
Abstract
The 2017 American Thyroid Association guidelines for the diagnosis and management of thyroid disease during pregnancy and the postpartum were published six years after the previous ones. They provide comprehensive clinical recommendations for the whole spectrum of thyroid diseases, as well as for optimal iodine intake during pregnancy, postpartum, and lactation. The present position statement mainly regards the recommended flow chart for therapeutic decision making in pregnant women being diagnosed with subclinical hypothyroidism. Here, we comment on the major biochemical and clinical situations and the corresponding therapeutic recommendations. In particular, we welcome the critical revision of the thyrotropin (TSH) reference range in pregnancy, and we agree that there is no need to treat thyroid peroxidase antibody–negative women with a serum TSH ranging from 2.5 μIU/mL to the upper limit of the reference range. This recommendation will hopefully reduce the huge proportion of healthy pregnant women in whom, according to the previous guidelines, levothyroxine therapy had to be initiated. On the other hand, we are concerned with the recommendation to only “consider treatment” in thyroid peroxidase antibody–negative pregnant women with a serum TSH ranging from the upper limit of the reference range to 10.0 μIU/mL. This is because thyroid antibodies may be falsely negative during gestation, and serum negative chronic autoimmune thyroiditis is a well-known clinical entity even outside pregnancy. Based on these and other arguments, we recommend treatment with levothyroxine in pregnant women with TSH levels ranging between the upper limit of the reference range and 10.0 μIU/mL independently from their thyroid antibody status.
I
The 2017 version of the American Thyroid Association (ATA) guidelines for the diagnosis and management of thyroid disease during pregnancy and the postpartum (11) were published six years after the previous ones (12) and took into account several recent, specifically designed, studies. We welcome the critical revision of the thyrotropin (TSH) reference range in pregnancy, and we fully agree that five studies, which appeared after the publication of the 2011 ATA guidelines (13 –17), demonstrate that the previous cutoff of TSH for defining SH in a pregnancy (>2.5 μIU/mL) was too low when referred to a population of thyroid disease-free women with adequate iodine intake and negative test for thyroid autoantibodies. As a consequence of this low cutoff, LT4 therapy was recommended in a huge proportion of healthy pregnant women. According to the 2017 ATA guidelines (11), the upper limit of the reference range for TSH, at least for the first trimester of pregnancy, can be calculated by subtracting approximately 0.5 μIU/mL from the upper limit of the non-pregnant reference range. Thus, this results in an upper end of the reference range of 4.0 μIU/mL with most assays. In the second and third trimesters, the non-pregnant upper reference range can be used as a cutoff (11). It is evident that increasing the upper reference range for TSH will greatly reduce the number of pregnant women diagnosed with SH, especially in the first trimester.
The above concept, however, does not automatically imply that once SH is diagnosed, treatment decisions should be changed. Our position statement mainly regards the recommended flow chart (Fig. 1) for decision making (treat/do not treat) in pregnant women being diagnosed with SH. We will comment on the four major laboratory and clinical situations and on the corresponding therapeutic recommendations.
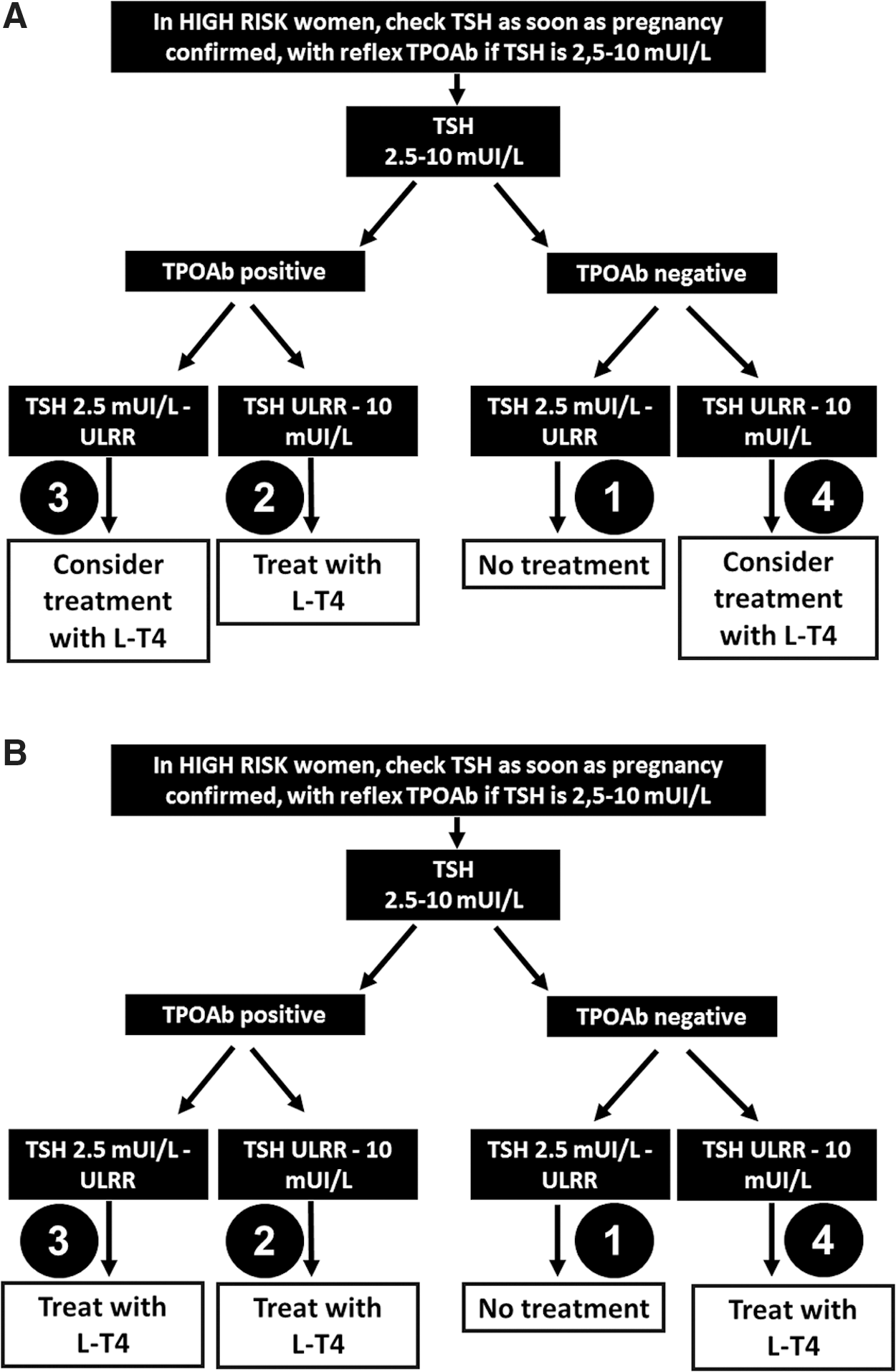
Algorithm for diagnosing and treating subclinical hypothyroidism in pregnant women, as recommended by the American Thyroid Association (
This is definitely the most relevant change introduced in the 2017 ATA guidelines (11). The recommendation is fully supported by five recently (after 2011) published studies, which enrolled >60,000 healthy and iodine-sufficient pregnant women with negative tests for thyroid peroxidase (TPO) autoantibodies (13 –17). The 2017 ATA recommendations are far more evidence based than the 2011 ones because the previous upper cutoff values for normal TSH (2.5 μIU/mL and 3.0 μIU/mL in the first and second/third trimester, respectively) derived from small series of pregnant women (18 –23).
Our conclusion: We agree with the modified recommendation.
This recommendation is unchanged with respect to the corresponding one in the 2011 ATA guidelines. Solid and long-standing evidence supports this indication.
Our conclusion: We agree with the modified recommendation.
This recommendation was changed compared with the 2011 ATA guidelines, which recommended LT4 treatment in the presence of a serum TSH concentration ranging from 2.5 to 4.0 μIU/mL and positive tests for TPO autoantibodies (12). In contrast, the 2017 ATA guidelines state that in the same situation, LT4 treatment should be considered, but this statement is not discussed in further detail (11). A “consider treatment” recommendation is of little help for clinicians involved in decision making. In our opinion, based both on personal experience and on previous—although limited—evidence (24,25), giving low-dose LT4, aimed at maintaining serum TSH <2.5 μIU/mL, is advisable. This treatment is not harmful and likely prevents further increases in serum TSH levels resulting from thyroid function deterioration in later stages of pregnancy. The strength of this recommendation is greater in the first trimester of pregnancy and becomes progressively weaker from mid-second trimester to term.
Our conclusion: We recommend treatment with LT4.
We are concerned with this 2017 ATA guidelines recommendation, which, in our opinion, does not appear fully evidence based. This is based on the following considerations:
1. For pregnant women with a serum TSH concentration ranging from the upper limit of the reference range to 10.0 μIU/mL, the 2017 ATA guidelines make a recommendation of “treatment” or “consider treatment” only based on the presence of positive or negative tests for circulating TPO autoantibodies (11). According to these guidelines (11), serum free thyroxine (fT4) levels should not be considered, mainly due to the technical limitations of the currently employed analytical methods, which are affected by the concentration of thyroxine-binding proteins (26). In our opinion, several reasons question a therapeutic decision based only on TPO autoantibody status. First, negative tests for TPO antibodies are found in a consistent proportion of patients with chronic autoimmune thyroiditis because of the pregnancy-specific immune suppressive status (27 –30). Although the effects of the alterations in the immune system become more evident in the second and third trimesters, negative tests for TPO autoantibodies may occur, even in the first trimester, mainly in women with chronic autoimmune thyroiditis but only modest elevations of thyroid autoantibodies outside pregnancy. Second, although thyroid autoantibodies represent the main biochemical marker of chronic autoimmune thyroiditis, the disease may occur in the absence of positive tests for thyroglobulin and TPO autoantibodies. This condition is commonly referred to as serum-negative chronic autoimmune thyroiditis (CAT) and, with few exceptions (31), can be easily diagnosed if an increased serum TSH value is associated with a hypoechoic pattern of the thyroid parenchyma on ultrasound (32). According to recent studies specifically addressing this topic, the prevalence of serum-negative CAT is not negligible, ranging between 10% and 15% of all patients with chronic autoimmune thyroiditis (33). Based on the above considerations, we believe that giving too much diagnostic credit to thyroid autoantibody status might lead to underestimating the number of patients who would require treatment.
2. Two recent prospective randomized intervention studies in pregnant women with slightly raised serum TSH levels likely influenced the 2017 panel decision to give the “consider treatment” recommendation (9,10,34). Lazarus et al. (9) and Casey et al. (10) performed two similarly designed independent studies and reported that compared with placebo, LT4 therapy did not produce any benefit on maternal and fetal outcomes. Both studies were accompanied by an editorial (35,36), and in both cases the fact that treatment with LT4 was started too late (at approximately 13 and 16 weeks of pregnancy, respectively) was identified as a major limitation (35,36). Indeed, the maternal surge of fT4 in early pregnancy (first 12 weeks) plays a major role in the development of the fetal brain (37,38). In addition to the above limitation, we would like to stress that evaluating the cognitive performance of the progeny at the age of three years (9), or at both three and five years (10), might be too early to detect significant alterations (38,39). Data in the literature suggest that the negative repercussions of maternal hypothyroidism might become evident only later in childhood (39,40).
However, there are three studies reporting no apparent neurodevelopmental deficit (as assessed by Intelligence Quotient and Developmental Quotient scores) in children born to overtly hypothyroid mothers who received substitution LT4 only late in pregnancy (41 –43), which would support the conclusions of the above-mentioned large prospective studies (9,10). These aspects deserve to be highlighted in order to reassure pregnant hypothyroid women who might consider voluntary pregnancy interruption. Thus, the observation by Haddow et al. reporting that maternal hypothyroidism, even when subclinical, can adversely affect the neuropsychic performance of the progeny still remains a matter of debate (44).
Taking together the above considerations, we acknowledge that the available prospective randomized data do not demonstrate a clear benefit of LT4 treatment in TPO antibody–negative women, thus being in line with the recommendation of the panel of the 2017 ATA guidelines. However, it should be taken into account that physicians are continually forced to make assumptions about risk–benefit ratios, and because of that, we believe a stronger recommendation should be favored, despite the lack of hard evidence. Our position stems, at least in part, from the evaluation of benefit versus risk (and cost), which, in our opinion, favors the former. A few potential downsides of a stronger recommendation favoring treatment include, at least theoretically, that a small proportion of women could be over-treated, and some women could be committed unnecessarily to long-term LT4 therapy. The latter risk implies that in women with negative tests for TPO autoantibodies, the need for LT4 treatment must be reevaluated after parturition in order to avoid unnecessary lifelong LT4 therapy and its associated costs.
Nevertheless, while waiting for more robust evidence demonstrating either benefit or no benefit of LT4 therapy in mothers with slightly elevated (up to 10 μIU/mL) serum TSH concentrations, it is our opinion that LT4 therapy aimed at maintaining serum TSH levels <4.0 μIU/mL is advisable, at least to prevent further increases in TSH levels later in pregnancy.
Our conclusion: We recommend treatment with LT4.
Conclusions
Based on the above considerations, we recommend treatment with LT4 in pregnant women with TSH levels ranging between 4.0 and 10.0 μIU/mL independently from their thyroid autoantibody status. While nearly a third of pregnant women worldwide would be treated (and likely over-treated) with LT4 based on the previous 2011 ATA guidelines, the new TSH reference ranges recommended for pregnant women in the 2017 ATA guidelines allow a more precise identification of mothers with subclinical hypothyroidism. The consequence is a marked reduction in the number of pregnant women treated with LT4 and not requiring it. However, there is good reason to treat those who may benefit from treatment!
Footnotes
Author Disclosure Statement
No competing financial interests exist.