CVD = 1.34 [CI 1.03–1.74]; RR for all-cause mortality = 1.15 [CI 1.00–1.32]), whereas studies from America failed to show significant results (RR for CVD = 1.02 [CI 0.92–1.12]; RR for all-cause mortality = 1.04 [CI 0.96–1.13]).
RR was adjusted for age and sex.
RR, relative risk; CVD, cardiovascular disease.
Effect of SCH on CVD risk and all-cause mortality according to CVD risk
Effects of SCH on the risk of CVD and all-cause mortality were analyzed according to the status of CVD risk. In the subgroup analysis with high CVD risk groups, SCH significantly increased risk of CVD and all-cause mortality (RR for CVD = 2.20 [CI 1.28–3.77]; I 2 = 84%; RR for all-cause mortality = 1.66 [CI 1.41–1.94]; I 2 = 45%; Figs. 1 and 2). In sensitivity analysis for CVD, the pooled RR barely changed and remained significant after omitting each study; the range was 1.63–2.32. However, in the subgroup analysis with low CVD risk groups, a modest association was observed with CVD (RR = 1.15 [CI 1.06–1.22]; I 2 = 39%; Fig. 1), while there was no significant association with all-cause mortality (RR = 1.10 [CI 0.98–1.24]; I 2 = 87%; Fig. 2). In sensitivity analysis for all-cause mortality, two outlier studies were found (14,15). When these studies were excluded, the pooled RR remained nonsignificant (RR = 1.03 [CI 0.99–1.07]; I 2 = 9%).
Effect of SCH on the risk of CVD and all-cause mortality in aged individuals
It has been suggested that the clinical significance of SCH is different in aged populations (13). Therefore, a meta-analysis was performed after dividing the studies according to the mean age. Subgroup analysis of the studies in which participants had a mean age of <65 years showed a significant association between SCH and risk of CVD and all-cause mortality with significant heterogeneity (RR for CVD = 1.54 [CI 1.21–1.96]; I 2 = 80%; RR for all-cause mortality = 1.28 [CI 1.10–1.48]; I 2 = 80%; Table 2). Sensitivity analysis for CVD found one outlier study (24). The statistical significance remained after omitting the outlier study (RR = 1.32 [CI 1.20–1.45]; I 2 = 49%). In sensitivity analyses for all-cause mortality, no outlier studies could be found, and the pooled RR value barely changed after omitting each study. However, a meta-analysis of the studies in which participants had a mean age of ≥65 years found no significant association between SCH and risk of CVD and all-cause mortality (RR for CVD = 1.07 [CI 0.97–1.18]; I 2 = 49%; RR for all-cause mortality = 1.13 [CI 0.97–1.33]; I 2 = 78%; Table 2). Sensitivity analysis found one outlier study (14). After omitting the outlier study, the pooled RRs of the remaining studies remained nonsignificant (RR = 1.06 [CI 0.98–1.20], I 2 = 25%).
Effect of SCH on the risk of CVD and all-cause mortality based on CVD risk in aged individuals
To determine whether CVD risk factors affect the association between SCH and the risk of CVD and all-cause mortality in aged populations, a further subgroup was made according to CVD risk in the aged population. Among the studies in which participants had a mean age of ≥65 years, subgroup analysis with low CVD risk groups showed no significant association between SCH and the risk of CVD and all-cause mortality (RR for CVD = 1.02 [CI 0.92–1.13]; I 2 = 2%; RR for all-cause mortality = 1.07 [CI 0.89–1.29]; I 2 = 84%; Fig. 3). When one outlier study (14) was excluded from sensitivity analysis for all-cause mortality, the pooled RR remained nonsignificant (RR = 1.04 [CI 0.96–1.12]; I 2 = 18.5%; Fig. 3). However, in contrast to studies with low CVD risk groups, the subgroup analysis with the high CVD risk group showed a significantly high risk of all-cause mortality in the SCH patients without significant heterogeneity (RR = 1.41 [CI 1.08–1.85]; I 2 = 0%; Fig. 3). Although the results for CVD did not reach statistical significance (RR = 1.50 [CI 0.89–2.54]; I 2 = 68%; Fig. 3), studies with high CVD risk groups showed higher risk than those with low CVD risk groups. The results of a subgroup analysis of the studies in which participants had a mean age of <65 years showed similar results (Supplementary Fig. S5).
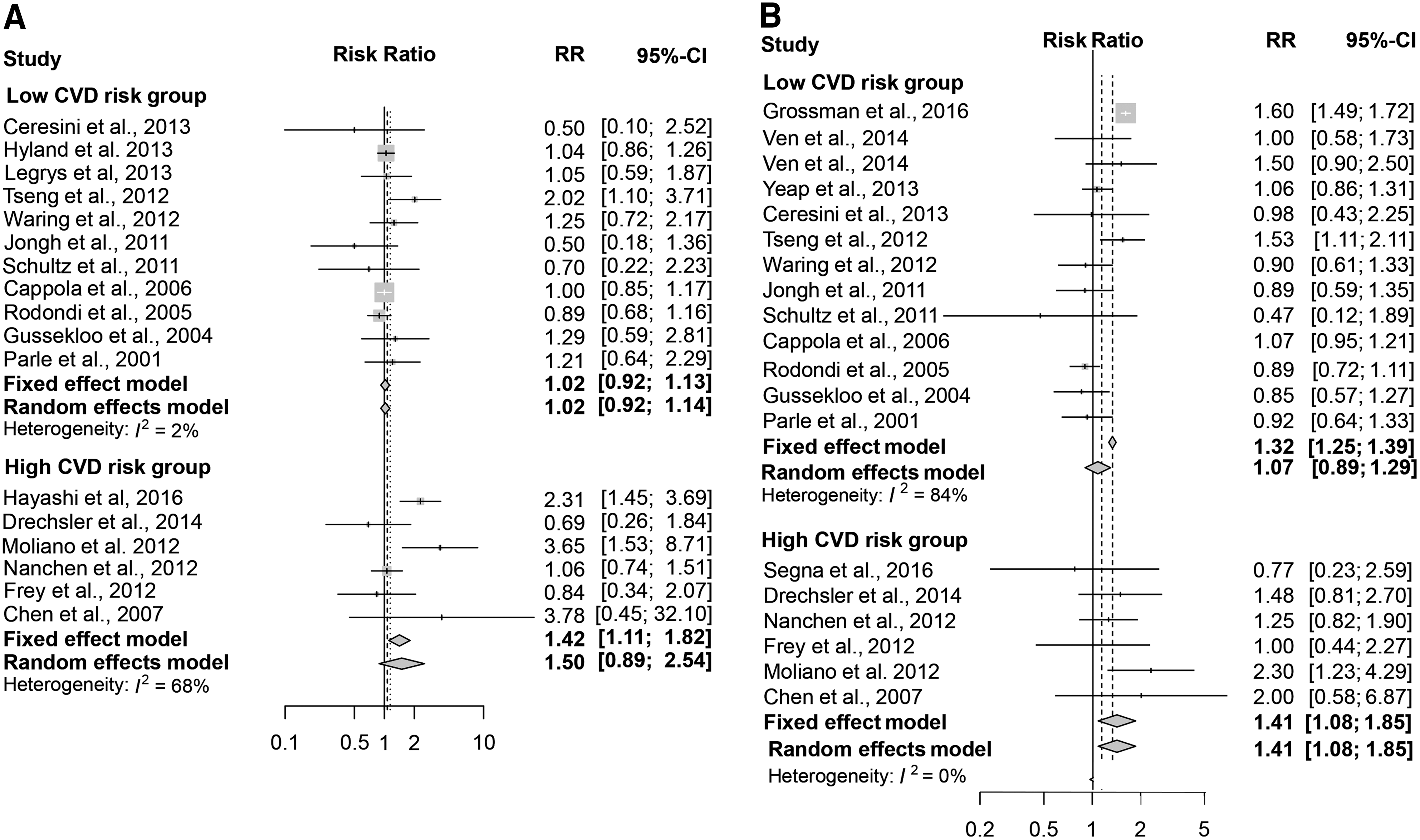
Subgroup analyses of studies with mean age ≥65 years according to CVD risk. (
Discussion
Based on this large-scale meta-analysis with 555,530 participants from 35 cohort studies, it is concluded that SCH is associated with an increased risk of CVD and all-cause mortality, specifically among individuals with high CVD risk. The increased risk of all-cause mortality in participants with SCD and high CVD risk was also observed in aged populations.
In this study, SCH was associated with increased CVD events and all-cause mortality by 20% compared to euthyroid status, and this risk was >60% in the high CVD risk group. Although there was significant heterogeneity, this risk effect persisted after sensitivity analysis and correction of publication bias. This result is different from the previous meta-analysis by Rodondi et al. (10), which reported no association after a meta-analysis of 12 studies. The difference may be due to the recent large population-based studies included in the current analysis (14 –16). Since there was significant heterogeneity, subgroup analyses were conducted to find associations between SCH and the risk of CVD events and all-cause mortality in the different groups.
Interestingly, a significant association between SCH and risk of CVD events and all-cause mortality was found in studies from Asia and Europe, whereas studies from America failed to show significant results. This phenomenon might result from specific ethnic characteristics. However, it also might reflect possible confounding effects stemming from heterogeneity of the study population. All eight American studies were conducted with participants from the general population, whereas four of seven Asian studies and 7 of 18 European studies were performed with participants at high CVD risk. Therefore, further studies with high CVD risk groups in America are needed.
The American Thyroid Association (ATA) and the American Association of Clinical Endocrinologists (AACE) recommend consideration of treatment of SCH for subjects with TSH levels ≥10 mIU/L; symptoms suggestive of hypothyroidism; a positive test for antibodies to thyroid peroxidase; or evidence of atherosclerotic cardiovascular disease, heart failure, or CVD risk factors (13). Because of a lack of data, further analysis according to TSH levels could not be conducted. However, a subgroup analysis was performed stratified by underlying CVD or CVD risk factors. In a previous meta-analysis by Rodondi et al., the association between SCH and CVD events and all-cause mortality did not differ among participants with and without underlying CVD (10). However, several newer studies suggest that groups with SCH and CVD or high underlying CVD risk have a high risk of CVD events and all-cause mortality (17,36,52). The present meta-analysis, which includes the more recent data, demonstrates that SCH is associated with a higher risk of CVD and all-cause mortality in participants with a high CVD risk compared to that of participants with a low CVD risk. Considering the different results compared to the previous meta-analysis, it is assumed that the current study could provide a new perspective to find a subgroup of patients with SCH based on CVD risk that could benefit from treatment. Furthermore, this may provide important evidence to support the current clinical guidelines of the ATA and AACE (13).
The European Thyroid Association (ETA) suggested recommendations for SCH should vary according to patient age (53). In younger subjects (<65–70 years), ETA guidelines recommend treatment of SCH for those with TSH levels of ≥10 mIU/L or symptoms suggestive of hypothyroidism. In contrast, in aged individuals (>70 years), the ETA recommend treatment of SCH for those with TSH levels of ≥10 mIU/L only when they exhibit clear symptoms of hypothyroidism or high CVD risk. Advancing age is associated with increased prevalence of SCH, and around 10% of aged individuals have SCH (3,52,54 –59). SCH is a possible contributor to diverse problems in aged individuals, such as CVD, cognitive dysfunction, musculoskeletal problems, and deleterious effects on bone (10,55,60,61). However, because of a widening of the reference range for TSH with increasing age (57,62), the clinical significance of SCH in aged individuals is poorly understood. In addition, the association between SCH and mortality in elderly people is inconsistent (14,50,58). Albeit the previous meta-analysis failed to find any association between SCH and all-cause mortality in older people, recent large population-based studies reported significant RRs of all-cause mortality (10,14 –16). This updated meta-analysis with recent studies confirms that SCH has no substantial association with all-cause mortality in a general population of aged people, but it did have an association in those with high CVD risk, providing evidence to support the ETA guidelines (53). In contrast to effects in older individuals, the deleterious effect of SCH on CVD events and mortality is well established among young adults (13). The present study also found a deleterious effect of SCH on mortality in studies that investigated relatively younger subjects.
Notably, SCH subjects with high CVD risk persistently show a significantly increased risk of all-cause mortality in both younger and aged communities. Considering the present results, SCH is a clinical heterogeneous entity, and this might be one possible explanation for the contradictory results between previous studies (10,14,50,58). Importantly, the present study demonstrates that assessment of CVD risk might help to find a group in whom treatment of SCH is beneficial, regardless of age.
The considerable strengths of this study are that a number of cohort studies with large populations were included, and predefined subgroup analyses could be performed. However, the present study has some limitations. First, most of the included studies measured TSH and fT4 at a single time point at baseline, and different cutoff values of TSH were used to define SCH across the studies included in the meta-analysis. Second, although effect size from a multivariate model that adjusted for age and sex was predominantly used, several studies did not supply age, sex, and other confounding factors for adjusted hazard ratios. Third, subgroup analysis could not be performed with healthy participants, but this was possible using a general population. Considering that these studies included both healthy participants and preexisting CVD patients, there might be a confounding effect. However, in view of the fact that the SCH patients with high CVD risk had an increased risk of adverse clinical outcomes in the subgroup analysis, the confounding by preexisting CVD appears to have only a minor influence on the results.
In conclusion, the findings demonstrate that SCH is associated with a greater risk of CVD and all-cause mortality in subpopulations with underlying CVD or high CVD risk. Further well designed prospective cohort studies are necessary to find high-risk groups, and randomized controlled trials are needed to investigate possible benefits of a levothyroxine replacement therapy in these high-risk groups.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.