
Abstract
Background:
Limited data suggest that treatment with statins is associated with a reduced risk of Graves' orbitopathy (GO) in patients with Graves' disease (GD), attributed to the anti-inflammatory rather than to the hypolipemic effects of these medications. The aim of the present study was to investigate whether there is an association between high cholesterol and GO. The primary outcome was the relation between GO and low-density lipoprotein (LDL)-cholesterol. The secondary outcomes were the relation between severity or activity (the clinical activity score [CAS]) of GO and LDL-cholesterol.
Methods:
A cross-sectional investigation was conducted in consecutive patients with GD who came under the authors' observation to undergo radioiodine treatment, a stratification aimed at forming two distinct groups of patients under the same conditions. A total of 250 patients were enrolled, 133 with and 117 without GO. Ophthalmological assessments and serum lipids measurements were performed.
Results:
In multivariate analyses with correction for the duration of hyperthyroidism, a variable that differed between patients with respect to the presence or absence of GO, a correlation between the presence of GO and both total (p = 0.01) and LDL-cholesterol (p = 0.02) was observed. In patients with hyperthyroidism lasting <44 months, total and LDL-cholesterol were higher (p = 0.01 and p = 0.008, respectively) among GO patients. In this subgroup, based on the presence/absence of GO, cutoff values were established for total (191 mg/dL) and LDL-cholesterol (118.4 mg/dL), above which an increased risk of GO was observed (total cholesterol relative risk: 1.47; p = 0.03; LDL-cholesterol relative risk: 1.28; p = 0.03). GO severity and CAS did not correlate with serum lipids. However, CAS was found to be higher (p = 0.02) in patients with high total cholesterol. When the analysis was restricted to untreated GO patients, a correlation was found between CAS and both total (p = 0.04) and LDL-cholesterol (p = 0.03), after adjustment for GO duration.
Conclusions:
In patients with a short duration of hyperthyroidism, total and LDL-cholesterol correlate with the presence of GO, suggesting a role of cholesterol in the development of GO. Depending on GO duration, total and LDL-cholesterol correlate with GO activity, suggesting a role of cholesterol in the clinical expression of GO.
Introduction
G
Statins are commonly employed for the treatment of hypercholesterolemia, a condition for which they are quite effective (21). They may show adverse reactions, and have been postulated to increase the risk of glucocorticoid-induced hepatitis in GO patients, although a population study was sufficiently reassuring (22). The possibility that the observed “protective” effect of statins on GO development may be a consequence of their hypolipemic actions was not considered, presumably due to the lack of association between GO and treatment with non-statin lipid-lowering medications, which was also assessed in the study of Stein et al., to the authors' knowledge the only investigation conducted on the subject (17). However, high cholesterol levels are associated with a general, altered, inflammatory state (23,24), which may be responsible for the observation of Stein et al. (17). In this regard, the absence of a significant association between GO and lipid-lowering medications other than statins may be explained by the fact that these medications have a lower potency in comparison to statins (25). It must also be taken into account that, although remarkable, the study from Stein et al. may possess some of the typical limitations attributed to retrospective investigations, as well as the fact that the data utilized were derived from a database and that comprehensive clinical data of the patients included were not examined (17). However, if, in contrast with the interpretation of Stein et al. (17), the effect of statins on GO development in GD patients reflected their hypolipemic actions, a relation between high serum cholesterol and the presence of GO in GD patients would be expected. In addition, the severity and activity of GO may differ based on the cholesterol levels. In order to investigate these possibilities, a cross-sectional study was conducted in consecutive patients with GD, aimed at determining whether there is a correlation between high serum cholesterol and GO.
The primary outcome of the study was the relation between the presence of GO and low-density lipoprotein (LDL)-cholesterol. The secondary outcomes were the relation between GO severity or activity and LDL-cholesterol.
Methods
Study design
The study was aimed at assessing the relation between GO and LDL-cholesterol in GD patients in a cross-sectional investigation. The research design entailed the inclusion of all consecutive GD patients, with or without GO, who came under the authors' observation to receive radioiodine treatment over a period of 18 consecutive months.
Setting
The study was performed in a tertiary referral center, namely the GO Clinic of the Endocrinology Units I and II and of the Ophthalmopathy Unit I of the University Hospital of Pisa, Italy. Patients were enrolled from January 1, 2016, to June 30, 2017. Patients were not selected but rather were included by means of consecutive sampling. The adopted inclusion and exclusion criteria are reported below. Data were collected by E.S., B.M., R.R., and F.M. and were recorded in a database. The study was not blinded. The following database validation procedures were employed: allowed character checks, batch totals, missing records check, cardinality check, digits check, consistency check, control totals, cross-system consistency check, data type check, hash totals, limit check, logic check, presence check, range check, spelling and grammar check, and uniqueness check.
Participants
The inclusion criterion comprised a diagnosis of GD in patients scheduled to undergo radioiodine treatment and who consequently discontinued antithyroid medications for two to three days. The exclusion criterion was earlier treatment of hyperthyroidism by methods other than antithyroid medications, namely thyroidectomy or radioiodine. A total of 250 consecutive patients who satisfied the inclusion criterion without the exclusion criterion were enrolled in the period reported above.
Outcomes
The primary outcome of the study was the observation of a relation between the presence of GO and LDL-cholesterol. The secondary outcomes were the observation of a relation between GO severity or activity (the clinical activity score [CAS]) and LDL-cholesterol. Concerning severity, both the NOSPECS score and the classification proposed by the European Group On Graves' Orbitopathy (EUGOGO) were used (26 –28). NOSPECS stands for no GO signs (N), only eyelid signs (O), soft tissue involvement (S), proptosis (P), extraocular motility restriction (E), corneal involvement (C), and sight loss (S), resulting in a numerical value, wherein each progressive class corresponds to a number from 1 to 6 (26). According to the EUGOGO classification, the severity of GO was defined as mild, moderately severe, or sight threatening (28). CAS was evaluated according to Mourits et al. (29,30). Additional outcomes were: (i) the relation between the presence of GO and total cholesterol, high density lipoprotein (HDL)-cholesterol, and triglycerides; (ii) the association between the presence of GO and high LDL-cholesterol, high total cholesterol, low HDL-cholesterol, and high triglycerides. In accordance with the recommendations of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) (25), LDL-cholesterol was considered high in the presence of values ≥115 mg/dL; total cholesterol was considered high when ≥190 mg/dL; HDL-cholesterol was considered low when ≤46 mg/dL in women and ≤40 mg/dL in men; and triglycerides were considered high when ≥150 mg/dL.
The presence of GO was established in any patient with a NOSPECS class ≥2, namely who had at least one of the following eye features: (i) exophthalmometry ≥17 mm in women and ≥19 mm in men, based on measurements conducted for the normal population (31 –35); (ii) eyelid aperture ≥9 mm (36); (iii) CAS ≥1/7; (iv) presence of diplopia; (v) presence of corneal alterations; (vi) presence of GO-related alterations of the fundi; and (vii) reduction in visual acuity that could be attributed to GO.
Sources of data and measurements
All patients underwent an ophthalmological assessment, which included the following procedures: (i) exophthalmometry; (ii) measurement of eyelid aperture; (iii) evaluation of CAS; (iv) assessment of diplopia; (v) assessment of the corneal status; (vi) examination of the fundi; and (vii) measurement of visual acuity. The following blood tests were performed: free thyroxine (fT4) and free triiodothyronine (fT3; Vitros Immunodiagnostics, Raritan, NJ); thyrotropin (TSH; Immulite 2000; Siemens Healthcare, Gwynedd, United Kingdom); anti-TSH receptor antibodies (TRAb; Brahms, Berlin, Germany); total cholesterol (Roche, Mannheim, Germany); LDL-cholesterol (Roche); HDL-cholesterol (Roche); and triglycerides (Roche). Smoking habits, physical activity (at least 30 minutes of exercise three times a week), dietary habits (roughly estimated daily calories in the last three days), and alcohol consumption (at least 50 g of ethanol/week) were recorded in all patients. The following conditions or treatments that can potentially affect cholesterol levels were recorded: diabetes, chronic renal failure, and therapy with statins, non-statin lipid-lowering medications, or other medications that could affect lipid levels, including estroprogestins, β-blockers, and thiazide diuretics.
Potential bias
The possible fluctuations of lipid levels over time, due to eating habits or seasonal variations, could constitute a possible drawback of this study, as the lipid profile was measured only once initially. In order to overcome this possible bias, patients were classified according to the month or season of enrollment.
As mentioned above, the study included patients with GD who came under the authors' observation to undergo radioiodine treatment. The objective of this stratification was to have two distinct groups of patients under the same conditions, namely off antithyroid medications for two to three days, therefore minimizing the effects of thyroid function changes on cholesterol levels, since both hyper- and hypothyroidism affect cholesterol (37).
As reported below, a minority of GO patients had been subjected to treatments that could have affected GO severity and activity. Therefore, in addition to the analysis of the total cohort of GO patients, separate data analyses were performed in the subgroup of GO patients who had not received treatment.
In theory, patients may have been affected by orbital diseases distinct from GO but bearing a certain resemblance to it, namely ocular myasthenia gravis or myositis (27,38). In the latter cases, an isolated diplopia and/or palpebral ptosis would have been expected, but none of the patients exhibited these attributes. Other conditions that can resemble GO are orbital lymphoma or inflammatory orbital pseudotumor, in which the findings commonly differ from GO at orbital computed tomography (CT) or magnetic resonance imaging, and hyperthyroidism is absent (27,39). A CT scan of the orbit was performed in 84/133 patients with an eye involvement, and it revealed alterations typical to GO across all cases (27). In addition, none of the patients displayed a reduction in visual acuity in the absence of other GO symptoms, all patients obtained a clear-cut diagnosis of Graves' hyperthyroidism with detectable TRAb, and the onset of hyperthyroidism and GO occurred within six months from one another in all cases, as reported previously in typical cases of GO (40). Therefore, the possibility of misdiagnosis of orbitopathies different from GO was highly improbable.
Sample size
Since, to the authors' knowledge, there were no previous studies on cholesterol levels and GO, an exact sample size could not be calculated. Based on an extrapolation derived from the study of Stein et al., namely, the assumption that the protective effect of statins on GO development was due to the lowering of cholesterol levels, and with the observation of a 40% GO reduction in patients treated with statins compared to GD patients who were not given statins (17), it was estimated that to obtain a statistically significant difference with a p-value of ≤0.05 and a statistical power of 0.8 for the primary outcome, at least 50 patients per group would be required. As reported above, 250 patients were enrolled, thereby largely exceeding this estimate.
Study registration, informed consent, and approval
The study was registered at
Quantitative variables
Numerical data with a normal distribution, which was assessed using the Wilks Shapiro test, are presented as mean ± standard deviation (SD). The remaining numerical data are presented as median and interquartile range. Cutoff values were established with the following formula: [(mean values in the non-affected population × SD in the affected population) + (mean values in the affected population × SD in the non-affected population)]/(SD in the affected population + SD in the non-affected population).
Statistical analyses
When appropriate, the following tests were performed: (i) t-test; (ii) Mann–Whitney U-test; (iii) chi-square test; and (iv) multiple regression analysis.
Results
Participants
As shown in Table 1, 117 patients without GO and 133 patients with GO were examined. The proportion of patients with GO was higher compared to that reported in previous studies (1). This reflects the fact that the study was carried out in a tertiary referral center, since, compared to primary care or secondary referral centers, a greater proportion of the GD patients who usually come under the authors' observation also suffer from GO (1). The two groups (patients with or without GO) were similar in terms of sex, familial history of hypercholesterolemia, extent of physical activity, alcohol consumption, body mass index (BMI), proportion of patients with conditions that could affect cholesterol levels (diabetes, chronic liver failure), proportion of patients taking medications that could affect cholesterol levels (statins, non-statin lipid-lowering medications, estrogens and progestins, β-blockers, thiazide diuretics), serum fT4, fT3, and TSH, and thyroid status. In contrast, age, smoking habits, duration of hyperthyroidism (time since the diagnosis of hyperthyroidism), and TRAb levels exhibited significant differences between the two groups. Thus, GO patients were on average older, and they tended to be more frequently smokers. In addition, the duration of hyperthyroidism was shorter and TRAb levels higher in patients with GO. It is worth emphasizing that only a minority of patients in each group suffered from conditions or took medications that could affect cholesterol, including statins. None of the patients was on glucocorticoids at the time of enrollment. However, 32/133 (24%) GO patients had been treated with intravenous glucocorticoids previously, more than three months before enrollment.
Numerical values are reported as mean ± SD or median and IQR, as appropriate. Statistically significant values are shown in bold.
p-Values were obtained by t-test, chi-square test, or Mann–Whitney U-test, as appropriate.
GO, Graves' orbitopathy; NS, not significant; BMI, body mass index; IQR, interquartile range; fT4, free thyroxine; fT3, free triiodothyronine; TSH, thyrotropin; TRAb, anti-TSH receptor autoantibodies; SD, standard deviation.
Primary outcome data: relation between the presence of GO and serum lipids
As shown in Table 2, serum levels of total cholesterol, LDL-cholesterol, HDL-cholesterol, and triglycerides did not show any difference between patients with or without GO. Since the two groups differed in terms of age, smoking habits, duration of hyperthyroidism, and TRAb, as mentioned above, multivariate regression analyses were performed with correction for each of the above-mentioned variables. While corrections for age, smoking, and TRAb did not affect the findings, correction for duration of hyperthyroidism did so significantly. Thus, there was a significant correlation between the presence of GO and both total and LDL-cholesterol when adjusted for duration of hyperthyroidism (p = 0.01 and p = 0.02, respectively).
Numerical values are reported as mean ± SD or median and IQR, as appropriate.
p-Values were obtained by t-test or Mann–Whitney U-test, as appropriate.
LDL, low-density lipoprotein; HDL, high-density lipoprotein.
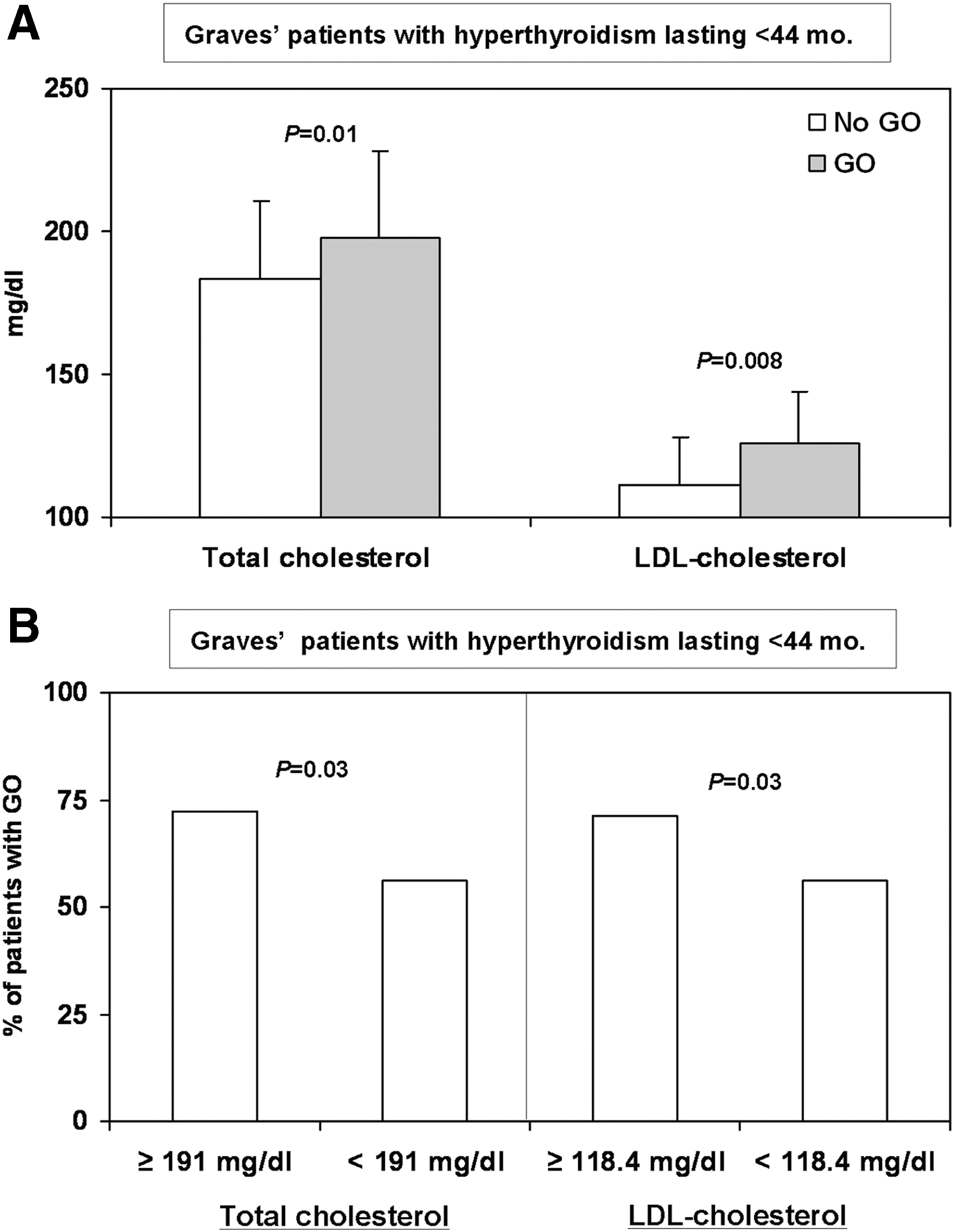
Based on the duration of hyperthyroidism in patients with or without GO, a cutoff value was established at 44 months, and the cohort was divided into two groups: one with a short (<44 months) and the other with a long (≥44 months) duration of hyperthyroidism. When the analysis was restricted to patients with a duration of hyperthyroidism <44 months (165 patients: 106 with GO and 59 without GO), both total and LDL-cholesterol levels resulted to be significantly higher in patients with GO (Fig. 1A), whereas HDL-cholesterol and triglycerides did not differ between the two groups (not shown). In contrast and as expected, when the analysis was restricted to patients with duration of hyperthyroidism ≥44 months (85 patients: 27 with GO and 58 without GO), serum lipids did not exhibit differences between patients with or without GO (not shown).
(
In patients with a duration of hyperthyroidism <44 months, based on the presence or absence of GO, cutoff values were established for total and LDL-cholesterol at 191 mg/dL and 118.4 mg/dL, respectively. Serum concentrations of total and LDL-cholesterol above these values were associated with a significantly increased risk of GO: total cholesterol relative risk (RR) = 1.47 [confidence interval (CI) 1.01–2.14], p = 0.03; LDL-cholesterol RR = 1.28 [CI 1.01–1.62], p = 0.03. The frequency of GO according to the presence of total or LDL-cholesterol concentrations above the cutoff values is illustrated in Figure 1B.
Subsequently, we analyzed the possible association between the presence of GO and the proportion of patients with high LDL-cholesterol, high total cholesterol, low HDL-cholesterol, and high triglycerides, all established in accordance with the recommendations of ESH and ESC (25). As demonstrated in Table 3, the proportion of patients with an alteration of the various serum lipid fractions did not differ between patients with and without GO. However, when the analysis was restricted to the 165 patients with a duration of hyperthyroidism <44 months, the proportion of patients with high total cholesterol was significantly greater in patients with GO (Table 4).
p-Values were obtained by chi-square test.
p-Values were obtained by chi-square test. Statistically significant values are shown in bold.
Secondary outcome data: relation between GO severity or activity and serum lipids
Among patients with GO, both the NOSPECS score, a measure of GO severity (26), and CAS, a measure of GO activity (29,30), did not appear to correlate with serum concentrations of total cholesterol, LDL-cholesterol, HDL-cholesterol, and triglycerides on univariate analysis (not shown). This was also the case when GO severity was determined using the EUGOGO classification (28) (not shown).
In the univariate analysis, the following variables showed significant correlations with NOSPECS: age (direct correlation, p = 0.005); sex (NOSPECS values 3.6 ± 1.0 in men and 3.1 ± 1.1 in women; p = 0.04), and TSH (direct correlation, p = 0.03). Similar findings were obtained when GO severity was assessed according to the EUGOGO classification, which in the univariate analysis also displayed a significant correlation with age (direct correlation, p = 0.01); sex (GO degree in men: mild 4/24 [16.6%], moderately severe 18/24 [75%], sight threatening 2/24 [8.4%]; GO degree in women: mild 44/109 [40.4%], moderately severe 59/109 [54.1%], sight threatening 6/109 [5.5%]; p = 0.04), and TSH (direct correlation, p = 0.01). Although this did not constitute an established aim of the present study, the former findings confirm the role of age, sex, and hypothyroidism as GO risk factors (4). In the multivariate analysis, adjustments for these three variables did not show a significant correlation between GO severity (assessed both using NOSPECS and the EUGOGO classification) and serum lipids.
By means of the univariate analysis, CAS displayed a significant correlation with age (direct correlation, p = 0.01), fT4 (inverse correlation, p = 0.03), fT3 (inverse correlation, p = 0.04), and TSH (direct correlation, p = 0.001), further confirming the role of age and hypothyroidism as GO risk factors (4). In addition, an inverse correlation was determined between CAS and GO duration (p = 0.02), reflecting the notorious early peak of CAS in the natural history of GO (41).
When multivariate analyses were performed in which the relation between CAS and total cholesterol, LDL-cholesterol, HDL-cholesterol, and triglycerides was adjusted for the variables correlated with CAS through the univariate analysis, no notable values of significance were obtained (not shown).
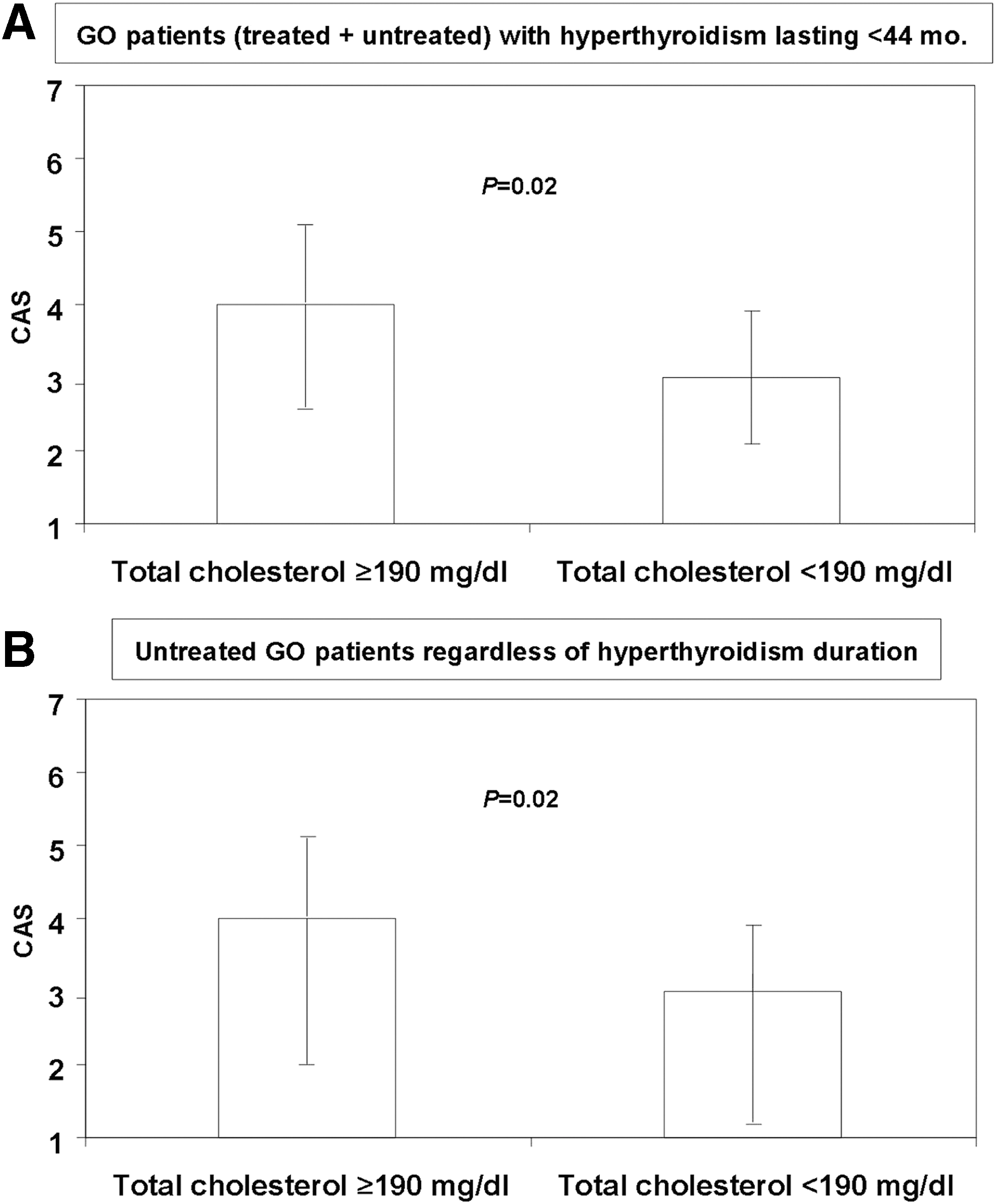
Subsequently, severity and activity measures were compared in GO patients, depending on the presence of high LDL-cholesterol, high total cholesterol, low HDL-cholesterol, and high triglycerides. As illustrated in Figure 2A, CAS values were significantly higher in GO patients with high total cholesterol. In contrast, no significant differences were observed with regards to GO severity (assessed both using NOSPECS and the EUGOGO classification; not shown).
(
The possibility was considered that the findings could have been compromised by the fact that some of the patients with GO had undergone previous treatments for their eye disease, as reported above. Therefore, the analysis was restricted to the 101 GO patients who had not received any previous treatment. Both severity (assessed using NOSPECS and the EUGOGO classification) and CAS did not correlate with serum concentrations of total cholesterol, LDL-cholesterol, HDL-cholesterol, and triglycerides by univariate analysis (not shown). Subsequently, multivariate analyses were performed in which the correlations with the various lipid fractions were adjusted for the variables that showed significant correlation with NOSPECS by univariate analysis in this subgroup of patients, namely sex (NOSPECS values 3.6 ± 1.1 in men and 2.9 ± 1.0 in women; p = 0.008) and TSH (direct correlation, p = 0.0097). Similarly, multivariate analyses were performed in which the correlations with the various lipid fractions were adjusted for the variables that showed significant correlation with GO severity according to the EUGOGO classification by univariate analysis, again sex (GO degree in men: mild 3/16 [18.7%], moderately severe 11/16 [68.8%], sight threatening 2/16 [12.5%]; GO degree in women: mild 41/85 [48.2%], moderately severe 42/85 [49.4%], sight threatening 2/85 [3.4%]; p = 0.009), and TSH (direct correlation, p = 0.03). In addition, multivariate analyses we performed with adjustments for the variables significantly correlated with CAS, namely age (direct correlation, p = 0.04) and GO duration (inverse correlation, p = 0.04).
The multivariate analyses confirmed the absence of a correlation between GO severity (assessed both using NOSPECS and the EUGOGO classification) and the various lipid fractions. However, adjustment for GO duration displayed a significant correlation of CAS with both total (p = 0.04) and LDL-cholesterol (p = 0.03), whereas adjustment for age had no effect. Finally, severity (both NOSPECS and EUGOGO classification) and CAS were compared in untreated GO patients in relation to the presence of high LDL-cholesterol, high total cholesterol, low HDL-cholesterol, and high triglycerides. As shown in Figure 2B, CAS values were significantly higher in GO patients with high total cholesterol. No other significant differences were observed (not shown).
Discussion
The present study was prompted by the observation of a reduced risk of GO in GD patients on statins for at least two months (17). The possibility was considered that the findings reflected the lowering of cholesterol rather than a direct anti-inflammatory effect of statins (17,18). Consequently, a cross-sectional study was conducted in consecutive patients with GD. A significant correlation was found between the presence of GO and both total and LDL-cholesterol in patients with a GD of relatively recent onset, suggesting a role of cholesterol in the development of GO. In addition, a correlation was found of CAS with total and LDL-cholesterol in untreated GO patients depending on GO duration, signifying a role of cholesterol in GO activity. Results in support of the conclusions are summarized and discussed in the following sections.
The study included the first 250 eligible consecutive patients with GD with or without GO who came under the authors' observation to undergo radioiodine treatment. As mentioned above, the aims of this stratification were to have two groups of patients under the same conditions and to minimize the effects of thyroid function on cholesterol levels, which can be affected by both hyper- and hypothyroidism (37). As a matter of fact, thyroid function did not differ between the two study groups. In spite of this stratification, some features displayed divergence among patients with or without GO, three of which—age, smoking, and TRAb—were somehow expected, since they are established GO risk factors (3 –16). An additional variable that differed between the two groups was the duration of hyperthyroidism, which was found to be significantly shorter in patients with GO. This probably reflects an arbitrary tendency in the authors' institution to treat Graves' hyperthyroidism more aggressively when it is found to be associated with GO (5,41,42). As a matter of fact, the former difference emerged to be of paramount importance in the interpretation of the results. Thus, when the analysis was adjusted for duration of hyperthyroidism, multiple regression modeling provided evidence for a significant direct correlation between the presence GO and the levels of total and LDL-cholesterol, thereby fulfilling the primary outcome of the study. In addition, when the analysis was restricted to patients with a short duration of hyperthyroidism (<44 months), total cholesterol and LDL-cholesterol were found to be significantly higher in patients with GO. In the former population of patients with a GD of recent onset, based on the presence or absence of GO, cutoff values were established for total cholesterol at 191 mg/dl and for LDL-cholesterol at 118.4 mg/dL, and it was found that levels above these values were associated with a significantly increased risk of GO. Still, in the former population, the proportion of patients with high total cholesterol was significantly greater in patients with GO.
Overall, the fact that the relation between GO and cholesterol was restricted only to patients with GD of recent onset could be somehow anticipated. In GD patients, there is a close temporal relation between the occurrences of hyperthyroidism and GO, and GO only very rarely manifests itself >12 months after the onset of hyperthyroidism (40). This implies that risk factors for GO are more readily identified in patients with GD of recent onset compared to patients with long-standing disease, in whom GO occurrence is a very rare event (40). In this context, it is interesting to note that the observations of Stein et al., who, as mentioned above, found a protective role of statins in terms of GO development, were obtained in patients with GD of recent onset (17).
In patients with GO, the severity and activity appeared to be minimally affected by serum lipids, even though CAS values were significantly higher in GO patients with high total cholesterol. The possibility was considered that the findings may have been compromised by the fact that some patients had undergone intravenous glucocorticoid treatment for GO before enrollment, with a consequent improvement of GO. Therefore, the analysis was restricted to untreated GO patients, and a significant correlation was found by multivariate analysis with adjustment for GO duration (a variable that correlated with CAS by univariate analysis) between CAS and both total and LDL-cholesterol. In this subgroup of patients and in the confirmation of the findings obtained from the total cohort of GO patients, CAS was significantly higher in those with high total cholesterol. Overall, these data suggest the possibility that not only is cholesterol a possible GO risk factor, but also that it may be associated with more active forms of the eye disease.
One possible limitation of this study is that severity and activity of GO in the cohort may not have been necessarily the worst possible in each individual patient. In this regard, it would have been interesting to investigate whether GO outcomes after treatment is affected by lipid levels. However, this aspect could not be examined, since, after radioiodine therapy, patients were given different types of treatment that rendered the population highly heterogeneous. Another limitation is related to the possible fluctuations of lipid levels over time, due to eating habits or seasonal variations, as the lipid profile in the patients was measured only once at enrollment. Nevertheless, when patients were grouped according to the month or the season of enrollment, no differences were observed (not shown).
The mechanisms responsible for the relation between the presence of GO and cholesterol in patients with a GD of recent onset are not known and require further investigation. One hypothesis is related to the altered inflammatory state of hypercholesterolemia that may in particular explain the above-mentioned correlation of GO activity with total and LDL-cholesterol. It is well known that disorders of lipid metabolism are associated with a state of mild-to-moderate, systemic, chronic inflammation (23,24). The increased load of free fatty acids in the liver, present in hyperlipemic states, causes dysfunction of the mitochondria and endoplasmic reticulum of hepatocytes, leading to the release of reactive oxygen radical species (23). In addition, free fatty acids can indirectly cause the release of pro-inflammatory cytokines, namely interleukin-6 and tumor necrosis factor-α, both involved in the pathogenetic mechanisms of GO (19,20). The present study could not establish an association between GO and high triglycerides, which argues against the possibility that free fatty acids are in some way involved in GO. In support of an altered inflammatory state in hypercholesterolemia as the cause underlying our findings, Busnelli et al. observed a protective effect of statins in terms of systemic inflammation in a porcine model (24). In any case and rather evidently, the explanations for the relation between hypercholesterolemia and GO are entirely speculative and require further investigation.
In conclusion, this study reveals a relation between the presence and the activity of GO and the levels of cholesterol in patients with GD and GO of comparatively recent onset. The findings may have important clinical implications, as they may unravel a new field in GO management and prompt the necessity for further studies aimed at investigating if lowering cholesterol levels is associated with improved GO outcomes.
Footnotes
Author Disclosure Statement
The authors declare that they do not have any commercial association that might create a conflict of interest in connection with this manuscript.