
Abstract
Background:
Evidence has shown that programmed cell death ligand 1 (PD-L1) overexpression is associated with poor prognosis and resistance to immune therapies in several human cancers. However, data on the prognostic significance of PD-L1 expression in thyroid cancer are limited and remain controversial. This systematic review and meta-analysis aimed to evaluate comprehensively the clinicopathologic significance and prognostic value of PD-L1 expression in non-medullary thyroid cancers.
Methods:
Electronic databases, including Medline/PubMed, EMBASE, and the Cochrane Library, were searched up until July 5, 2017. In total, seven comparisons (from six articles) comprising 1421 patients were included in the pooled analysis.
Results:
There was moderate quality evidence from four studies (n = 721) that shows positive PD-L1 expression was significantly associated with poor survival among thyroid cancer patients (pooled hazard ratio = 3.73 [confidence interval (CI) 2.75–5.06]). Increased PD-L1 expression was also found to be significantly associated with disease recurrence (odds ratio = 1.95 [CI 1.15–3.32]) and concurrent thyroiditis (odds ratio = 1.65 [CI 1.09–2.51]).
Conclusions:
The results confirm the prognostic significance of PD-L1 expression in thyroid cancer patients. PD-L1 expression has the potential to be implemented as a prognostic biomarker used to guide clinicians in identifying patients with more aggressive cancers, and for the selection of individuals that would derive durable clinical benefit from anti-PD-1/PD-L1 immunotherapy. Prospective clinical trials will be useful to support these findings.
Introduction
O
Treatment of patients with differentiated thyroid cancer (DTC; both papillary and follicular [FTC] histologies) typically consists of surgical resection, hormone-suppressive therapy, and the selective use of radioactive iodine (RAI) to ablate residual thyroid tissue and eradicate any suspected micrometastases or recurrent disease (7). However, for patients with RAI-refractory and metastatic DTC, therapeutic options are presently limited (8). In patients with RAI-resistant tumors, the 10-year survival rate falls from approximately 60% to only 10% (9). Additionally, 2% of patients advance to develop anaplastic thyroid cancer (ATC) (10). While rare, ATCs are a particularly aggressive and rapidly fatal form of thyroid cancer associated with a median survival of only three to five months (11) and a five-year survival rate of 0–10% (12). Anaplastic thyroid cancer may arise de novo. However, in most cases, it represents a terminal dedifferentiation from a pre-existing well-differentiated thyroid carcinoma (WDTC) (13). A few studies have shown that multimodal therapy comprising of surgery, chemotherapy, and radiotherapy may improve survival outcomes in select patients. Unfortunately, despite combination treatment, most patients die from uncontrolled local tumor invasion or distant metastases (14). Therefore, it is essential that novel biomarkers are identified and validated in order to best inform clinical decision making and improve patient outcomes.
Programmed cell death 1 (PD-1; CD279), a member of the B7-CD28 superfamily, is a type 1 transmembrane protein expressed by T, B, and natural killer (NK) cells following activation (15). Its ligand, programmed cell death ligand 1 (PD-L1; B7-H1; CD274) is constitutively expressed on specific tumor and immune cells, including activated B and T cells, dendritic cells, and macrophages (15). Binding of PD-L1 to PD-1 can impede T-cell activation, disrupt cytokine production, and induce the apoptosis or exhaustion of effector T cells, resulting in tumor growth (16,17). Accumulating evidence has shown that PD-L1 overexpression is associated with poor prognosis and resistance to immune therapies in several human cancers (18 –21). Blockade of the PD-1/PD-L1 signaling pathway with targeted monoclonal antibodies has emerged as a promising therapeutic approach in cancer, demonstrating encouraging antitumor activity and eliciting durable clinical responses in multiple tumor types (17). Ongoing research is now focused on identifying biomarkers that can predict a favorable clinical response and guide patient selection for anti-PD-1/PD-L1 therapy (22,23).
Research informing the prognostic significance of PD-L1 expression in thyroid cancer is limited and remains controversial (24 –29). In certain studies, positive PD-L1 expression has been associated with a significantly poorer prognosis. However, others have failed to replicate these findings. A recent study has identified almost no expression of PD-L1 in medullary thyroid cancer (MTC) cells and accompanying tumor-infiltrating immune cells (30). To the authors' knowledge, no systematic review investigating this topic has been published thus far. In this systematic review, a meta-analysis was performed to evaluate comprehensively the clinicopathologic significance and prognostic value of PD-L1 expression in non-MTCs.
Methods
Literature search
Two authors (M.A. and S.G.) independently performed a comprehensive literature search of published articles using the Medline/PubMed, EMBASE, and Cochrane Library databases. The final search was conducted on July 5, 2017. Discrepancies were resolved by mutual discussion. The following keywords were employed for literature retrieval: (“PD-L1” or “PDL1” or “B7-H1” or “B7 homolog 1” or “CD274” or “Programmed Death Ligand 1”) and (“thyroid cancer” or “thyroid neoplasm” or “thyroid carcinoma” or “thyroid tumor”). A manual search through the reference lists of the articles and related reviews was also conducted.
Eligibility criteria
The criteria for inclusion encompassed the following: (i) studies were focused on non-MTC; (ii) all patients were histologically confirmed as having non-MTC; (iii) The expression of PD-L1 was tested using immunohistochemistry (IHC) staining on tumor cells and/or tumor-infiltrating lymphocytes (TILs) in primary cancer tissues; (iv) PD-L1 protein expression was assessed on the cell membrane, cytoplasm, or both; (v) The study provided an association between PD-L1 expression with clinicopathologic features and/or prognosis; and (vi) articles were published as a full paper in English. Studies that did not meet the inclusion criteria were excluded. In the case where duplicate publications from the same center were identified, only the article with the newest or most relevant information was included.
Data extraction
From each included study, the following information was extracted independently by two authors (M.A. and S.G.): name of the first author, year of publication, country of origin, tumor type, number of cases, tumor-node-metastasis (TNM) stage, IHC staining pattern, cutoff values for PD-L1 positive expression, antibody, PD-L1 status, survival outcome, and quality assessment score. Any discrepancies between the two authors were resolved by consensus. The primary outcome measure was disease-free survival (DFS), which was defined as the time period between completion of primary treatment and detection of residual disease, recurrent disease, or death. Following initial therapy, absence of persistent tumor was defined as (i) no clinically detectable thyroid cancer, (ii) no imaging evidence of tumor via RAI imaging and/or neck ultrasound, or (iii) low serum thyroglobulin (Tg) during thyrotropin suppression (Tg <0.2 ng/mL) or following stimulation (Tg <1 ng/mL) with negative thyroglobulin antibodies (7). Hazard ratios (HRs) with corresponding confidence intervals (CIs) were extracted from tables and used to report on the association between PD-L1 expression and DFS. Odds ratios (ORs) were used to evaluate the relationship between positive PD-L1 expression and the following factors: sex, age, tumor size, TNM stage, local/distant recurrence, extrathyroidal extension (ETE), multifocality, lymph node metastasis, and concurrent lymphocytic thyroiditis. When both univariate and multivariate analyses were reported, HRs and CIs were preferentially included from multivariate analysis. In instances where HRs and CIs were not reported, corresponding authors were contacted.
Assessment of study quality
Two authors (M.A. and S.G.) independently assessed the quality of all included studies according to the Newcastle–Ottawa Quality Assessment Scale (NOS). Disagreements in scoring were resolved by discussion between the authors. The NOS evaluates the following three parameters: selection (0–4 points), comparability (0–2 points), and outcome (0–3 points). The maximum NOS score is nine points, with studies scoring greater than five considered to be of high quality.
An overall quality assessment rating was given using an adapted version of the GRADE criteria (31). Briefly, the quality of evidence was downgraded a level for each of the following factors: poor study design (25% or more of trials, weighted by sample size, have a low NOS score [<5/9]), inconsistency of results (25% or more of the trials, weighted by sample size, have results which are not in the same direction), imprecision (sample size <300), and publication bias (Egger's regression two-tailed p-value was <0.10). The quality of evidence was classified as “high quality,” “moderate quality,” “low quality,” and “very low quality.” The study did not assess for indirectness (where the trial context, for example setting, patients, intervention, comparison, or outcomes, is not exactly the same as the review question), as we were looking at a specific study population (people with non-MTC).
Statistical methods
Pooled HRs and ORs with their CIs were used to evaluate the association between PD-L1 expression with DFS and clinicopathologic parameters, respectively. Patients were dichotomized by sex (male vs. female), age (<45 years vs. ≥45 years), tumor size (<2 cm vs. ≥2 cm), TNM stage (I–II vs. III–IV), local/distant recurrence (+recurrence vs. –recurrence), ETE (+ETE vs. –ETE), multifocality (+MF vs. –MF), lymph node metastasis (+N vs. –N), and concurrent lymphocytic thyroiditis (+thyroiditis vs. –thyroiditis). Subgroup analysis was performed based on tumor type (DTC vs. ATC). Heterogeneity among studies was assessed using the chi-square test and I 2 metric. A random-effects model was implemented when there was evidence of significant heterogeneity (i.e., I 2 statistic >50%). Further analysis was performed to identify the causes of heterogeneity. Potential publication bias was assessed using the Egger linear regression test and Begg funnel plot. The meta-analysis was performed with Review Manager v5.3 (Revman the Cochrane Collaboration, Oxford, England) and Comprehensive Meta-Analysis v3.0 (Biostat, Englewood, NJ). Statistical tests were all two-sided, with p-values <0.05 considered statistically significant.
Results
Search results
In the present study, 71 articles were identified using the initial search strategy. Duplicate studies were identified and removed, with a total of 56 studies remaining. After screening the titles and abstracts, 44 studies were excluded on the basis that they were not original articles (e.g., review, letter, case report), not thyroid cancer-related studies, not English language papers, not human studies, were conference abstracts, or were irrelevant. After reading 12 potentially suitable articles in detail, it was determined that six satisfied the inclusion criteria. Details of the screening process are depicted in Figure 1.
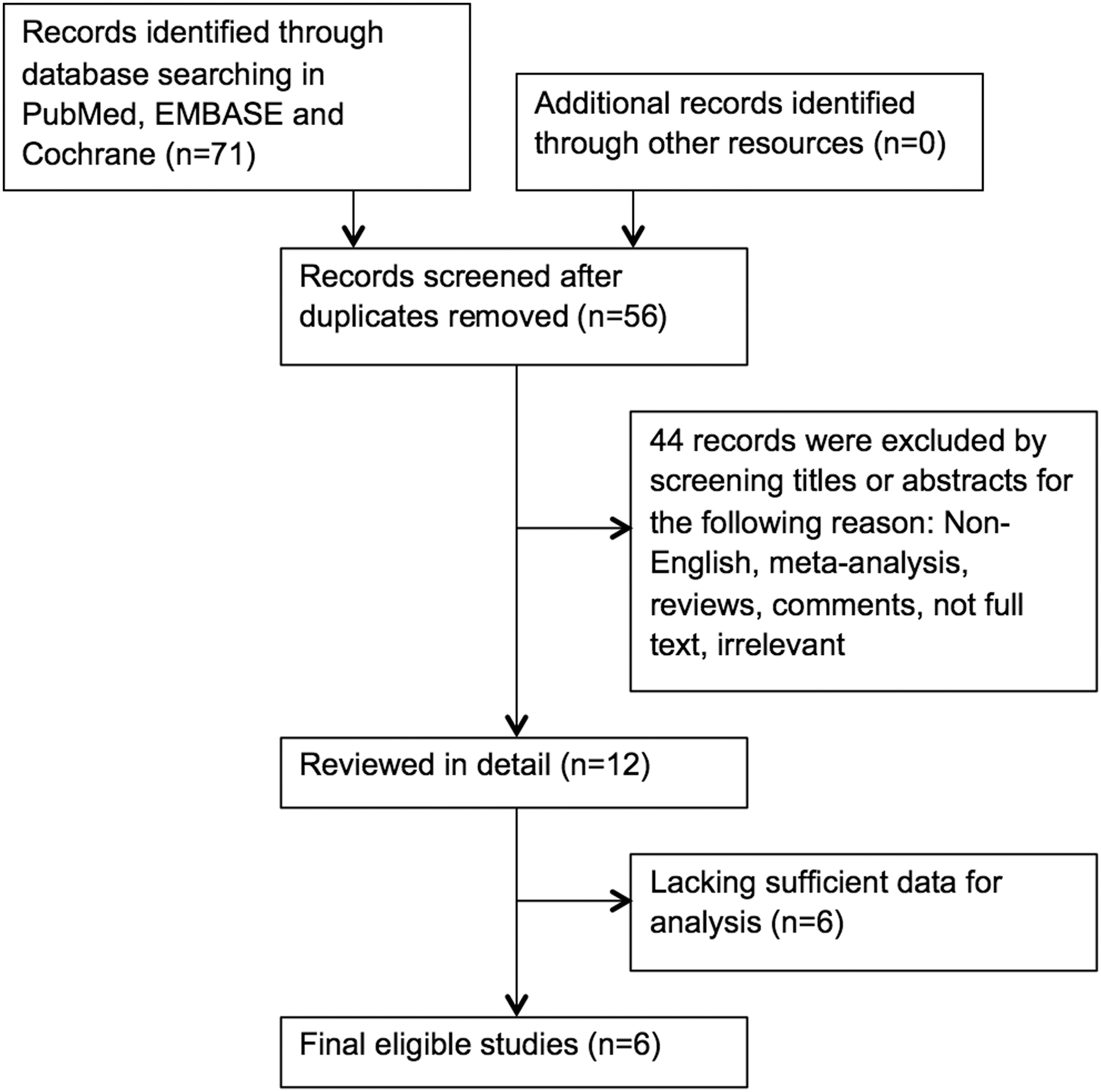
Flow diagram of study selection.
Study characteristics
The characteristics of the included studies are presented in Table 1. The studies were generally of high quality, with a mean NOS score of 6.1 (range 5–7). Of note, the single article by Chowdhury et al. provided two independent comparisons on the basis that membranous and cytoplasmic PD-L1 staining was scored and reported separately. Thus, in total, seven comparisons (from six articles) comprising 1421 patients were included in the pooled analysis. PD-L1 overexpression was found in 660 (46.4%) patients. The year of publication of the eligible studies ranged from 2013 to 2017. In all seven comparisons, PD-L1 expression levels were measured in tumor cells and/or TILs via IHC staining. PD-L1 expression was identified on the cell membrane, cytoplasm, or both. Each article had a distinct cutoff value used to define positive and negative PD-L1 expression. For this review, patients were considered to be scored positive for PD-L1 based on the specific cutoff criteria reported in each study. DFS was used as the endpoint in five of the seven comparisons (24,25,27,28,32). Due to the absence of detailed data regarding DFS from the original study by Cunha et al., this comparison could not be included in the final analysis. Recurrence-free survival and progression-free survival were implemented by the remaining two comparisons (26,29). As overall survival was only evaluated in one study, it was not investigated in the meta-analysis.
IHC, immunohistochemistry; PD-L1, programmed cell death ligand 1; PTC, papillary thyroid cancer; FTC, follicular cell cancer; PDTC, poorly differentiated thyroid cancer; ATC, anaplastic thyroid cancer; DTC, differentiated thyroid cancer; DFS, disease-free survival; PFS, progression-free survival; OS, overall survival; RFS, recurrence-free survival.
PD-L1 as a prognostic factor for thyroid cancer
The study evaluated the association between PD-L1 expression and DFS from four studies (involving five comparisons). These comparisons utilized cytoplasmic ± membranous staining techniques to measure PD-L1 levels. The pooled HR, involving 721 patients, provided moderate quality evidence (downgraded, as there was evidence of publication bias; Egger p-value = 0.08) that positive PD-L1 expression was significantly associated with poor survival among thyroid cancer patients (HR = 3.73 [CI 2.75–5.06]; see Fig. 2A).
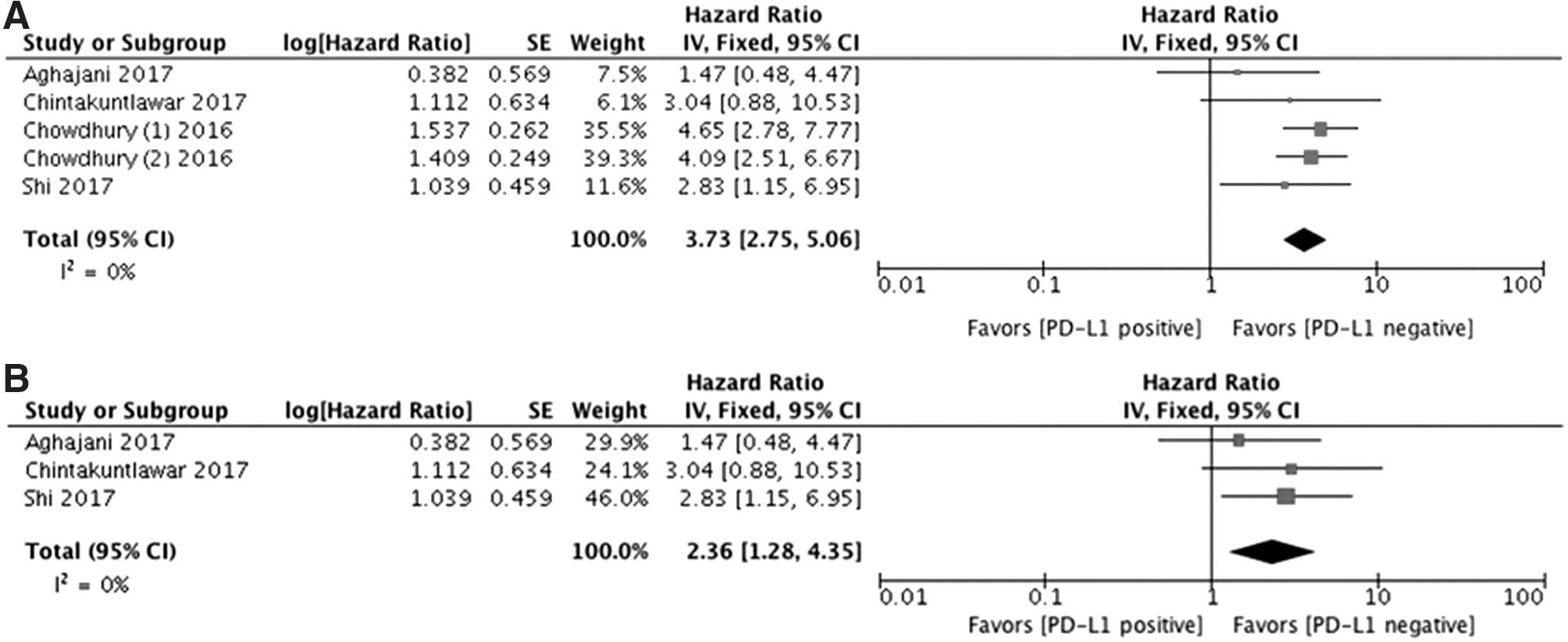
Forest plot of studies evaluating the association between programmed cell death ligand 1 (PD-L1) expression and survival in patients with thyroid cancer. (
A subgroup analysis including only those studies in which both cytoplasmic and membranous staining were measured, provided high-quality evidence that elevated PD-L1 expression was significantly associated with a reduced DFS (HR = 2.36 [CI 1.28–4.35]; see Fig. 2B).
Further, subgroup analysis based on histological thyroid cancer subtype was performed, providing high-quality evidence that increased expression of PD-L1 was significantly associated with a reduced DFS in DTC (HR = 3.78 [CI 2.76–5.18]; see Fig. 3A). However, elevated PD-L1 expression was not significantly associated with a reduced DFS in ATC patients (HR = 3.04 [CI 0.88–10.53]; see Fig. 3B). The overall quality of evidence rating for this finding is very low (downgraded for inconsistency of results, imprecision, and publication bias).

Forest plot of studies evaluating the association between PD-L1 expression and survival in patients with thyroid cancer. (
Association between PD-L1 expression and clinicopathologic features
Sex
Pooled results from five comparisons (n = 948) suggest there is no statistically significant association between PD-L1 expression and sex (OR = 1.17 [CI 0.79–1.73]; refer to Fig. 4A). The overall quality of evidence rating for this finding is high.
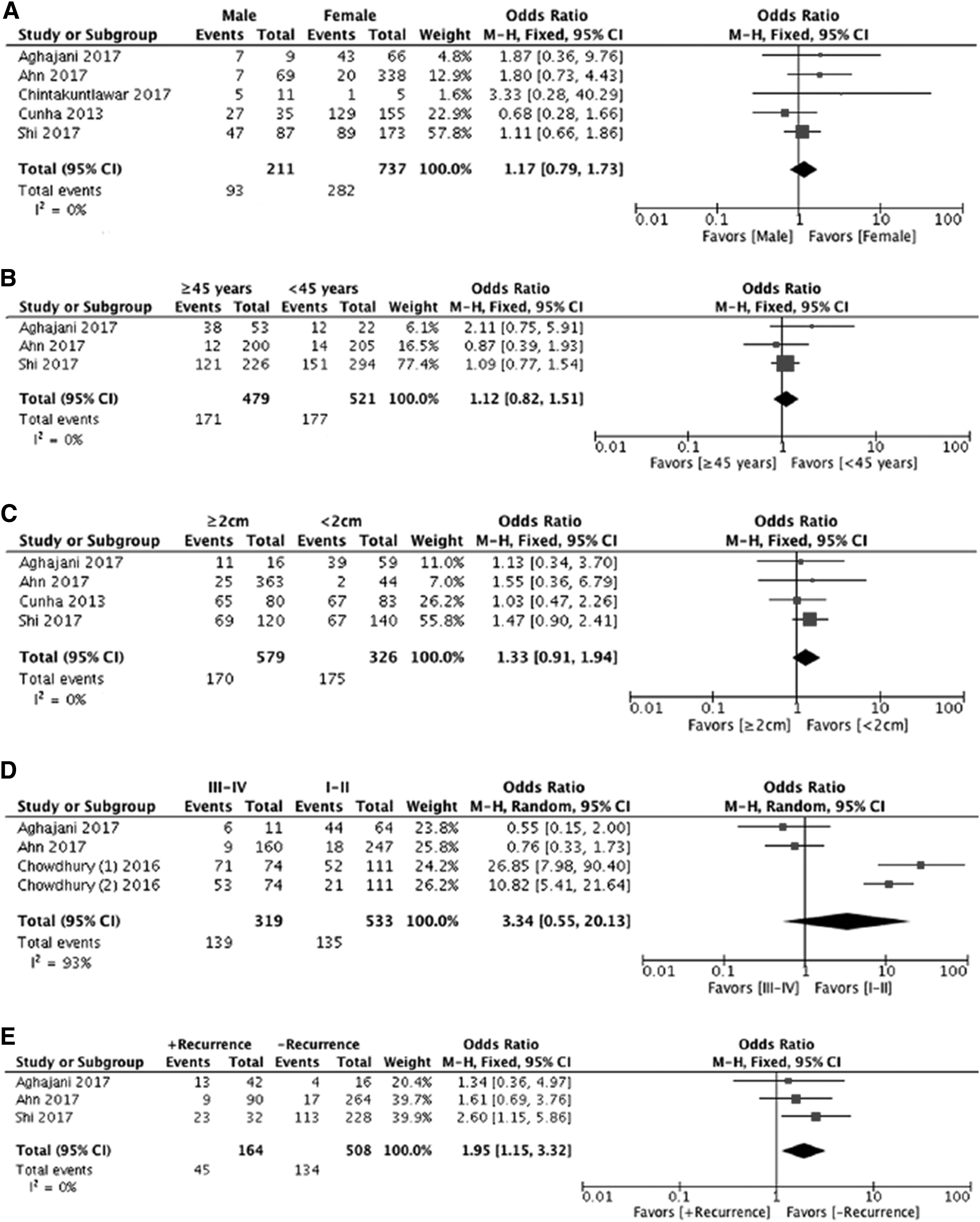
Forest plots of the association between PD-L1 expression and clinicopathologic characteristics of non-medullary thyroid cancer.

Age
We evaluated the association between PD-L1 expression and age in a total of 1000 patients from three studies (Fig. 4B). Pooled effects showed there was no significant association between PD-L1 expression and age (OR = 1.12 [CI 0.82–1.51]). The overall quality of evidence rating for this finding is high.
Tumor size
Pooled results from four studies (n = 905) showed that high PD-L1 expression was not significantly associated with a larger thyroid tumor size (OR = 1.33 [CI 0.91–1.94]; see Fig. 4C). The overall quality of evidence rating for this finding is high.
Stage
Four studies, including 852 patients, were analyzed for the association between PD-L1 expression and TNM stage (Fig. 4D). Positive PD-L1 expression was more evident in late-stage cancer compared to early-stage cancer (OR = 3.34 [CI 0.55–20.13]). However, this result was not statistically significant and had high heterogeneity (p < 0.00001; I 2 = 93%). Thus, it should be considered with caution. The overall quality of evidence for this finding is moderate (downgraded for inconsistency of results).
Disease recurrence
The association between PD-L1 expression and local/distant recurrence was evaluated in a total of 672 patients from three studies (Fig. 4E). Of the people with positive PD-L1 expression, 45/164 (27.4%) had +Recurrence and 134/508 (26.4%) had –Recurrence, with an OR of having recurrence of 1.95 [CI 1.15–3.32]. Hence, increased PD-L1 expression was found to be significantly associated with disease recurrence (OR = 1.95 [CI 1.15–3.32]). The overall quality of evidence rating for this finding is high.
ETE
No statistically significant relationship was detected between PD-L1 expression and ETE based on pooled data from three studies (n = 595; OR = 1.02 [CI 0.60–1.72]; Fig. 4F). The overall quality of evidence rating for this finding is high.
Multifocality
Six of the studies, including 1271 patients, examined the relationship between PD-L1 expression and multifocality (Fig. 4G). The pooled OR provided high-quality evidence that PD-L1 expression had no clear association with multifocality (OR = 0.83 [CI 0.61–1.14]).
Lymph node metastasis
Three studies comprising 1000 patients were evaluated for the association between PD-L1 expression and lymph node metastasis (Fig. 4H). The pooled results showed there was no statistically significant association between PD-L1 expression and lymph node metastasis (OR = 1.13 [CI 0.83–1.54]). The overall quality of evidence rating for this finding is high.
Concurrent thyroiditis
A total of four studies, including 906 patients, were analyzed for the association between PD-L1 expression and concurrent thyroiditis (Fig. 4I). Of the people with positive PD-L1 expression, 107/188 (56.9%) had +Thyroiditis and 239/718 (33.3%) had –Thyroiditis, with an OR of having thyroiditis of 1.65 [CI 1.09–2.51]. Hence, positive PD-L1 expression was significantly associated with concurrent thyroiditis, and the quality of evidence for this finding is high.
Subgroup analysis by tumor type
Subgroup analysis comprising studies evaluating PD-L1 status in patients with non-medullary DTC provided high-quality evidence that elevated PD-L1 expression was significantly associated with an increased incidence of recurrent disease (HR = 2.18 [CI 1.09–4.33]; see Fig. 5A) and concurrent Hashimoto's thyroiditis (HR = 1.71 [CI 1.09–2.70]; see Fig. 5B). However, in this subgroup, PD-L1 expression was not significantly associated with sex (HR = 1.04 [CI 0.67–1.60]; see Fig. 5C), age (HR = 1.17 [CI 0.84–1.62]; see Fig. 5D), tumor size (HR = 1.31 [CI 0.88–1.94]; see Fig. 5E), stage (HR = 5.60 [CI 0.78–40.10]; see Fig. 5F), ETE (HR = 1.10 [CI 0.57–2.13]; see Fig. 5G), multifocality (HR = 0.79 [CI 0.56–1.11]; see Fig. 5H), or lymph node metastasis (HR = 1.66 [CI 0.50–5.53]; see Fig. 5I).
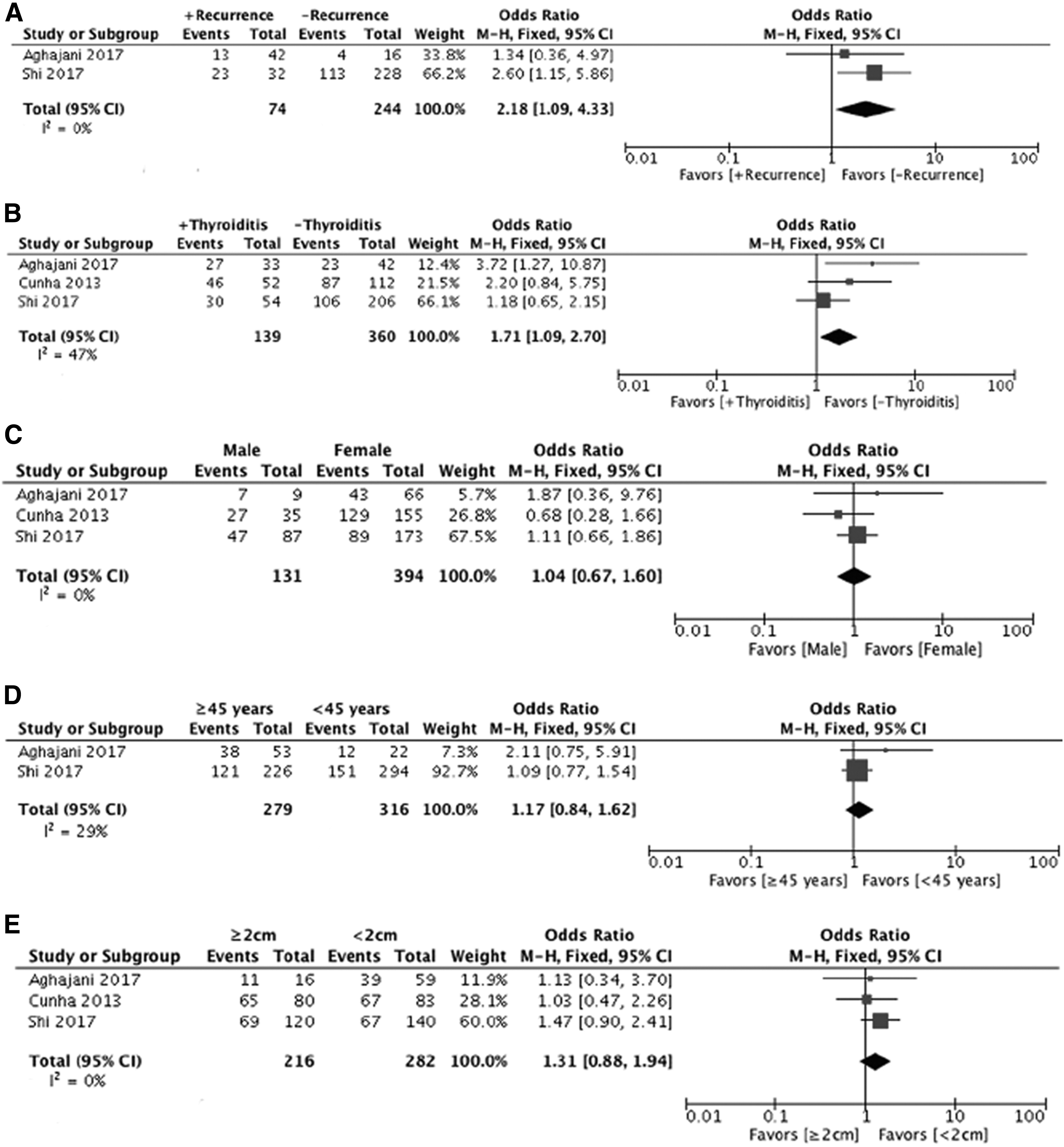
Forest plots of the association between PD-L1 expression and clinicopathologic characteristics of patients with DTC.
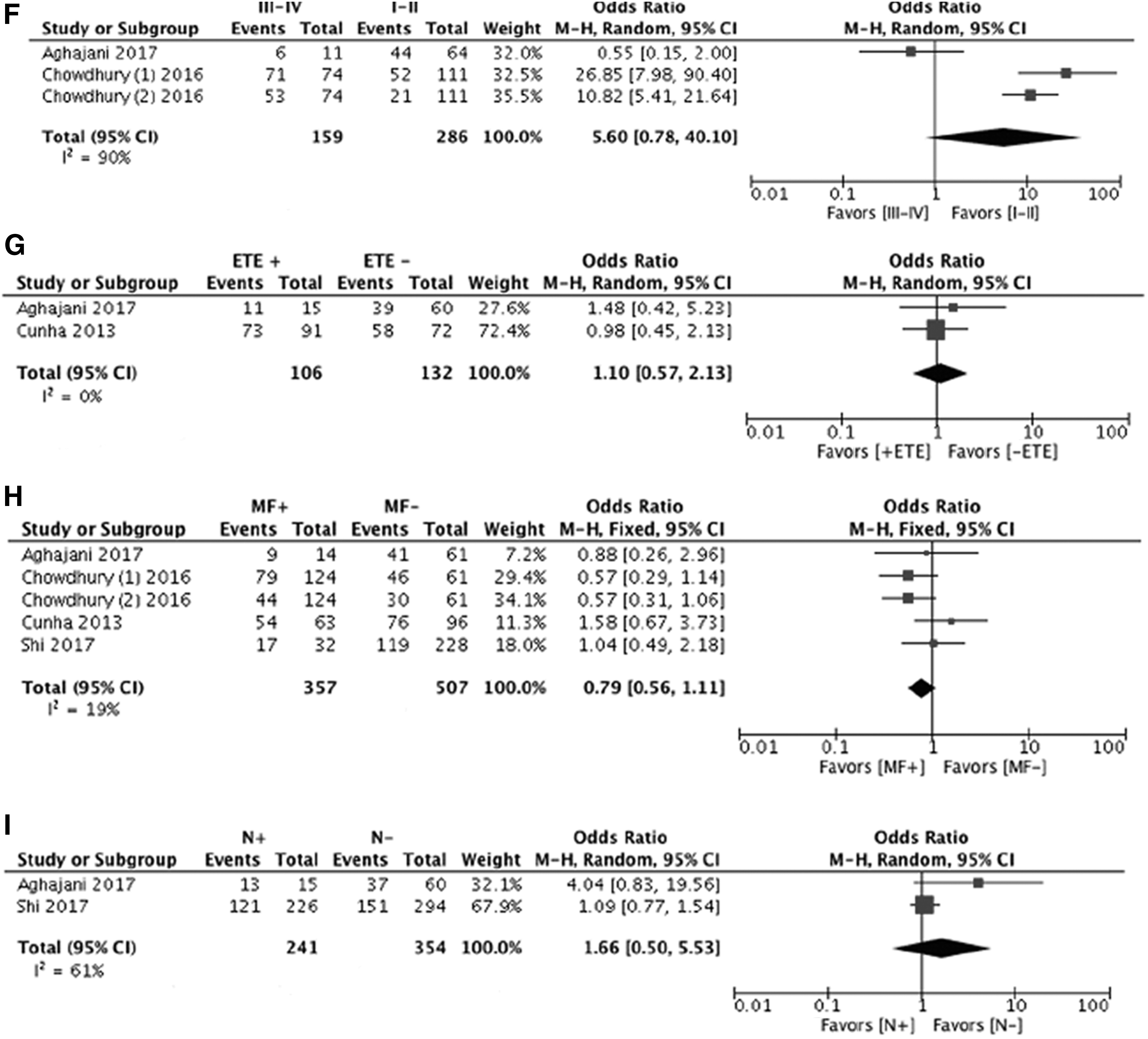
Heterogeneity was observed in the analysis of PD-L1 expression with TNM stage (p < 0.00001; I 2 = 93%), and in the subgroup analysis with lymph node metastasis (p = 0.11; I 2 = 61%) and TNM stage (p < 0.0001; I 2 = 90%). Thus, a random-effects model was employed. The remaining analyses were performed applying a fixed-effects model.
Publication bias and sensitivity analysis
Egger's test indicated the presence of significant reporting bias in regards to survival (Egger's test, p = 0.08). However, Egger's test did not identify significant reporting bias in the remaining outcomes assessed.
Discussion
To the best of the authors' knowledge, the present meta-analysis is the first to investigate the association between PD-L1 expression and clinical outcomes in thyroid cancer. This study provided moderate to high-quality evidence that elevated PD-L1 expression was significantly associated with DFS in the present cohort of thyroid cancer patients. It would appear that patients with positive PD-L1 expression are up to three times more likely to have a poorer DFS than participants who did not have positive PD-L1 expression. Furthermore, the results revealed that patients with disease recurrence and concurrent thyroiditis tended to have higher levels of PD-L1 expression.
This study has several strengths. First, an amended GRADE approach was used to assess the quality of evidence. Second, a systematic and rigorous search was implemented when identifying observational studies investigating the prognostic capabilities of PD-L1 expression in non-MTCs. Third, the pooled analysis was comprised of studies of similar designs measuring comparable outcomes, which minimized methodological heterogeneity.
There are certain limitations that require consideration when interpreting the results of this review. First, the number of studies included in the analysis was relatively small. Second, this meta-analysis was restricted to articles published in English. Third, cutoff values used to establish high or low PD-L1 expression varied between the studies. Furthermore, the antibodies, experimental procedures, immunohistochemical reagents, and scoring methods used to determine these cutoff values also differed. To address these inconsistencies, subgroup analysis was performed in which only studies evaluating both cytoplasmic and membranous PD-L1 staining were included. Future investigations employing uniform evaluation methods will generate more reliable results. Finally, two of the primary studies did not provide sufficient data to deduce HRs and their CIs, and were not included in the final analysis. In the future, additional multicenter studies will be necessary to support the routine use of PD-L1 expression as a prognostic biomarker in thyroid cancer.
PD-L1 overexpression has been shown to play a vital role in the generation of an immunosuppressive tumor microenvironment, with PD-1/PD-L1 interactions inhibiting effector T-cell activation and preventing the immune-mediated lysis of tumor cells (33). In accordance with the results, elevated PD-L1 expression has been strongly correlated with poor prognosis in a number of human malignancies (34). However, inconsistent results have been reported in lung cancer, colorectal cancer, and melanoma, with PD-L1 expression demonstrating both positive and negative predictive value (35). As mentioned previously, inconsistencies between assays, site of PD-L1 assessment, and undefined cutoff values are possible reasons for the irregularities between results.
For patients with non-MTC, the association between PD-L1 expression and prognosis was largely inconclusive. While some studies have shown that positive PD-L1 expression is associated with a significantly poorer prognosis and adverse clinicopathologic features, others have not confirmed these findings. In 2013, Cunha et al. reported more diffuse PD-L1 expression in DTC when compared to benign tissues. However, their results did not confirm PD-L1 expression as a diagnostic marker by IHC (28). Aghajani et al. observed no significant trend between elevated PD-L1 expression and lowered DFS in PTC. However, sub-analysis revealed that patients with both positive PD-L1 expression and low levels of CD8+ T-cell infiltration were associated with increased lymph node metastasis, lymphovascular invasion and reduced DFS (24). Additional research exploring the prognostic value of PD-L1 expression coupled with CD8+ density will be necessary to confirm these findings.
In a study of 407 thyroid cancer patients, Ahn et al. established no significant association between tumoral PD-L1 expression and clinicopathologic features. However, both a higher frequency and stronger staining intensity of PD-L1 protein was observed in ATCs and FTCs (25). Chintakuntlawar et al. explored the role of PD-L1 expression in a cohort of uniformly treated ATC patients. In their small cohort of 16 patients, positive staining of PD-L1 in tumor cells was shown to be predictive of poor prognosis in ATC (26). Recently published data from Bastman et al. revealed that PD-L1 expression by tumor cells and associated leukocytes was more prominent in patients with ATCs (11). These findings suggest that the antitumor immune response in ATC may be hindered by PD-1/PD-L1 interactions. Whether PD-L1 expression is a predictive marker of response to anti-PD-L1 therapy in these patients warrants further investigation.
This systematic review sheds important new light on the area, revealing that patients with local and/or distant disease recurrence tended to have higher PD-L1 expression levels than patients without recurrent disease. These findings are consistent with the study by Sun et al., wherein PD-L1-positive patients with non-small-cell lung carcinoma were seen to have a higher disease recurrence rate when compared to the PD-L1 negative group (48% vs. 27%; p < 0.001) (36). Interestingly, the study by Shi et al. reported that a lower incidence of recurrence was not observed in patients with a more advanced tumor stage who underwent total thyroidectomy. It was suggested that the elevated PD-L1 expression in patients with total thyroidectomy (66.7% vs. 48.1%) could explain why more extensive surgery did not enhance patient prognosis (29). Thus, novel agents targeting the PD-1/PD-L1 axis may prove valuable in the treatment of patients with recurrent thyroid cancers.
Notably, increased PD-L1 was expressed more frequently in patients with concurrent thyroiditis. In thyroiditis, thyroid gland parenchyma is lost and subsequently replaced by inflammatory infiltrate, which then go on to generate chemokines, cytokines, and growth factors within the tumor microenvironment. These proinflammatory cytokines, including interferon-γ, interleukin (IL)-1, IL-10, and IL-6, may trigger the upregulation of PD-L1 expression, thereby inducing thyroid tumorigenesis (27). Conversely, the negative impacts of PD-L1 expression were reduced in a subgroup of PTCs with concurrent Hashimoto's thyroiditis, suggesting that autoimmunity may remain protective, irrespective of PD-L1 upregulation in tumor tissues (29). This observation supports the notion that immune effects, and potentially immune therapy, may yield significant impact in the management of thyroid cancer. An improved understanding of the molecular mechanisms underlying concurrent autoimmunity and thyroid cancer could assist in the development of innovative therapeutic strategies and treatments.
Based on the pooled data, positive PD-L1 expression was more evident in late-stage compared to early-stage thyroid cancers. While not statistically significant, the magnitude of effect was clinically meaningful. Following initial surgery, the American Joint Committee on Cancer (AJCC)/International Union against Cancer (UICC) TNM staging system is commonly implemented to predict disease-specific mortality, and is consulted when tailoring decisions concerning postoperative adjunctive therapy (7). However, the AJCC/UICC TNM staging system has been shown to inaccurately predict the risk of persistent disease following initial therapy or clinically evident disease recurrence (37,38). As the incidence of thyroid cancer continues to escalate, clinicians will require a superior means of identifying patients with aggressive disease in order to ascertain when adjuvant treatment and long-term surveillance is appropriate. Currently, none of the staging systems designed to predict mortality from thyroid cancer incorporate molecular profiling (7). The results of this meta-analysis suggest that PD-L1 has the potential to be included alongside standard clinicopathologic prognostic markers to improve the detection of clinically relevant thyroid cancers. Additional studies comprising larger samples sizes will be necessary to validate the prognostic capabilities of PD-L1 expression in the staging of thyroid cancer.
There is currently a pressing need for biomarkers that can assist clinicians in predicting patients most likely to benefit from novel immunotherapies targeting the PD-1/PD-L1 axis. By identifying responders and non-responders prior to the commencement of treatment, patient exposure to avoidable immune-related toxicities and the financial burden of these therapies on healthcare systems would be considerably reduced. In most analyses to date, pretreatment tumor specimens with increased membranous and/or cytoplasmic PD-L1 expression by IHC have been associated with higher overall response rates to the PD-1/PD-L1 blockade, establishing its potential to serve as a predictive marker. However, it is important to note that a fraction of patients with high PD-L1 expression are unresponsive to these agents, and others with tumors confirmed as negative for PD-L1 have achieved objective clinical responses (39). The positive predictive value of this assay may therefore be insufficient for routine clinical use. Hence, it has been proposed that the most accurate predictive models for the effectiveness of PD-1/PD-L1 blockade will involve integrating PD-L1 expression with supplementary factors, including the type, location, and degree of immune infiltrate present, as well as the tumor genomic landscape and mutational load (40,41). The implementation of these biomarker signatures may be fundamental in better defining the prognosis of thyroid cancer, identifying patients at high risk of tumor recurrence, and predicting and stratifying patients who will benefit from adjuvant therapy.
In conclusion, this meta-analysis is the first to report the prognostic significance of PD-L1 expression in thyroid cancer patients. The results confirm that elevated PD-L1 status assessed via IHC is a prognostic indicator for reduced survival in patients with thyroid carcinoma. Moreover, PD-L1 overexpression was significantly associated with concurrent thyroiditis and local/distant disease recurrence. In the future, PD-L1 expression may be implemented as a prognostic biomarker used to guide clinicians in identifying patients with more aggressive cancers, and for the selection of individuals who would derive durable clinical benefit from anti-PD-1/PD-L1 immunotherapy. However, irregularities between assays, locations for PD-L1 expression assessment, and defined cutoff values for positive versus negative expression were evident within the included studies. Clarifying these inconsistencies will be necessary in order to develop applicable biomarkers to improve clinical decision making and subsequently optimize the therapeutic benefit for patients treated with novel immunotherapies. Prospective clinical trials comprising larger cohort sizes will be crucial in improving the outcomes of patients with advanced or metastatic thyroid cancer.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.