
Abstract
Background:
Maternal thyroid dysfunction may adversely affect fetal brain development, but more evidence is needed to refine this hypothesis. The aim of this study was to evaluate potential fetal programming by abnormal maternal thyroid function on child neurodevelopmental disorders.
Methods:
The design was a case-cohort study within the Danish National Birth Cohort (1997–2003). From the eligible cohort of 71,706 women, a random 12% sub-cohort (n = 7624) was selected, and all women (n = 2276) whose child was diagnosed with seizures, specific developmental disorder (SDD), autism spectrum disorder (ASD), and/or attention-deficit/hyperactivity disorder (ADHD) up to December 31, 2010, were identified. All women had a blood sample drawn in early pregnancy (median week 9), and the stored sample was used for measurement of free thyroxine and thyrotropin. Method- and week-specific reference ranges were used for classification of maternal thyroid function. A weighted Cox proportional hazards model was used to estimate adjusted hazard ratio (aHR) with 95% confidence intervals (CI) for neurodevelopmental disorders in children exposed to maternal thyroid dysfunction.
Results:
The overall frequency of abnormal maternal thyroid function was 12.5% in the sub-cohort and significantly higher among cases of ASD (17.9%; aHR = 1.5 [CI 1.1–2.1]), but not among other types of neurodevelopmental disorders (febrile seizures: 12.7%; epilepsy: 13.1%; SDD: 12.6%; and ADHD: 14.0%). However, evaluation of subtypes of maternal thyroid dysfunction showed that maternal overt hypothyroidism (thyrotropin >10 mIU/L) was a risk factor for epilepsy in the child (aHR = 3.5 [CI 1.2–10]), as was overt hyperthyroidism for cases diagnosed within the first year of life (aHR = 3.0 [CI 1.03–8.4]). Furthermore, both maternal hypothyroidism (aHR = 1.8 [CI 1.1–2.7]) and overt hyperthyroidism (aHR = 2.2 [CI 1.1–4.4]) were risk factors for ASD in the child, and isolated low free thyroxine was associated with ASD (aHR = 4.9 [CI 2.03–11.9]) and ADHD (aHR = 2.3 [CI 1.2–4.3]) in girls but not in boys.
Conclusions:
Abnormal maternal thyroid function in early pregnancy was associated with epilepsy, ASD, and ADHD in the child, but associations differed by subtypes of exposure and by child age and sex. More evidence on subtypes and severity of maternal thyroid function is needed, and alternative outcomes of child neurodevelopment may be warranted.
Introduction
T
Neurodevelopmental disorders are diseases that develop secondary to disruption of early brain development, and symptoms may range from specific disabilities to global impairments (3). Previously, a higher risk of seizures (4), autism spectrum disorders (ASD) (5), and attention-deficit/hyperactivity disorder (ADHD) (5) was observed in children born to mothers diagnosed with hyper- or hypothyroidism in the years following the pregnancy. These children may have been exposed to unidentified maternal thyroid dysfunction in the pregnancy, but only crude indicators of exposure were available from hospital diagnoses and redeemed prescription of drugs in these large cohort studies using data from the Danish nationwide registers.
The present study obtained more specific information on maternal thyroid function in early pregnancy as evaluated by measurement of thyrotropin (TSH) and free thyroxine (fT4) in stored biobank samples from a large number of pregnant women in the Danish National Birth Cohort (DNBC). A case-cohort study was designed, and maternal thyroid function was measured in a random sub-cohort and in all women in the entire cohort whose child was diagnosed with a neurodevelopmental disorder during follow-up.
Method and Materials
Study design and population
The DNBC is a Danish nationwide birth cohort established from 1997 to 2003 (6). In brief, the cohort included about 100,000 pregnant women who lived in Denmark and were able to participate in telephone interviews in Danish during the pregnancy. All women included in this study gave birth to a singleton live-born child (Fig. 1). If a woman gave birth more than once during the study period, only information from the woman's first pregnancy in the recruitment period was included. The present study was a case-cohort design within the DNBC. Women eligible for inclusion had a blood sample drawn in general practice at the time of inclusion in early pregnancy (median 9th week; range 5th–19th week). The blood sample was sent by mail and stored in a −80°C freezer in the Danish National Biobank. From the 71,706 women eligible for the study, a 12% random sub-cohort was drawn, and in addition to this, all women in the eligible cohort whose child was diagnosed with a neurodevelopmental disorder in Danish nationwide registers up to December 31, 2010, were sampled (Fig. 1). As expected from the sampling procedure, there was an overlap between individuals in the random sub-cohort and cases (Fig. 1). For a group of participants, thyroid function test results were not available, mainly because the stored blood sample was not available (Fig. 1). All participants had provided written informed consent at the time of inclusion in the DNBC. The study was approved by the Danish Ethic Committee (N-20130054).
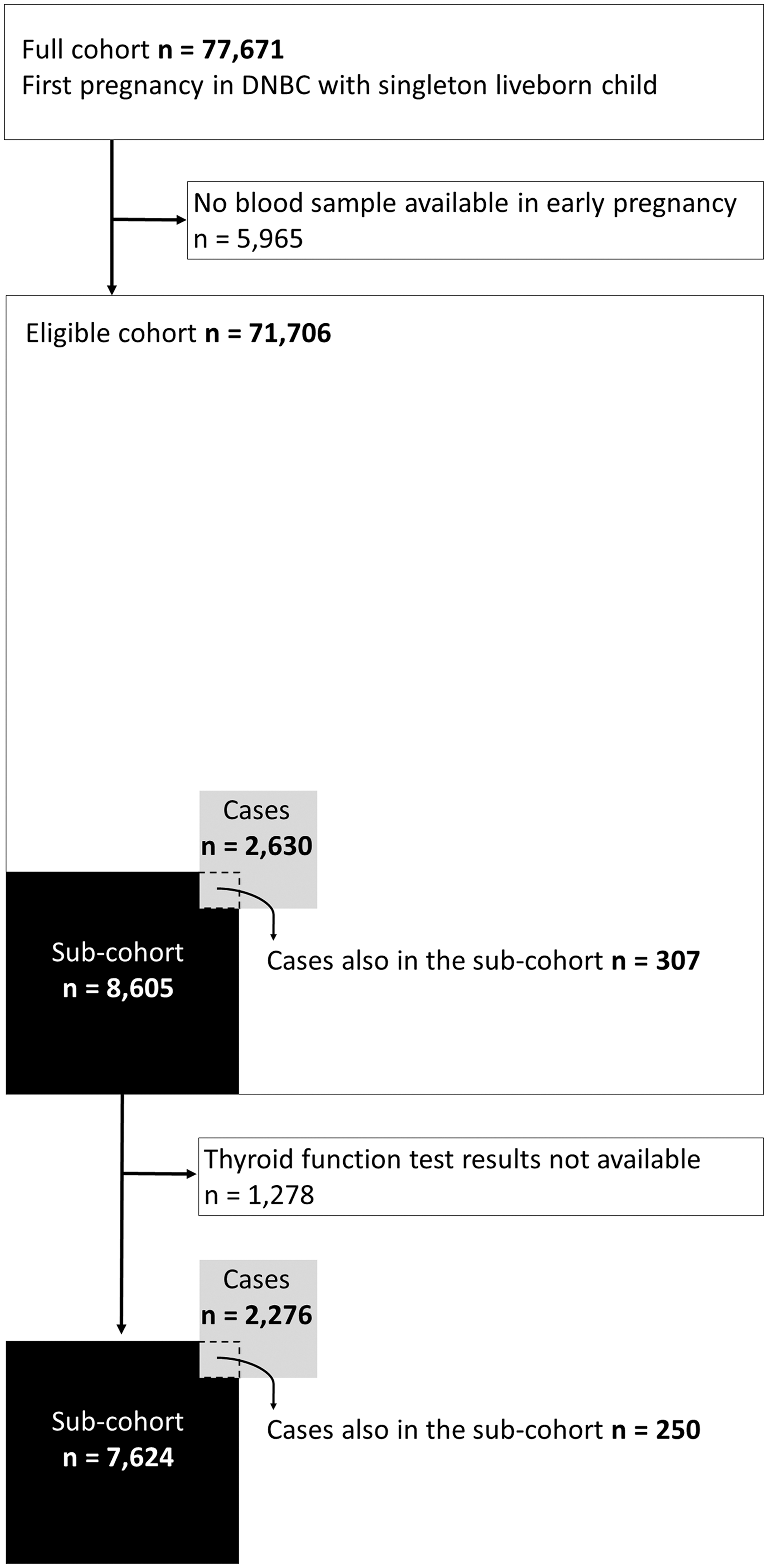
Flow chart illustrating the selection of the study population from the Danish National Birth Cohort (DNBC), including a 12% random sub-cohort sample and all cases in the entire cohort diagnosed with epilepsy, febrile seizures, specific developmental disorders, autism spectrum disorders, or attention-deficit/hyperactivity disorder during follow-up. Individuals sampled as both sub-cohort member and as a case are illustrated as “Cases also in the sub-cohort.”
Exposure
Maternal thyroid function in the early pregnancy blood sample was evaluated from measurement of TSH and fT4 by a Dimension Vista automated immunoassay (Siemens Healthcare Diagnostics, Eschborn, Germany) in 2015, as previously described (7). Maternal thyroid function was classified according to the method- and pregnancy week-specific reference ranges (2.5 and 97.5 percentiles) previously established and described for this cohort of women (7,8). Information on hospital diagnosis and treatment of maternal thyroid disease was available via linkage to Danish nationwide health registers, as previously described (8,9). For each woman, information was available on known thyroid disease and previous or current treatment at the time of blood sampling in early pregnancy and on thyroid disease diagnosed and treated up to five years after the pregnancy under study.
Outcomes
Information on neurodevelopmental disorders in the child was obtained via linkage to the Danish National Hospital Register (DNHR) (10), the Danish Central Psychiatric Register (DCPR) (11), and the Danish National Prescription Register (12), which hold nationwide information on in- and outpatient hospital diagnoses of disease classified according to the 10th revision of the International Classification of Disease (ICD-10) and redeemed prescription of drugs classified according to the anatomical therapeutic chemical classification system (ATC). For each child, information on neurodevelopmental outcomes was included from day 31 after birth (to exclude the neonatal period) and up to December 31, 2010 (to December 31, 2007, for diagnoses in the DCPR). Epilepsy was defined by a diagnosis of epilepsy (ICD-10: G40.0–G41.9) and a minimum of two redeemed prescriptions of antiepileptic drugs (ATC: N03). Febrile seizures were defined by minimum two diagnoses of the disease (ICD-10: R56.0) registered before the age of five years. Specific developmental disorders (SDD) and ASD were defined by a diagnosis of the disease (ICD-10: F80.0–F89.9)), and ADHD was defined by a minimum of two redeemed prescriptions of drugs used for treatment of the disorder (ATC N06BA).
Covariates
Information on covariates was available from the Danish Medical Birth Register (13) (maternal age and number of previous childbirths, child sex, and day of birth) and the DNBC telephone interview in early pregnancy (maternal pre-pregnancy weight and height, alcohol intake, and current smoking). From Statistics Denmark, data were obtained on maternal origin, geographical residence, and educational level. In addition, information was obtained on maternal psychiatric disease (hospital diagnosis [ICD-8: 295.19-315.99; ICD-10: F00.0–F99.9]), redeemed prescription of drugs used for treatment of psychiatric disease (ATC: NO5AA-N06AX), and anti-epileptic drugs (ATC: N03) before, during, and up to five years after the pregnancy.
Statistical analyses
Measures of association were assessed using a weighted Cox proportional hazards model, with the age of the child as the time axis. Children were followed from day 31 after birth to diagnosis of disease, death, emigration, or December 31, 2010, whichever came first. A small number of children diagnosed with unspecified developmental disorder only (n = 11) were not included in the follow-up study for developmental disorders. The weighting scheme by Kalbfleisch and Lawless (14) was used to account for the oversampling of cases. The proportional hazards assumption was evaluated in log-log plots and by scaled Schoenfeld residuals, which showed no violation of the assumption.
Crude and adjusted analyses were performed in separate models for each category of maternal thyroid dysfunction (all types combined as well as subtypes of overt and subclinical hyper- and hypothyroidism and isolated low/high fT4 separately). TSH and fT4 were also included in the models as continuous independent variables, and a possible non-linear relationship was investigated in restricted cubic spline models. Potential confounders were identified a priori, and covariates were finally selected from this group by a stepwise procedure (p = 0.1). The main model included the birthday of the child, maternal age, parity, geographical residence, educational level, pre-pregnancy body mass index (BMI), smoking in the pregnancy, and maternal psychiatric/seizures disorder. Maternal origin and pre-pregnancy alcohol intake were not confounders in any of the models and were not included. Pre-pregnancy alcohol intake was chosen to include information on alcohol intake prior to pregnancy recognition (15,16). The birthday of the child and maternal age were included as restricted cubic spline (five knots), other variables as categorical. Gestational age at birth and birth weight were considered potential intermediates and not included in the main model. Child sex was considered a potential effect measure modifier, and stratified analyses were performed. Multiplicative interaction was assessed by the inclusion of cross-product term (maternal thyroid function and child sex) in the adjusted model along with the main effect terms.
Multiple imputation by chained equations (five imputed data sets) was used to impute missing data on covariates (BMI 1.7%, educational level 0.4%, geographical residence 0.3%, and smoking in pregnancy <0.1%) to maintain participants with incomplete data (n = 228). The robustness of the imputation was examined using more imputed data sets (n = 20), and complete case analysis revealed similar measures of association.
Statistical analyses were performed using STATA v14 (Stata Corp., College Station, TX). A 5% level of significance was chosen, and adjustment for multiple comparisons was not performed (17).
Results
Study population
A total of 7624 children were included in the sub-cohort, and 2276 cases were identified, leaving 250 children as both a case and a sub-cohort member (Fig. 1). The sub-cohort was representative of the entire eligible cohort (Table 1), and a significant disparity was only observed for maternal geographical residence. Among the 2276 cases, 172 children were diagnosed with more than one disorder during follow-up, resulting in 2455 diagnoses of neurodevelopmental outcomes (Table 1; seizures, n = 825; developmental disorders, n = 487; and ADHD, n = 1143).
Among the 2276 children identified as a case, 2104 had one diagnosed disorder, 165 were diagnosed with two disorders, and seven children with three disorders, resulting in 2455 diagnoses of seizures, developmental disorders, and ADHD.
p < 0.05 for comparison of cases (n = 2276) and non-cases in the sub-cohort (n = 7374) using the chi-square test.
Individuals with missing values not included (origin n = 19, geographical residence n = 239, educational level n = 244, smoking in pregnancy n = 24, pre-pregnancy BMI n = 1225, pre-pregnancy alcohol intake n = 101).
Divided by the Great Belt.
p < 0.05 for comparison of sub-cohort and eligible cohort using the chi-square test.
Self-reported by telephone interview in early pregnancy.
Hospital diagnosis and/or prescription of psychiatric drugs or antiepileptic drugs up to five years after birth of the child.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index.
For the 825 cases with seizures, 489 were diagnosed with febrile seizures at a median of 1.2 years of age and 375 with epilepsy at median of 3.5 years of age, including 39 children with a diagnosis of both types of seizures (Table 2).
Adjusted model included birthday of child, maternal age, parity, history of psychiatric/seizure disorder, geographical residence, educational level, pre-pregnancy BMI, and smoking in the pregnancy.
TSH above the week- and method specific 2.5 percentile and below the 97.5 percentile; fT4 above the week- and method specific 2.5 percentile and below the 97.5 percentile.
TSH below the week- and method specific 2.5 percentile; fT4 above the week- and method specific 97.5 percentile.
TSH below the week- and method specific 2.5 percentile; normal fT4.
TSH above the week- and method specific 97.5 percentile; fT4 below the week- and method specific 2.5 percentile.
TSH above the week- and method specific 97.5 percentile; normal fT4.
fT4 below the week- and method specific 2.5 percentile; normal TSH.
fT4 above the week- and method specific 97.5 percentile; normal TSH.
HR, hazard ratio; CI, 95% confidence interval; fT4, free thyroxine; TSH, thyrotropin.
Among the 487 cases with developmental disorders, 476 were eligible for the follow-up study. A total of 174 children were diagnosed with SDD at a median of 5.5 years of age, and 302 children were diagnosed with ASD at a median of 5.3 years of age (Table 3). Finally, 1143 children initiated medical treatment for ADHD at a median of 8.4 years of age (Table 3). There was a male predominance for the majority of disorders (male sex sub-cohort, 50%; seizures, 56%; developmental disorders, 74%; and ADHD, 80%).
Children with a diagnosis of unspecified developmental disorder (n = 11) were not included.
Adjusted model included birthday of child, maternal age, parity, history of psychiatric/seizure disorder, geographical residence, educational level, pre-pregnancy BMI, and smoking in the pregnancy.
TSH above the week- and method specific 2.5 percentile and below the 97.5 percentile; fT4 above the week- and method specific 2.5 percentile and below the 97.5 percentile.
TSH below the week- and method specific 2.5 percentile; fT4 above the week- and method specific 97.5 percentile.
TSH below the week- and method specific 2.5 percentile; normal fT4.
TSH above the week- and method specific 97.5 percentile; fT4 below the week- and method specific 2.5 percentile.
TSH above the week- and method specific 97.5 percentile; normal fT4.
fT4 below the week- and method specific 2.5 percentile; normal TSH.
fT4 above the week- and method specific 97.5 percentile; normal TSH.
CI, 95% confidence interval.
Maternal characteristics differed markedly between cases and sub-cohort for most covariates, except maternal origin and pre-pregnancy alcohol intake (Table 1). In the sub-cohort (Table 2), a total of 951 (12.5%) women were classified with abnormal thyroid function, including overt and subclinical hyper- or hypothyroidism, as well as isolated low or high fT4. The vast majority of these women (n = 904) had no known thyroid disease (no diagnosis or treatment) at the time of blood sampling, whereas 47 had a diagnosis of thyroid disease (22 received current treatment). Similarly, the majority of the 6673 women classified as euthyroid had no known thyroid disease (n = 6572), whereas 101 had a diagnosis of thyroid disease (17 received current treatment).
Overall associations
Overall, maternal thyroid dysfunction did not associate with febrile seizures and epilepsy (Table 2) or SDD (Table 3). The frequency of abnormal maternal thyroid function in children diagnosed with ASD was 17.9% and was significantly higher than in the sub-cohort, which was consistent in adjusted analyses (Table 3). Among cases of ADHD, the frequency of abnormal maternal thyroid function was 14.0%, which was slightly higher than in the sub-cohort but did not reach statistical significance in adjusted analyses (Table 3).
Associations with subtypes of maternal thyroid dysfunction
Additional findings appeared for outcomes of epilepsy, ASD, and ADHD, while no associations emerged from evaluation of subtypes of maternal thyroid dysfunction for outcomes of febrile seizures and SDD (Tables 2 and 3). For epilepsy, results indicated an association with maternal overt hypothyroidism (Table 2), but the estimate did not reach statistical significance. For ASD, significant associations with maternal overt hyperthyroidism and maternal hypothyroidism were observed (Table 3), whereas no association with overt thyroid disease was observed for ADHD.
Notably, all cases of epilepsy and ASD diagnosed after exposure to maternal overt hyper- or hypothyroidism were born to mothers with no known thyroid disease at the time of blood sampling, and women with known thyroid disease (n = 101 sub-cohort members) were excluded from the subsequent analyses of child's age and severity of maternal overt thyroid disease. First, the association between maternal overt hyperthyroidism and epilepsy was modified by age of the child at diagnosis of epilepsy. Thus, children born to mothers with overt hyperthyroidism were a median of nine months at diagnosis, which was younger than non-exposed children (3.5 years; p = 0.02). In stratified analyses, maternal overt hyperthyroidism was associated with epilepsy diagnosed before the age of one year (Table 4). Modification by child's age was not observed for associations with overt hypothyroidism or with outcome of ASD. Second, the severity of maternal overt thyroid disease was evaluated from levels of maternal TSH and fT4 among children who either had no neurodevelopmental outcome or were diagnosed with epilepsy or ASD. For overt hypothyroidism, median maternal TSH was higher among cases of epilepsy (median 11.0 mIU/L; range 3.5–26.2 mIU/L) than non-cases (6.4 mIU/L; 3.3–89.2 mIU/L) but not among cases of ASD. Maternal TSH >10 mIU/L was a significant risk indicator for epilepsy in the child (adjusted hazard ratio [aHR] = 3.5 [95% confidence interval (CI) 1.2–10.0]). However, the distribution of maternal TSH among non-cases was wide and included a number of high values, suggesting a low predictive value of a positive test. No differences were observed in maternal fT4 or in levels of TSH and fT4 for maternal overt hyperthyroidism.
Children born to mothers with known thyroid disease at the time of blood sampling were not included.
Adjusted model included birthday of child, maternal age, parity, history of psychiatric/seizure disorder, geographical residence, educational level, pre-pregnancy BMI, and smoking in the pregnancy.
TSH above the week- and method specific 2.5 percentile and below the 97.5 percentile; fT4 above the week- and method specific 2.5 percentile and below the 97.5 percentile.
TSH below the week- and method specific 2.5 percentile; fT4 above the week- and method specific 97.5 percentile.
CI, 95% confidence interval.
In crude analyses, an association between maternal isolated low fT4 and ASD as well as ADHD in the child was observed (Table 3). However, associations were attenuated after adjustment for potential confounders. When stratified by sex of the child, differences in the stratum-specific estimates were identified (Table 5). Notably, an association with maternal hypothyroxinemia was observed only in girls, and a significant interaction on the multiplicative scale was observed for the association with ASD (Table 5). The significant dependency on child sex was not seen for associations with other types of maternal thyroid dysfunction or for other outcomes of neurodevelopmental disorders.
TSH above the week- and method specific 2.5 percentile and below the 97.5 percentile; fT4 above the week- and method specific 2.5 percentile and below the 97.5 percentile.
fT4 below the week- and method specific 2.5 percentile; normal TSH.
Adjusted model included: birthday of child, maternal age, parity, history of psychiatric/seizure disorder, geographical residence, educational level, pre-pregnancy BMI, and smoking in the pregnancy.
Measure of interaction on multiplicative scale (cross product term between child's sex and maternal isolated low fT4): autism spectrum disorder: 4.91 [CI 1.46–16.54], p = 0.010; ADHD: 1.95 [CI 0.771.80], p = 0.09.
CI, 95% confidence interval.
Additional analyses
The evaluation of fT4 and TSH as continuous variables showed no significant association with any outcome of neurodevelopmental disorders, and no non-linear relation was observed. Twenty-two children were identified who had registrations of treatment for hypothyroidism during follow-up. Child hypothyroidism was more common among cases (0.5%) than in the sub-cohort (0.2%), but exclusion of this group did not change the associations observed. The frequency of abnormal maternal thyroid function in children with multiple outcomes was 11.6% and did not differ from the overall frequency. Preterm birth (<37 weeks) and low birth weight (<2500 g) were more frequent in children with seizures. However, additional adjustment for these covariates did not change the results.
Discussion
Principal findings
In this nationwide case-cohort study, maternal thyroid function was measured in stored biobank samples from a large number of pregnant women. Abnormal maternal thyroid function was a risk indicator for severe and pervasive neurodevelopmental disorders (epilepsy, ASD, and ADHD) in the child but not for the more specific and less pervasive disorders (SDD and febrile seizures). The results corroborate previous findings to some extent, but associations were diverse and differed by subtypes of exposure and neurodevelopmental outcomes and were modified by child age and sex.
Thyroid hormones and brain development
How maternal thyroid function in pregnancy may influence fetal brain development has been examined for decades, and the scientific evidence is based on studies of different design and methods. Experimental studies in rats have shown diverse effects of maternal hypo- and hyperthyroidism on brain development in the offspring (18). In humans, case descriptions of neurological symptoms in endemic cretinism provided evidence of the detrimental effects of maternal hypothyroidism (19). Over the years, the evidence has been extended by numerous case-control and cohort studies, which have provided a non-exposed control group, but the observational design may be prone to bias or confounding, and findings have been diverse. Randomized controlled trials provide the highest level of confidence, but such studies have not demonstrated significantly improved child neurocognitive outcomes by treatment of maternal hypothyroidism or hypothyroxinemia in pregnancy (20,21).
Previous and present findings
Previously, Danish nationwide register studies were performed to evaluate the association between maternal thyroid disease in pregnancy and child neurodevelopmental disorders. A consistent finding in these studies (4,5) was a higher risk of seizures, ASD, and ADHD in children born to mothers who were first diagnosed and treated for hyper- or hypothyroidism in the years following the pregnancy and possibly had undetected disease during the pregnancy. These studies were characterized by a large study population including all children born in Denmark over a period of years, but relied on indicators of exposure in pregnancy from redeemed prescriptions of drugs and hospital diagnosis of disease, and less detail on potential confounders.
The present study was strengthened by the case-cohort design. Measurement of maternal thyroid function in early pregnancy provided the opportunity to study multiple outcomes using the same random sub-cohort. Results were consistent with the previous findings to some extent. However, although maternal thyroid function was measured in a large number of pregnant women, the number of exposed cases was limited in some of the analyses. In line with the previous findings, abnormal maternal thyroid function was a risk indicator for epilepsy, ASD, and ADHD but not for febrile seizures.
Seizure disorders
Studies in rats have shown a higher frequency and more severe types of seizures after exposure to maternal hypothyroidism in pregnancy (22,23), and studies in non-pregnant rats have shown a higher seizure susceptibility in experimental hyperthyroidism (24,25). Notably, the association between maternal hypothyroidism and epilepsy in the child in the present study was confined to cases with marked maternal hypothyroidism. For overt hyperthyroidism, the association was observed for cases of epilepsy diagnosed within the first year of life, but they all received continuous treatment with antiepileptic drugs. The disparity in the results for different types of seizures and the association with overt maternal thyroid disease, but not with smaller aberrations in maternal thyroid function, is a key finding and may support an association.
ASD
An increased risk of ASD was also observed after exposure to both hypo- and hyperthyroidism. In a nested case-control study within a national birth cohort in Finland (26), Brown et al. observed a higher prevalence of elevated maternal thyroid peroxidase antibodies in cases of autism, whereas no difference in measures of maternal thyroid hormones was observed. The role of the immune system in the pathophysiology of ASD has been discussed (27). No data were available on thyroid autoantibodies in the present study. However, the association with unknown maternal overt thyroid disease in the present study and the previous findings (5) may signify that thyroid autoimmunity is not the only determinant. In the previous study (5), no association was found with maternal thyroid disease diagnosed before birth of the child or with paternal thyroid disease. The lack of an association with these exposures, and the predominant association in children exposed to maternal thyroid disease first diagnosed after birth of the child, may contradict an underlying autoimmune component to some extent. The association between overt hyperthyroidism and ASD in the present study is in contrast to the previous findings (5) and to other reports (28,29). Experimental studies have demonstrated that both lack and excess of thyroid hormone influence fetal brain development (18), but more studies in humans are warranted.
ADHD
In the present study, no overall association was observed between maternal thyroid dysfunction and ADHD. Much focus has been on smaller aberrations in maternal thyroid function (1,30). In line with previous studies (28,31), a higher risk of ASD and ADHD was observed in children exposed to maternal hypothyroxinemia, and multiplicative effect measure modification by child sex was observed. A study from Finland observed similar associations for ADHD symptoms in girls (32), whereas a study from the Netherlands (31) reported no interaction with child sex. Fetal sex differences in maternal human chorionic gonadotropin (hCG) have been considered, and higher concentrations in case of a female fetus have been proposed (33,34). Adding to this, a recent study showed that a lower hCG was associated with a higher risk of hypothyroxinemia (35). The frequency of maternal hypothyroxinemia in the random sample in the present study was of the same magnitude in women carrying a male and female fetus. On the other hand, symptoms of ADHD and comorbid problems may differ by the child's sex (36), and it is a possibility that risk factors and mechanisms of disease also differ in boys and girls. It is important to note that some of the neurodevelopmental disorders (e.g., ADHD) have seen a considerable increase in diagnostic activity in many countries over the latest decade (37), which could influence the diagnostic accuracy. In the present study, cases of ADHD were identified from a minimum of two redeemed prescriptions of drugs used for the treatment of the disorder, but it is acknowledged that this case-selection strategy did not include nonpharmacological interventions. Consequently, children with ADHD who did not receive medical treatment were classified as non-cases in the present study.
Methodological considerations
A strength of the present study is the measurement of maternal thyroid function from a large group of pregnant women combined with information on diagnosis and treatment of thyroid disease from nationwide registers. Still, the number of cases is small in the stratified analyses, and the confidence intervals are consequently wide. This weakens the conclusions based on the data. Method- and week specific reference ranges established in this cohort of women were used, as described in detail previously (7). No information was available on thyroid autoantibodies, but women diagnosed with thyroid or other autoimmune diseases or taking thyroid interfering medications were excluded from the cohort used for the establishment of reference ranges. It is acknowledged that maternal thyroid function was evaluated from a single measurement and may not reflect thyroid function throughout pregnancy, but major abnormalities were likely to be detected and correct (38).
The sub-cohort was randomly selected from a large population-based birth cohort and was comparable to the full eligible cohort of women who had a blood sample drawn. All children were followed up to 13 years of age, but information was only available on diagnosis in the DCPR up to December 31, 2007, and different results with a longer follow-up cannot be excluded. The definition of developmental disorders and febrile seizures relied on hospital diagnosis, and the validity of a diagnosis of ASD in the DCPR (39) and febrile seizures in the DNHR (40) was previously reported to be high. The completeness of a diagnosis of SDD is unknown. While it was possible to adjust for a number of potential confounders, unmeasured or residual confounding may still be present.
Perspectives
In conclusion, the results of this nationwide case-cohort study support the hypothesis of fetal programming by maternal thyroid abnormalities to some extent. Previous large register studies (4,5) generated the hypothesis of unidentified maternal thyroid dysfunction, and actual measurement of thyroid function in stored biobank samples showed that women diagnosed in the years after pregnancy had a high frequency of abnormal thyroid function in early pregnancy (8). The present study suggests that such undiagnosed abnormalities may increase the risk of some neurodevelopmental disorders in the child. Thyroid function was measured in a large number of pregnant women, and still the findings were diverse and differed by subtypes of exposure and outcome. Rather than opting for larger studies, future considerations may focus on alternative outcomes of child neurodevelopment. More evidence is needed on associations with subtypes and severity of abnormal maternal thyroid function and to understand the mechanisms and impact of smaller aberrations in maternal thyroid function.
Footnotes
Acknowledgments
We deeply acknowledge Professor Peter Laurberg, Department of Endocrinology, Aalborg University Hospital, Denmark, who passed away on June 20, 2016. Professor Peter Laurberg conceptualized and initiated the study, participated in the design, and was responsible for the biochemical analyses.
This work was supported by the Obel Family Foundation. This research has been conducted using the Danish National Biobank resource. The Danish National Biobank is supported by the Novo Nordisk Foundation. The Danish National Research Foundation has established the Danish Epidemiology Science Centre that initiated and created the DNBC. The cohort is furthermore a result of a major grant from this Foundation. Additional support for the DNBC is obtained from the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Augustinus Foundation, and the Health Foundation.
Author Disclosure Statement
Nothing to disclose.