
Abstract
Background:
Women of reproductive age with differentiated thyroid cancer (DTC) often need radioactive iodine (RAI) treatment after surgery. In contrast to the well-documented effect of RAI on testicular function, the potential negative effects of this treatment on ovarian reserve have been largely dismissed. The objective of this pilot study was to examine the possibility that RAI treatment is deleterious to the ovarian reserve by prospectively measuring the concentration of anti-Müllerian hormone (AMH) after RAI treatment.
Methods:
Thirty premenopausal women (M age = 34 years; range 20–45 years) with a new diagnosis of DTC scheduled to undergo RAI ablation were recruited for this study. All of them had TNM stage 1 disease (T1–3, N0, or N1, M0), and were scheduled to receive RAI activities ranging from 30 to 150 mCi. AMH was measured at baseline and at 3, 6, 9, and 12 months after the administration of RAI.
Results:
Of the 30 women, only 24 returned after the baseline assessment. RAI treatment resulted in a significant decrease in AMH concentrations at three months, from 3.25 ± 2.75 to 1.9 ± 1.74 ng/mL (p < 0.0001). Only partial recovery was subsequently documented. Eighty-two percent of subjects had final values below baseline levels, such that at one year, serum AMH was still 32% lower than prior to treatment (2.36 ± 1.88 ng/mL; p < 0.005). The only two continuous variables that correlated with the extent of AMH reduction at three months were the woman's age (r = 0.51; p = 0.02) and the age at menarche (r = 0.48; p = 0.03). Importantly, the RAI dose was not associated with the extent of AMH reduction and neither were smoking or the use of birth control pills. Older subjects (≥35 years) were significantly more likely to experience a marked AMH reduction at three months (63.7 ± 18.5% vs. 33.1 ± 29.2%; p = 0.01). The only predictor of recovery after one year was the extent of AMH decrease at three months: the lower the decline, the higher the chances for recovery.
Conclusions:
RAI in DTC has a rapid and profound effect on ovarian reserve, with only a partial recovery potential. In an era of declining human fertility, it is of relevance to recognize the potentially adverse effect of RAI in women of reproductive age. AMH measurement may be useful as a tool in this decision-making process.
Introduction
T
Since the ovaries are exposed to ionizing radiation when RAI is excreted through the urine, the hypothesis for this study was that primary oocytes are prone to suffer an injury that can be demonstrated prospectively by an accepted index of the gamete pool reserve such as the circulating level of anti-Müllerian hormone (AMH).
Subjects and Methods
Subjects
Premenopausal women between 18 and 45 years of age with a diagnosis of DTC and scheduled to undergo postsurgical RAI ablation were invited to take part in this study. In addition to other existing malignancies and advanced renal, hepatic, or cardiac disease, exclusion criteria included TNM stage II (9), previous pelvic surgery (with the exception of Cesarean section) or surgical fertility treatments, and previous radiation exposure to the pelvis. Additionally, a small group of patients with Graves' disease were recruited to serve as a control group of women receiving low-dose RAI for a nonmalignant condition.
Study protocol
This was a prospective study scheduled to follow each patient for one year after the administration of RAI. The protocol was approved by the Tel Aviv-Sourasky Institutional Human Study Committee (approval #0660-12-TLV), and each subject gave written informed consent. Each woman underwent a baseline serum AMH measurement at least one month after thyroidectomy and typically about one month prior to RAI treatment. As AMH levels do not typically fluctuate, no particular effort was made to obtain the sample at a specific phase of the menstrual cycle. During the initial visit, each subject answered a detailed general and reproductive health questionnaire, which included questions about menstruation, pregnancies, comorbidities, smoking, and the use of oral contraceptives. Each woman was then invited to return to the endocrinology clinic at Tel Aviv-Sourasky Medical Center for repeat AMH measurements at 3, 6, 9, and 12 months after the RAI treatment.
AMH assay
Serum AMH was determined using an AMH Gen II enzyme-linked immunosorbent assay (Beckman Coulter, Brea, CA) according to the manufacturer's instructions. Women were advised not to use any biotin-containing supplements for one week prior to the assay. According to the manufacturer, the limit of detection of the assay is 0.08 ng/mL, with a probability of 95%, and the lowest quantifiable concentration is 0.17 ng/mL, with a 20% degree of imprecision. In the authors' laboratory, the assay has a coefficient of variation of 10.8%.
Statistics
Demographic and clinical characteristics of the two subject groups were tabulated and compared using the Mann–Whitney or Fisher's exact text for continuous or categorical parameters, respectively. In order to assess the behavior of AMH levels over time after RAI treatment in DTC patients, a mixed linear model was applied using an unstructured covariance matrix, adjusting for age and dose. Spearman's correlation was used in univariate analysis. To identify factors related to recovery, a logistic regression model was applied. All calculations were performed using IBM SPSS Statistics for Windows v24.0 (IBM Corp., Armonk, NY). Statistical significance was assumed for p < 0.05.
Results
Subjects' clinical characteristics and baseline AMH levels
Thirty women with newly diagnosed DTC were originally recruited for the study and provided a baseline AMH measurement. With the exception of one subject who had a mixed follicular and papillary cancer and six women with a follicular variant of papillary thyroid cancer, all other subjects had classical papillary thyroid cancer. All had TNM stage 1 disease (T1–T3, N0 or N1, M0). The indication for RAI in T1, N0 subjects was microscopic extrathyroidal extension of the tumor into the adjacent fat tissue. None had been previously exposed to RAI or any form of radiation. Apart from the baseline AMH levels presented for the entire group of recruited subjects, this report focuses on the 24 subjects who returned for later assessments of AMH after RAI treatment. In addition, data are also presented on five women who underwent RAI ablation for Graves' disease.
The age of the subjects ranged from 20 to 45 years. Demographic and salient clinical characteristics, including baseline AMH levels and the doses of RAI, are shown in Table 1. Specifically, 13/24 (54%) women in the DTC group and 3/5 (60%) in the Graves' disease group were ≥35 years old at the time of treatment (p = n.s.), seven subjects in the DTC group were ≥40 years old, as was one woman in the group of subjects with Graves' disease. Three women in the DTC group reported irregular menses, with two of them carrying a diagnosis of polycystic ovary syndrome. All patients with Graves' disease had regular menstrual periods. One woman in each group carried a diagnosis of non-classical 21-hydroxylase deficiency, but none received any specific treatment for this condition. One patient in the DTC group had normal menses under cabergoline therapy for a microprolactinoma. All women in the DTC group were euthyroid under thyroxine replacement therapy that was initiated after surgery and received RAI after recombinant human thyrotropin stimulation. Notably, baseline AMH concentrations were not different between the two groups of young women. As expected, baseline AMH levels were negatively correlated with the women's age (Fig. 1).
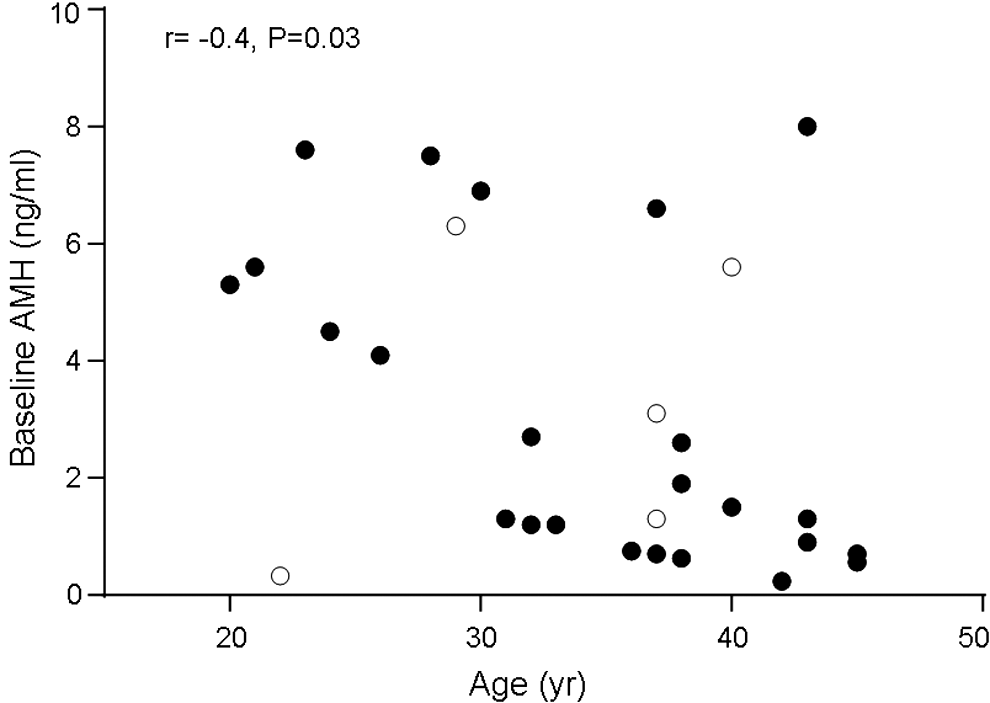
Baseline serum anti-Müllerian hormone (AMH) levels are inversely correlated with the women's age. All 35 women (30 with differentiated thyroid cancer [solid circles] and five with Graves' disease [empty circles]) are included in this analysis.
Median age was 36.5 years (range 20–45 years) for women with DTC and 37 years (range 22–40 years) in subjects with Graves' disease (p = n.s.).
Distribution of RAI doses administered to DTC subjects was as follows: six subjects received 30 mCi, two received 50 mCi, four received 100 mCi, and 12 were administered 150 mCi.
DTC, differentiated thyroid cancer; SD, standard deviation; RAI, radioiodine; AMH, anti-Müllerian hormone; n.s., not significant.
AMH response to RAI treatment
The AMH response to RAI over time for subjects with DTC is shown in Figure 2. A significant decline in AMH levels over time, and at all time points, was demonstrated using a linear mixed model that adjusted for age and RAI dose (dose was included in the model but did not affect it). A nadir was observed three months after RAI when AMH was 49% lower than baseline (1.9 ± 0.38 vs. 3.25 ± 0.56 ng/mL before treatment; p = 0.001). Thereafter, some recovery was observed for the entire group, with AMH levels plateauing at nine months, such that at one year, AMH concentrations still remained 32% below baseline (p = 0.016). The AMH values at the additional time points for the entire group were 2.23 ± 0.43, 2.47 ± 0.47, and 2.36 ± 0.47 ng/mL at 6, 9, and 12 months post treatment, respectively.
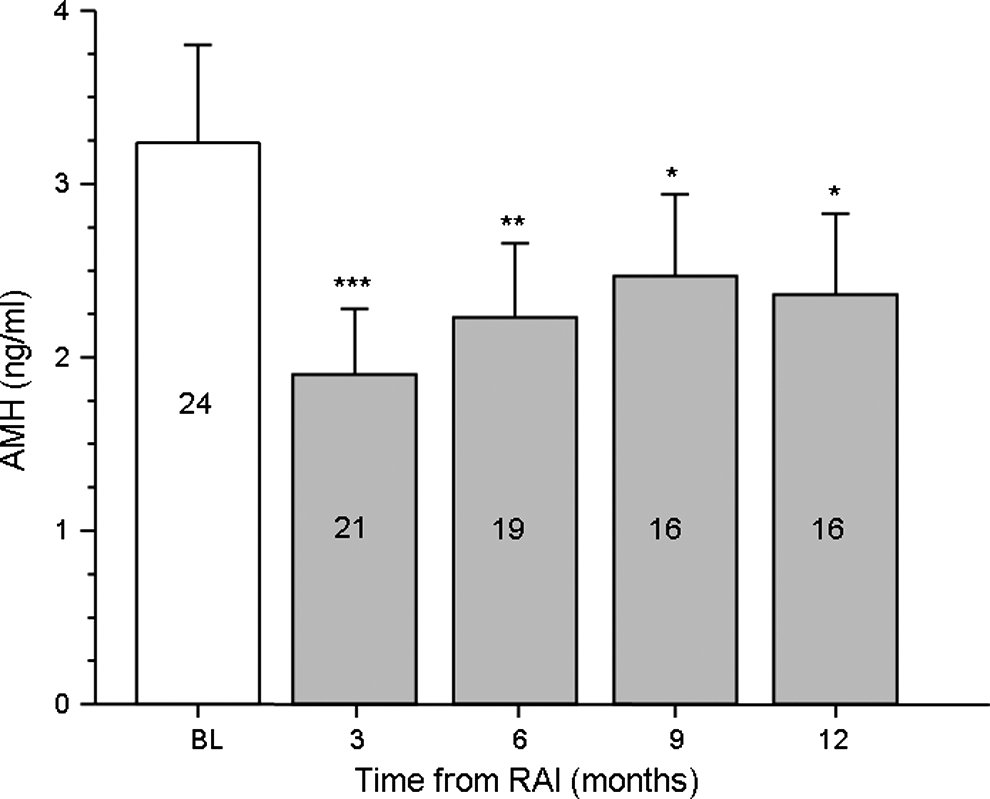
AMH levels in women with differentiated thyroid cancer in relation to the time elapsed since radioiodine ablation. The number of subjects assessed at each time point is indicated in the box. The bars show the means with standard errors. Significance for paired comparisons relative to baseline is indicated by the asterisks. ***p < 0.005; **p < 0.01; *p < 0.05.
Using univariate analysis of all the potential factors likely to affect the extent of this decrease, a positive correlation was found between the age of the subjects (r = 0.51; p = 0.02) and the age at menarche (r = 0.48; p = 0.03) Notably, there was no correlation between the decrease in AMH levels at three months and the RAI dose (Rs = −0.195; p = 0.4). When categorical parameters were considered, a diagnosis of Hashimoto's thyroiditis was strongly associated with the extent of decline in AMH at three months. The five subjects with Hashimoto's thyroiditis experienced a 72% decline compared to only 42% in the women without such a diagnosis (p = 0.015). Of note, baseline AMH concentrations were not different between DTC subjects with or without Hashimoto's thyroiditis (3.36 ± 1.7 and 3.22 ± 0.59, respectively; p = n.s.). No other categorical factor, such as smoking or the use of birth control pills, was associated with this decline.
In contrast, in women with Graves' disease who had received a much smaller dose of RAI, there was no treatment effect on AMH levels. They were 2.6 ± 2.0 ng/mL at baseline and 3.3 ± 2.35, 3.6 ± 2.14, 3.3 ± 2.52, and 3.4 ± 1.83 ng/m: at 3, 6, 9, and 12 months, respectively (p = n.s.).
To identify further factors that might predict the AMH decrease and recovery in subjects with DTC, the data were analyzed of the 16 subjects who had a full set of values for all time points. In this subgroup, the median AMH decrease at three months was 54% relative to baseline, and the levels were still 36% lower than before RAI at one year. The decrease in AMH levels at three months were stratified as a marked (≥40%) or moderate reduction (<40%). Using the median age of 35 years as a cutoff (eight subjects were <35 years of age, and eight were older), by univariate analysis, it was noted that older patients were significantly more likely to experience a marked reduction at three months than their younger counterparts (p = 0.007; a graphic representation of the AMH response in this subgroup of patients, stratified by decades, is presented in Supplementary Fig. S1; Supplementary Data are available online at
Menstrual pattern and reproductive history of women with DTC following RAI
Following RAI treatment, two women with DTC reported amenorrhea lasting up to four months (one after receiving 30 mCi and the other one after treatment with 150 mCi), while three other women reported irregular periods for at least one year following treatment. Altogether, 19.2% of women with DTC experienced menstrual irregularities after RAI treatment. All other patients reported no change in their menstrual pattern. Several of them were on oral contraception before and after treatment. To the best of the authors' knowledge, so far, only two women have conceived and delivered a healthy child, both at two years and three months after receiving RAI.
Discussion
The data presented here indicate that RAI therapy, even at the lowest administered dose of 30 mCi, induces a sharp and profound (49%) decrease in AMH, a commonly accepted index of ovarian reserve. The injury to the ovaries is most severe three months after treatment, and although there appears to be some subsequent recovery, by the end of a year after exposure, women are left with a level of AMH that is about 32% lower than baseline, above and beyond the expected age-dependent decline over this time period (10). The data also indicate that women >35 years of age are at a particularly high risk for this effect, and although no a correlation was found in any of the analyses with the dose administered, such an effect was not seen in age-matched women with Graves' disease who received doses <30 mCi, suggesting that there may be a threshold effect. Finally, in the subgroup analysis, the only determinant for a partial recovery was the extent of reduction at three months: the smaller the effect RAI on AMH levels, the greater the chances of experiencing some recovery.
A deleterious dose-dependent effect of RAI on the testicular germinal epithelium was first recognized and reported almost 35 years ago (11). This retrospective study, which documented testicular function in 12 men a year after RAI treatment, indicated a dose-related increase in FSH with a concomitant sperm count decrease. This observation was later confirmed by prospective studies of men subjected to RAI for thyroid cancer (9,12). It was further noted that although the intensity of the effect, to the point of irreversibility, was dose dependent, a notable impact was also detectable after exposure to relatively low radiation activities (<100 mCi). A concern about ovarian function in women exposed to RAI was only published later in 1989. This study retrospectively documented transient amenorrhea (up to 12 months) following RAI therapy in 27% of premenopausal women with thyroid cancer (13). The women with transient amenorrhea were older (38.9 ± 7.1 vs. 32.2 ± 6.1 years; p < 0.001), and they also displayed an increase in FSH levels. However, in contrast to men, and in keeping with the authors' own observation, this effect did not appear to be related to the dose administered. Indeed, transient amenorrhea in women treated with thyroid cancer is now a well-recognized acute effect of RAI treatment, its rate ranging between 12% and 30% of women with previously regular menses (for a review, see Sawka et al.) (8), consistent with the findings of the current study. However, based on the analysis of historical retrospective studies conducted between 1960 and 2002 (7,14 –16), a notion emerged that transient menstrual irregularities were probably inconsequential, since there was no clear evidence for decreased fertility in these women, and neither was RAI treatment associated with an increased risk of adverse obstetric outcomes (14 –16). The ovaries were even deemed to be resistant to radiation damage in comparison to the potential for irreversible damage to testicular function (17). This was further supported by a prospective study that followed FSH levels of 50 young women with DTC who had received RAI. Transient amenorrhea was reported by 20% of these subjects, a significant doubling of FSH was documented at six months. However, by one year, all patients had regular menses, and FSH levels were back to baseline values, strengthening the view that this effect had little clinical significance (18). Nonetheless, one prolonged effect of exposure of women to RAI that did gain some recognition was an earlier onset of menopause, which, from retrospective studies, was reported to occur between 1.5 and 4.4 years earlier than in control subjects (19,20). While this indirectly suggested a RAI-induced injury to the oocyte pool, no subsequent study specifically looked at this issue in depth.
This study chose to use AMH as a convenient, objective, and widely accepted index of ovarian reserve in lieu of the more cumbersome and subjective antral follicle count, with which it maintains an excellent correlation (21). AMH has not only gained considerable acceptance in estimating ovarian reserve in cancer patients subjected to chemotherapy or radiation (22), but also has shown power in predicting the age of menopause onset, particularly in older women (23). The fact AMH is also relatively insensitive to the phase of the menstrual cycle and to the use of oral contraceptives simplifies its use in this study.
A recent cross-sectional study found that AMH concentrations were 15% lower in 45 women aged 35 years who had received RAI as part of thyroid cancer treatment than in 40 age-matched control women (2.82 ± 1.88 vs. 3.35 ± 1.84 ng/mL; p = 0.038). However, the extent of the acute effect could not be appreciated in this cohort of women who were assessed anywhere between 3 and 180 months after RAI treatment. Interestingly, these authors found no correlation between AMH levels and age in both groups combined (24).
A significant finding emerging from this prospective study was the partial recovery of AMH after the nadir observed at three months post RAI in the majority of women. Still, this presumed recovery was not universal. Indeed, in some subjects the decline in AMH continued to worsen over time. The biologic basis for this recovery is still unclear. Interestingly, a similar and limited phenomenon has been reported in young women (18–39 years) undergoing chemotherapy for breast cancer who were followed for two years after treatment completion. In parallel to the present findings with RAI, age was a major factor predicting the decrease in AMH with chemotherapy. Of note in that study was also the observation that some recovery in AMH was seen in 45% of women during the two-year follow-up (25). Thus, although being a robust and accepted marker of ovarian reserve, in certain situations where the ovaries are exposed to gonadotoxic agents, AMH is not completely congruent with the pool of viable primary oocytes, as a potential for recovery appears to exist. Therefore, one should be careful not to equate AMH with the potential for fertility.
Finally, women >35 years of age were particularly susceptible to the effect of RAI on AMH. This resonates with previous findings suggesting older women receiving RAI were more likely to experience transient amenorrhea (13). Although this study was not designed to address issues such as fertility or age at menopause, it should be noted that in a recent very large retrospective cohort study from the California Cancer Registry that followed 18,850 women with DTC, RAI ablation was linked to a decreased birth rate among women between 35 and 39 years of age compared to women who had not received RAI (11.5 vs. 16.3 births per 1000 woman-years; p < 0.001). In addition, the median time to first live birth after a diagnosis of DTC was prolonged among women who received RAI compared to those who did not (34.5 vs. 26.1 months; p < 0.0001) (26).
Being a pilot project, this study has inherent limitations. First, the number of patients enrolled is limited, and some subjects were lost to follow-up. However, the extent of the effect of RAI given for DTC over AMH is far and beyond any expected age-related decline (∼0.2 ng/mL per year) in AMH concentration (10), such that causality seems very plausible. Follow-up was only 12 months, and although there appears to be a plateau, the possibility cannot be excluded that a longer follow-up period might have shown additional recovery. Because of the limited follow-up, the characterization of fertility issues was beyond the scope of this study. Finally, a small group of matched subjects were included who had received low doses of RAI for the treatment of hyperthyroidism. The lack of decrease of AMH after treatment in these subjects suggests there might be a dose threshold, which this study was clearly underpowered to detect.
The strength of the study resides mostly in its design, which showed for the first time in a prospective manner that RAI not only induces temporary menstrual abnormalities but in fact exerts a direct effect on ovarian reserve, as reflected by the level of AMH. This effect appears not to be entirely reversible.
Although the decline in AMH after RAI treatment is not necessarily synonymous with a decline in fertility (fertility is dependent on a number of factors: the oocyte pool that correlates with the patient's age and other inherited and acquired conditions), the findings call for the conduction of well-designed, larger prospective studies with longer follow-up periods to confirm and extend these observations and address potential reproductive issues. Meanwhile, in an era of declining human fertility, RAI treatment in young women with low-risk DTC should be given careful thought, particularly in those >35 years of age who still desire to have a child. Until further data are available, it is speculated that the measurement of AMH may be useful as an adjunct decision-making tool when contemplating RAI ablation in women of reproductive age.
Footnotes
Author Disclosure Statement
We certify that none of the authors has any competing financial interests.