
Abstract
Background:
Lobectomy may be sufficient for patients with intrathyroidal papillary thyroid carcinomas (PTC) <4 cm without nodal metastasis. Based on the 2015 American Thyroid Association guidelines, a strategy using ultrasound to identify appropriate candidates for lobectomy was implemented.
Methods:
Patients with Bethesda V or VI cytology who underwent surgery for PTC (January 2016 to May 2017) were retrospectively reviewed. Eligibility for lobectomy was based on both tumor (unilateral, intrathyroidal tumors ≤3 cm in size) and non-tumor (history of hypothyroidism, radiation exposure, etc.) characteristics. A detailed sonographic assessment of extrathyroidal extension (ETE) included surgeon-performed evaluation of thyroid capsular distortion, a long interface between tumor and thyroid capsule, irregular or indistinct tumor margins abutting the thyroid capsule, or a tracheal footprint.
Results:
Of 141 patients with PTC, 35 (25%) patients were candidates for lobectomy, and 105 (75%) patients were not candidates for lobectomy because of non-tumor (n = 46) or tumor (n = 59) characteristics. Of the 35 patients who were candidates for lobectomy, 27 had sonographic ETE on detailed assessment. Total thyroidectomy was performed in 23 patients, while thyroid lobectomy was performed in 12 patients. Total thyroidectomy was indicated based on final histopathology in 15 patients (ETE, aggressive histology, vascular invasion, or cervical metastasis). Histopathologic ETE was present in 13 of these 15 patients and was the only indication for total thyroidectomy in the remaining eight patients. Positive and negative predictive values for the prediction of ETE based on detailed sonographic assessment were 52% and 100%, respectively. In comparison to a strategy of routine total thyroidectomy, a detailed sonographic assessment of ETE reduced the rate of potentially avoidable total thyroidectomy from 57% to 31%.
Conclusions:
Patients with PTC who are potential candidates for lobectomy often require total thyroidectomy based on microscopic ETE detected on surgical pathology. A detailed sonographic assessment of ETE can reliably rule out microscopic ETE, reducing the rate of potentially avoidable total thyroidectomy.
Introduction
P
Retrospective analyses of previously treated thyroid cancers show that identification of appropriate candidates for lobectomy may be challenging. A significant number of patients who meet the preoperative criteria for lobectomy have high-risk features found postoperatively on surgical pathology requiring total thyroidectomy to enable administration of radioactive iodine (RAI), including aggressive histology, vascular invasion, nodal metastasis, or extrathyroidal extension (ETE) (7,8). Routine thyroid lobectomy in these patients would therefore result in high rates of inadequate lobectomy requiring completion thyroidectomy, while in contrast, routine total thyroidectomy would result in many potentially avoidable total thyroidectomies. Therefore, a strategy to identify candidates for lobectomy precisely is critical to minimize rates of completion thyroidectomy and potentially avoidable total thyroidectomy.
The purpose of this study was to assess a strategy implemented at a high-volume endocrine surgery center to identify appropriate candidates for lobectomy precisely. It was hypothesized that in preoperative candidates for lobectomy, total thyroidectomy is most commonly necessitated postoperatively due to ETE, and that a strategy centered around a detailed sonographic assessment of ETE can be used to minimize inadequate thyroid lobectomies and unnecessary total thyroidectomies.
Methods
Study protocol and participants
A retrospective study was performed of patients with Bethesda V or VI cytology who underwent surgery for PTC from January 2016 to May 2017 at a single institution by three attending surgeons (M.Y., M.L., and K.Z.). Bethesda V cytology was included in this study, as the rate of malignancy at the authors' institution for Bethesda V cytology is audited quarterly and ranges from 90% to 100%. In January 2016, the 2015 ATA guidelines for the management of differentiated thyroid cancers were incorporated into the authors' institution's clinical practice. Candidates for thyroid lobectomy included unilateral, intrathyroidal tumors ≤3 cm in the absence of cervical adenopathy. Although tumors ≤4 cm in size may be treated by lobectomy according to ATA guidelines, the institutional size threshold of 3 cm was discussed at tumor board and implemented based on interdisciplinary consensus. Surgeon-performed ultrasound (M.Y., M.L, and K.Z.) was routinely performed to assess ETE and nodal metastasis. A detailed sonographic assessment of ETE included evaluation for thyroid capsular abutment with indistinct margins, capsular distortion, a long interface between tumor and thyroid capsule, or a tracheal footprint (Fig. 1). A long interface between tumor and thyroid capsule was felt to increase the risk of ETE due to the increased opportunity for ETE to occur over a large area.

A detailed sonographic assessment of extrathyroidal extension includes evaluation of (
Patients with a family history of thyroid cancer, history of ionizing radiation, and hypothyroidism requiring thyroid hormone supplementation were routinely offered total thyroidectomy. Patients without sonographic ETE were routinely offered lobectomy, while patients with sonographic ETE were routinely offered total thyroidectomy. Based on results of surgical pathology, total thyroidectomy was considered necessary in patients with tumor size >3 cm, ETE (macroscopic or microscopic), five or more central neck metastases, one or more lateral neck metastases, aggressive histology (tall cell, diffuse sclerosing variants, etc.), vascular invasion, or contralateral carcinoma >1 cm. Tall-cell histology was defined by ≥50% cells three times as tall as they are wide.
Statistical analysis
Summary statistics were used to describe baseline characteristics. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of sonographic features in the prediction of ETE were evaluated. A flow diagram was created to describe how a detailed sonographic assessment of ETE affected surgical decision making. Statistical analysis was performed with SAS v9.4 (SAS Institute, Cary, NC).
Results
Candidates for lobectomy
A total of 141 patients with Bethesda V or VI cytology who underwent surgery for PTC from January 2016 to May 2017 were identified (Fig. 2). Of these, 46 (32.6%) patients underwent total thyroidectomy due to a family history of thyroid cancer, history of ionizing radiation, hyper- or hypothyroidism, or Hashimoto's thyroiditis. A total of 59 (42.6%) were not candidates for lobectomy because of tumor size >3 cm, the presence of bilateral nodules, or central or lateral neck lymphadenopathy detected on ultrasound. A total of 35 (24.8%) patients with unilateral, intrathyroidal tumors ≤3 cm with no evidence of cervical metastases were considered candidates for lobectomy. The mean age of these patients was 48 ± 14 years, 65% of patients were female, and the mean tumor size was 1.3 ± 0.6 cm.
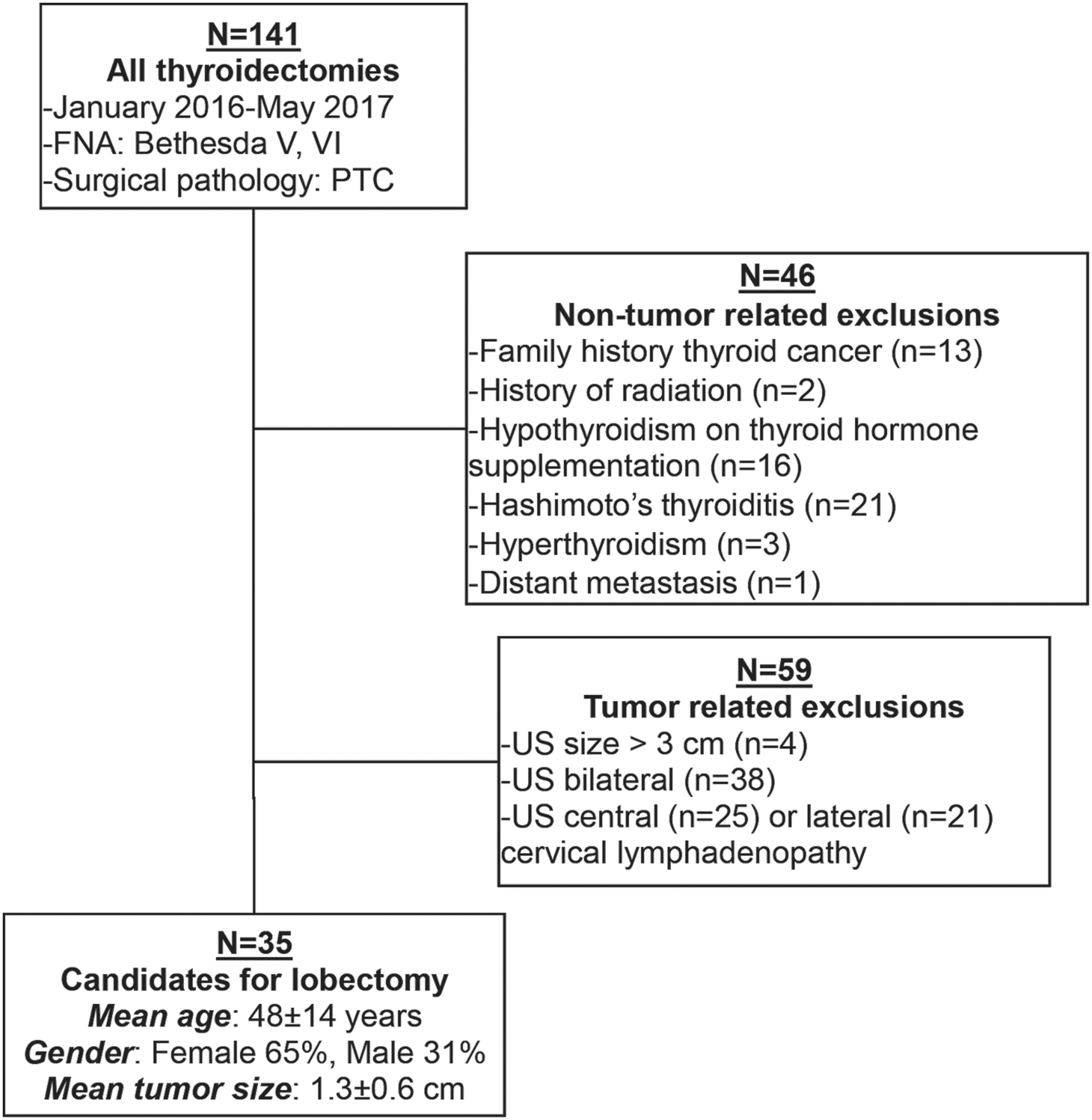
Cohort derivation.
Candidates for lobectomy requiring total thyroidectomy
Of 35 candidates for lobectomy, total thyroidectomy was necessary in 15 (42.9%) based on surgical pathology. Postoperative findings necessitating total thyroidectomy in order of descending frequency included ETE (n = 13), aggressive histology (n = 4), cervical metastasis (n = 4), and vascular invasion (n = 3). Of 13 patients with ETE, ETE was the only feature necessitating total thyroidectomy in eight patients. Macroscopic ETE was identified in 3/13 (23%) patients, and was successfully predicted by ultrasound in all three cases.
Application of a detailed sonographic assessment of ETE to surgical decision making
A flow diagram depicting the application of a detailed sonographic assessment of ETE to surgical decision making in 35 candidates for lobectomy is shown in Figure 3. Eight (22.9%) patients had no evidence of sonographic ETE, while 27 (77.1%) patients had evidence of sonographic ETE. In patients without sonographic ETE, all underwent lobectomy, and none required completion thyroidectomy. In patients with sonographic ETE, four underwent lobectomy due to patient preference, resulting in one adequate lobectomy and three inadequate lobectomies requiring completion thyroidectomy. Twenty-three patients with sonographic ETE underwent total thyroidectomy, resulting in 11 potentially avoidable total thyroidectomies and 12 necessary total thyroidectomies. In comparison to a strategy of routine total thyroidectomy, the rate of potentially avoidable total thyroidectomy decreased from 57.1% to 31.4%. In comparison to a strategy of routine lobectomy, the rate of inadequate lobectomy requiring completion thyroidectomy decreased from 42.9% to 8.6%.
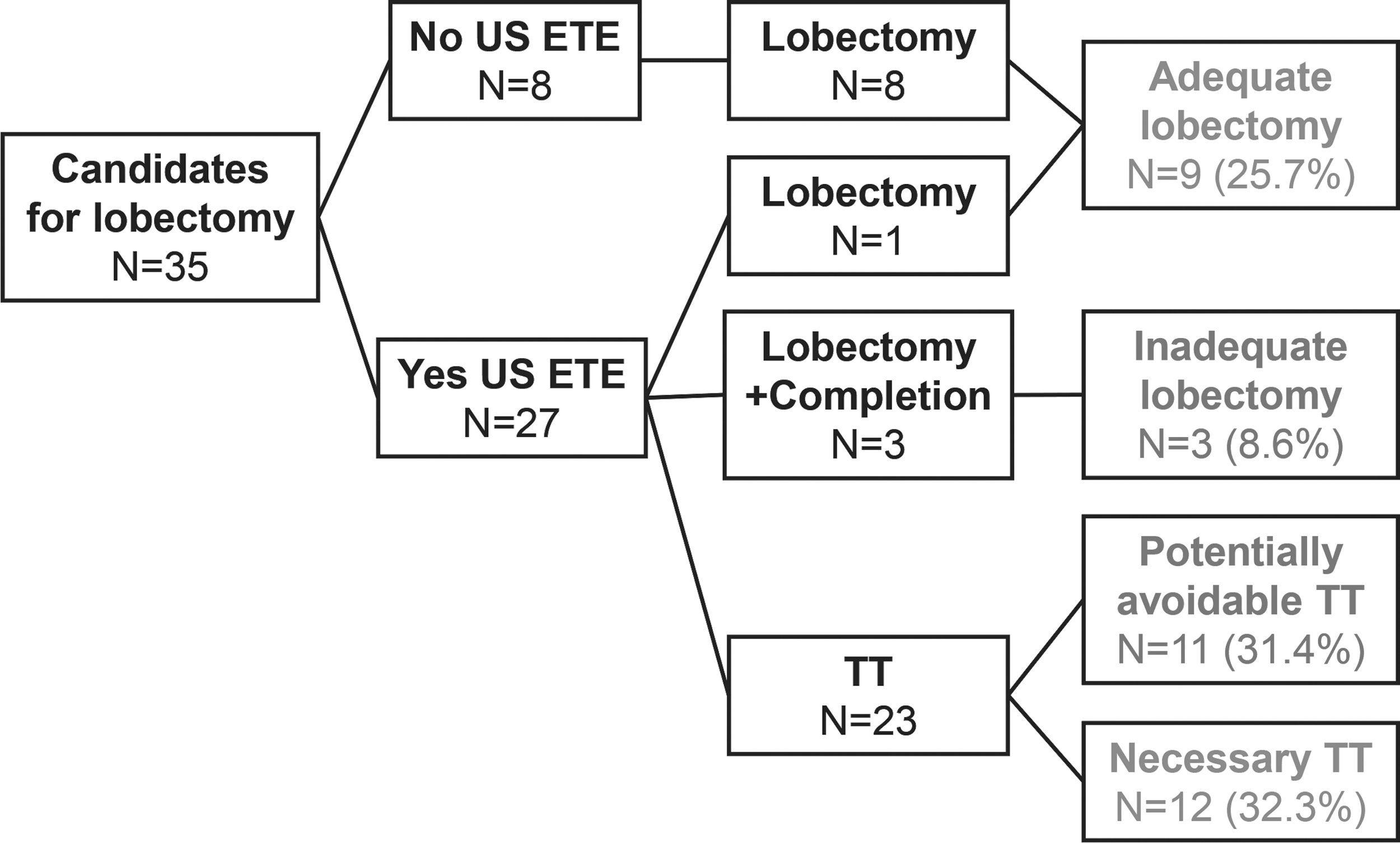
Flow diagram depicting the application of sonographic ETE to surgical decision making. US, ultrasound; ETE, extrathyroidal extension; TT, total thyroidectomy.
Performance of a detailed sonographic assessment of ETE
Of 36 candidates for lobectomy, 27 had sonographic ETE. A detailed sonographic assessment predicted ETE with a sensitivity of 100%, specificity of 36.4%, PPV of 51.9%, and a NPV of 100%.
Discussion
This study evaluated the implementation of the 2015 ATA guidelines into a high-volume endocrine surgery practice. It was found that only 35/141 (24.8%) patients with PTC were preoperative candidates for lobectomy, and 15/35 (42.9%) had postoperative findings necessitating total thyroidectomy. This was largely due to ETE (n = 13), which a detailed sonographic assessment ruled out with a negative predictive value of 100%. Applying these findings to surgical decision making, the number of potentially avoidable total thyroidectomies was minimized from 57.1% to 31.4% in comparison to a strategy of routine total thyroidectomy.
The 2015 ATA guidelines refined treatment recommendations for patients with differentiated thyroid cancer, in particular highlighting patients with low-risk disease who may not benefit from total thyroidectomy and/or RAI (2). Recommendation 35B states that lobectomy is an acceptable treatment for patients with T1–T2, N0 differentiated thyroid cancers, while recommendation 51 states that RAI is generally favored for tumors with aggressive histology, vascular invasion, microscopic ETE, five or more central neck metastases, or one or more lateral neck metastases (2). This is based on retrospective data from national cancer registries and tertiary referral centers showing no significant differences in survival between patients who receive lobectomy versus total thyroidectomy (3 –6). While the authors agree with the recommendations of the ATA guidelines, only patients with tumors up to 3 cm were offered lobectomy due to interdisciplinary consensus at their institution. However, this affected the study results only minimally, as just one patient with a tumor between 3 and 4 cm, who would have been a candidate for this study, was excluded.
Studies applying the 2015 ATA guidelines to previously treated thyroid cancers show that a significant number of patients, who would have appeared to be candidates for lobectomy preoperatively, would have required total thyroidectomy postoperatively. Kluijfhout et al. analyzed 1000 consecutive patients treated surgically for well-differentiated thyroid cancer from 2000 to 2010 (7,8). Of the 25% of patients who were potential candidates for lobectomy, total thyroidectomy would have been necessary in 43% based on aggressive histology, vascular invasion, microscopic ETE, and nodal metastasis. In a similar study, Lang et al. found that in 1513 cases of PTC, 39.7% of patients were preoperative candidates for lobectomy, while 42.8% had high-risk features requiring total thyroidectomy (9). Confirming the results of prior studies, the present study found that 35/141 (24.8%) patients with PTC were candidates for lobectomy, while 15/35 (42.9%) required total thyroidectomy based on surgical pathology postoperatively (Table 1). Also, similar to prior studies, one of the most common indications for total thyroidectomy in the present cohort was ETE, making it an ideal target for further preoperative scrutiny in selecting candidates for lobectomy (7,8,10).
Assuming a hypothetical strategy of routine thyroid lobectomy.
Assuming a hypothetical strategy of routine total thyroidectomy.
ATA, American Thyroid Association; PTC, papillary thyroid carcinoma; WDTC, well-differentiated thyroid cancer; FH, family history; ETE, extrathyroidal extension.
In contrast to prior studies involving the hypothetical application of ATA guidelines to previously treated thyroid cancers, the current study evaluated the actual implementation of a strategy incorporating ATA guidelines in a high-volume endocrine surgery practice. A number of sonographic features have been associated with ETE with varying performance, including irregular or indistinct margins, capsular abutment, subtle capsular distortion, a long interface of the thyroid capsule with the nodule, or the presence of a tracheal footprint (11 –15). In this study, sonographic ETE was defined as the presence of any one of these factors in order to maximize the sensitivity and NPV of the detailed sonographic assessment. As a result, only 8/35 (22.9%) potential candidates for lobectomy and 8/141 (5.7%) patients with PTC were offered lobectomy. This was an intentionally conservative deviation from the prior 2009 ATA guidelines recommending total thyroidectomy for tumors >1 cm (16).
Nevertheless, because ultrasound successfully ruled out ETE with a NPV of 100%, 8/35 (23%) patients were able to undergo lobectomy without completion thyroidectomy. In patients with sonographic ETE, the PPV of 52% was more modest in predicting pathologic ETE. However, knowledge of this statistic facilitates shared decision making in patients with sonographic ETE, allowing for adequate counseling regarding the risks and benefits of total thyroidectomy versus thyroid lobectomy. Moving forward, considering its modest predictive power, patients with sonographic ETE may be offered lobectomy after a thorough discussion of the risk of requiring completion thyroidectomy at the authors' institution. Furthermore, in comparison to strategies of routine lobectomy and total thyroidectomy, rates of inadequate lobectomy and potentially avoidable total thyroidectomy were minimized with this strategy.
Recently, the prognostic value of microscopic ETE as a significant risk factor in differentiated thyroid cancer has been called into question. Several retrospective studies from large tertiary centers have shown no difference in recurrence or mortality between patients without ETE and those with microscopic ETE (17,18). In the eighth edition of the American Joint Committee on Cancer staging system for differentiated thyroid cancer, only macroscopic rather than microscopic ETE can upstage a tumor to T3 (19). Although it is acknowledged that minimal ETE may not be associated with a poorer prognosis, the literature in this area continues to evolve. This study considered microscopic ETE to be an indication for total thyroidectomy, which is currently the standard of care recommended by the most recent edition of ATA guidelines.
The advantages of this study include its real rather than hypothetical implementation of the 2015 ATA guidelines into clinical practice. However, the study has limitations. The relatively recent implementation of the 2015 ATA guidelines at the authors' institution limited the sample size. Microscopic ETE may have limited prognostic significance, although this literature continues to evolve. Ultrasound is also user-dependent, and performance characteristics of a detailed sonographic assessment of ETE may vary by institution and provider. However, inter-observer variability was minimized, as ultrasound was performed by a limited group of three attending surgeons who agreed to standardized practices preoperatively. All three surgeons have similar training backgrounds and consulted one another in ambiguous cases.
In summary, the incorporation of the 2015 ATA guidelines into the authors' practice has allowed a subset of patients with low-risk PTC to undergo lobectomy safely. Although 42.9% of candidates for lobectomy ultimately required total thyroidectomy, a detailed sonographic assessment of ETE was effective in ruling out patients with ETE preoperatively. This minimized the number of potentially avoidable total thyroidectomies and inadequate thyroid lobectomies. In the setting of sonographic ETE, shared clinical decision making based on a discussion of operative risks and patient goals is recommended as the risk of pathologic ETE is approximately 50%.
Footnotes
Acknowledgments
This publication was supported in part by the H. H. Lee Research Program (E.J.K.).
Author Disclosure Statement
No competing financial interests exist.