
Abstract
Background:
Hyperthyroid patients remain at an increased risk of cardiovascular diseases (CVDs) after restoring euthyroidism. The impact of the different treatment modalities of hyperthyroidism on future CVD risk remains unclear. The aims of this study were to assess cardiovascular morbidity and mortality in hyperthyroidism before and after treatment, and to compare the effects of two different treatment modalities: radioactive iodine (RAI) and thyroid surgery.
Methods:
A comparative cohort study was conducted among 6148 hyperthyroid patients treated with either RAI or thyroidectomy and 18,432 age- and sex-matched controls. First, hospitalizations due to CVDs prior to the treatment were analyzed. Second, the hazard ratios (HR) for any new hospitalization and mortality due to CVDs after treatment were estimated among all the hyperthyroid patients compared to the age- and sex-matched controls and also in the RAI-treated patients compared to the thyroidectomy-treated patients. The results were adjusted for prevalent CVDs at the time of treatment.
Results:
Before treatment for hyperthyroidism, hospitalizations due to all CVDs were more common in the hyperthyroid patients compared to the controls (odds ratio = 1.61 [confidence interval (CI) 1.49–1.73]). During the post-treatment follow-up, hospitalizations due to CVDs remained more frequent among the patients (HR = 1.15 [CI 1.09–1.21]), but there was no difference in CVD mortality (HR = 0.93 [CI 0.84–1.03]). Compared to the patients treated with thyroidectomy, the RAI-treated patients had a higher risk of hospitalization due to all CVDs (HR = 1.17), atrial fibrillation (HR = 1.28), as well as a higher CVD mortality rate (HR = 2.56). Yet, treatment with RAI resulting in hypothyroidism was not associated with increased CVD morbidity compared to thyroidectomy.
Conclusions:
Hyperthyroidism increases the risk of CVD-related hospitalization, and the risk is sustained for up to two decades after treatment with RAI or surgery. Hyperthyroid patients treated with RAI remain at a higher CVD risk compared to patients treated with thyroidectomy. Hypothyroidism during follow-up, however, predicts better cardiovascular outcomes.
Introduction
H
Previous studies have also shown increased cardiovascular mortality after treatment with RAI for hyperthyroidism (3 –5,8) but not after thyroidectomy (1). In a recently published study comparing antithyroid medication and RAI, the mortality rates were increased during the periods of thionamide treatment for hyperthyroidism and after less intensive treatment with RAI (not resulting in hypothyroidism). However, after intensive treatment with RAI (resulting in hypothyroidism and thyroxine replacement therapy), the mortality rates did not differ between the patients and the controls (9).
Cardiovascular and cancer morbidity and mortality of patients treated with thyroidectomy and patients treated with RAI for hyperthyroidism have been reported previously (1,2,5,10). In the present work, those analyses are extended by comparing cardiovascular morbidity before and after the treatment of hyperthyroidism either with RAI or with thyroidectomy, and the impact of the treatment modalities and of the treatment outcomes (hypothyroidism or not) on cardiovascular mortality is studied after hyperthyroidism has been treated.
Methods
For this retrospective, register-based study, two groups of patients treated previously for hyperthyroidism were identified. The first group consisted of all the patients treated with thyroidectomy for hyperthyroidism in Finland in 1986–2007 (n = 4334). The patients were identified based on the procedure codes and International Classification of Diseases (ICD) codes from the nationwide Hospital Discharge Registry (HILMO) maintained by the National Institute for Health and Welfare, as previously reported (1). For thyroidectomized patients, the etiology of hyperthyroidism was obtained from the HILMO database. Follow-up data on thyroid status after the treatment were not available for the patients treated with thyroidectomy.
The second group consisted of the patients treated with RAI for hyperthyroidism during 1986–2007 at Tampere University Hospital (n = 1814). It was only possible to study the patients treated at Tampere University Hospital, where patients treated with RAI have been systematically registered since 1969. There were no register-based data available from other hospitals in Finland. Tampere University Hospital has a catchment population of 500,000 (10% of the Finnish population). The information on the etiology of hyperthyroidism, previous surgical treatment, the dates and doses of RAI treatments, and the follow-up data of thyroid function after treatment have been collected in the register since 1969. Following RAI treatment, the thyroid status of the patients has been monitored by blood samples every one to three months during the first year and subsequently every one to three years.
A control population was formed by randomly choosing three age- (±6 months) and sex-matched control subjects for each patient (treated with either RAI or thyroidectomy) from the comprehensive national Population Register Centre. The control subject had to reside in the same county as the patient and to be alive at the time the patient was treated. The total number of controls chosen was 18,432, with 12,991 controls for the patients treated with thyroidectomy and 5441 controls for the patients treated with RAI (Fig. 1).

Numbers of the patients treated with thyroidectomy or with radioactive iodine (RAI) for hyperthyroidism and the age- and sex-matched control groups.
The discharge diagnoses, as well as the dates of hospital admissions before and after the treatment, were obtained from the nationwide HILMO database, with deterministic record linkage based on the unique personal identification number assigned to all the residents of Finland. The HILMO database includes hospitalizations (hospital admission requiring an overnight stay) and causes of hospitalization of the Finnish residents since January 1969 and the procedure codes since 1986. Recording diagnoses to the HILMO database is compulsory in Finland, and its completeness and accuracy has been found to vary from satisfactory to very good (11).
Both the primary and secondary diagnoses recorded at discharge from the hospital were used in the analysis. The diagnoses have been coded according to the Finnish version of the eighth revision of the ICD (ICD-8) in 1986, the ninth revision (ICD-9) up to 1995, and the 10th revision (ICD-10) thereafter. A conversion between the different versions was made, and the cardiovascular diagnostic codes were classified into 10 major subgroups, which were analyzed separately: any CVD, hypertension, coronary artery disease, diseases of the pulmonary circulation, arrhythmias, heart failure, cerebrovascular diseases, diseases of other arteries and veins (including, for example, arteriosclerosis obliterans, aortic aneurysms and dissections, and thrombosis of both arteries and veins), and valvular diseases and cardiomyopathies. Of the arrhythmias, atrial fibrillation (AF) was also studied separately. The follow-up ended on the date of the first hospitalization due to each CVD, the date of death, emigration, or the common closing date (May 31, 2009), whichever occurred first.
The dates of death and emigration of the study subjects were obtained from the Population Registration Centre using computerized record linkage. The causes of death of the patients and the controls were obtained from Statistics Finland through record linkage. The dates and causes of death of all deceased citizens certified by a physician have been included in this register since 1971. The causes of death have been coded according to the ICD. For the mortality analysis, the underlying cause of death was used.
The study was undertaken in accordance with the Declaration of Helsinki. No informed consent could be obtained from the study subjects because of the large number of participants and because many of them died before data collection for the study. The ethics committee of the Pirkanmaa Hospital District reviewed the study protocol. The National Institute of Health and Welfare (THL) gave a permission to use the data from the Hospital Discharge Registry.
Statistical analysis
Stata for Windows v13 (StataCorp, College Station, TX) was used to calculate the hospitalization and mortality rates for various CVDs. Cox regression analyses were performed using IBM SPSS Statistics for Windows v23.0 (IBM Corp., Armonk, NY). A two-sided p-value of <0.05 was considered statistically significant. The differences in clinical characteristics between the patients treated with RAI and the thyroidectomized ones were estimated with a Mann–Whitney U-test or chi-square test, as appropriate. Kaplan–Meier curves were plotted to illustrate the hospitalization rates before and after the treatment of hyperthyroidism, and mortality after the treatment. Conditional logistic regression models were fitted to estimate the odds ratios (OR) of pretreatment hospitalization due to different CVDs (i.e., prevalent CVDs at the time of treatment). Cox regression analysis was used to estimate the hazard ratios (HR) and confidence intervals (CI) for CVD hospitalizations, and mortality after the treatment for hyperthyroidism, adjusted for prevalent CVDs.
Results
A total of 6148 patients treated for hyperthyroidism between January 1986 and December 2007 were included in the study. Of these, 4334 patients (5204 [85%] female) were treated surgically in the whole of Finland, and 1814 patients were treated with RAI at Tampere University Hospital. The median age of the patients at the time of treatment and of the corresponding controls was 49 years (interquartile range [IQR] 35–63 years). The median age was 50 years (IQR 35–64 years) in men and 49 years (IQR 35–64 years) in women. Sixteen percent (n = 988) of the patients and 15% (n = 2675) of the controls died during the follow-up, and a total of 177 subjects emigrated from Finland (Fig. 1). The median follow-up time after the treatment for hyperthyroidism was 10.6 years for the patients and 10.4 years for the controls.
The clinical characteristics of the RAI-treated and thyroidectomized patient groups are described in Table 1. The patients treated surgically were younger than the RAI-treated ones (median age at the time of the treatment 46 vs. 59 years). The sex distribution was quite similar, but the proportion of nodular disease was higher in the surgically treated patients (Table 1).
Mann–Whitney U-test.
Chi-square test.
RAI, radioactive iodine.
In Tampere University Hospital, 38 patients were treated first with RAI and then underwent surgery (2% of the RAI-treated patients), and 145 patients were treated surgically prior to RAI treatment (8% of the RAI-treated patients). No information on RAI treatment among the surgically treated patients was available from other Finnish hospitals. The patients treated first with RAI and then surgically were analyzed in the thyroidectomy group, and the patients treated first with thyroidectomy and then with RAI were analyzed in the RAI group.
CVD hospitalizations before the treatment of hyperthyroidism
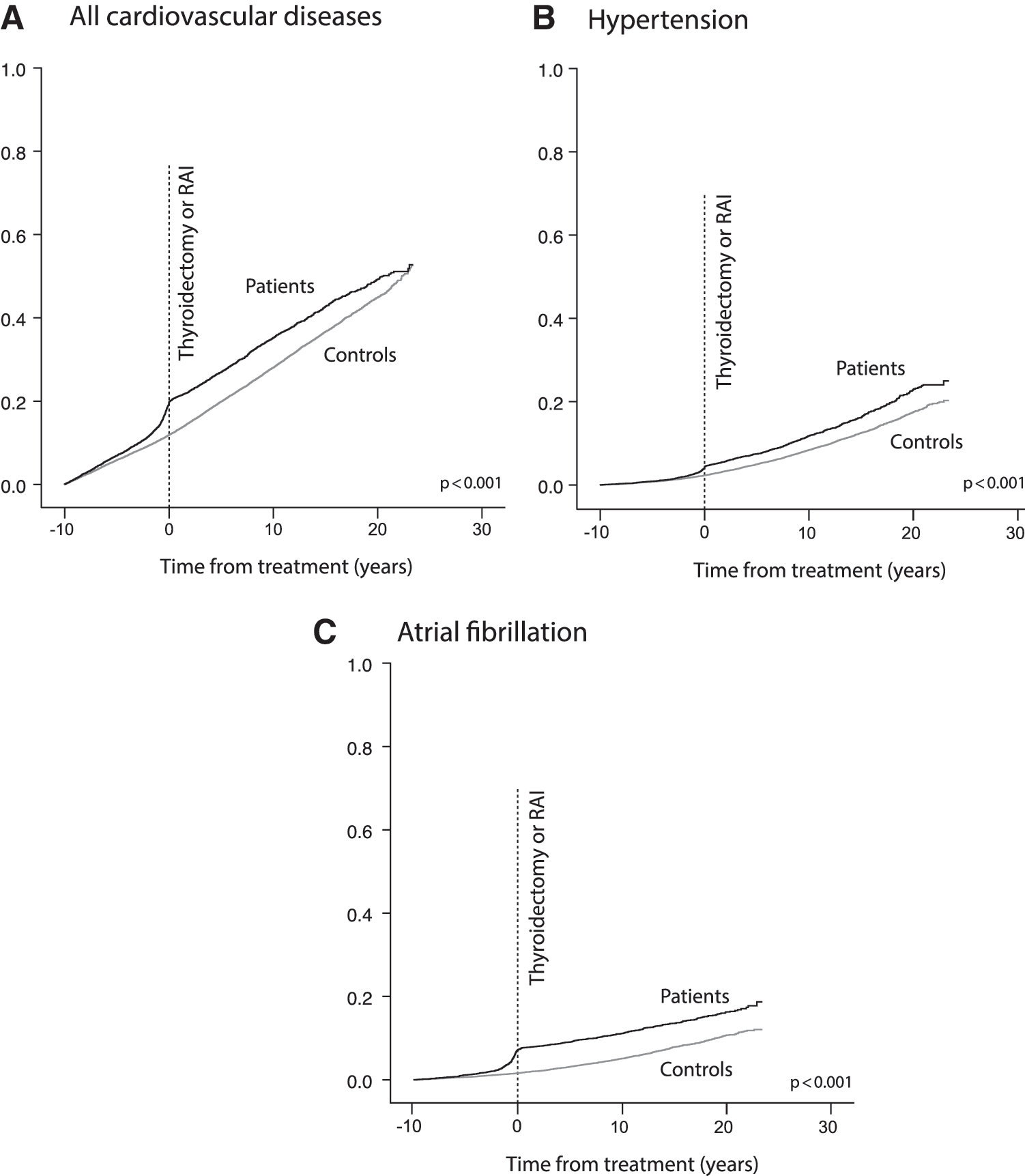
The difference in hospitalization rates between the patients (treated with either thyroidectomy or RAI) and the controls due to any CVD started to increase several years before the treatment of hyperthyroidism (Fig. 2). The risk of CVD hospitalization was increased by the time of the treatment in most of the subgroups of CVDs in the hyperthyroid patients compared to the controls (Table 2). The subgroup of CVDs most frequently associated with hospitalization before the treatment was hypertension. The hypertension-associated hospitalizations were 75% higher in the hyperthyroid patients compared to the controls at the time of the treatment. The second most frequent subgroup of CVDs consisted of arrhythmias, of which AF was the most common one. By the time of the treatment of hyperthyroidism, the OR for hospitalization due to AF was fivefold (OR = 5.13 [CI 4.39–6.00]) in the patients compared to the controls (Table 2). When the treatment groups (RAI or thyroidectomy) were separately compared to their own age- and sex -matched controls, a similar increase was seen in both treatment groups in hospitalizations due to any CVD, hypertension, or arrhythmias before the treatment of hyperthyroidism. The risk of hospitalization due to most other CVDs was also increased in the RAI-treated patients, but not in the thyroidectomized patients, compared to the respective control group (Table 2).
Nonbacterial endo-, peri and myocardial diseases, including valvular diseases and cardiomyopathy.
CVD, cardiovascular disease; OR, odds ratio; CI, confidence interval.
CVD hospitalizations after the treatment of hyperthyroidism
There were a total of 1719 hospitalizations due to any new CVD among the patients after the treatment of hyperthyroidism and 4408 hospitalizations among the controls. The risk of hospitalization due to any CVD was slightly but significantly higher among the patients compared to the controls during the follow-up when adjusted for prevalent CVDs at the time of treatment (HR = 1.15 [CI 1.09–1.21]). However, the risk clearly decreased when compared to the pretreatment risk of hospitalization due to CVDs (HR = 1.61 [CI 1.49–1.79]).
The most common subgroup of CVDs leading to hospitalization after treated hyperthyroidism among all the patients was arrhythmias (680 hospitalizations in the patients and 1275 in the controls), and the next most common was hypertension (668 hospitalizations in the patients and 1590 in the controls). The risk of hospitalization due to hypertension, arrhythmias, heart failure, cerebrovascular diseases, diseases of other arteries and veins, and valvular diseases and cardiomyopathies was slightly higher in the patients when adjusted for the prevalent hospitalizations due to the same disease prior to the treatment of hyperthyroidism. However, the risk of hospitalization for AF, coronary artery disease, or the diseases of pulmonary circulation was no longer increased after treated hyperthyroidism (Table 3).
Statistically significant values are shown in bold.
Nonbacterial endo-, peri and myocardial diseases, including valvular diseases and cardiomyopathy.
In separate analyses of the two treatment groups, the patients treated with RAI remained at an increased risk of CVD hospitalization due to any CVD, hypertension, arrhythmias, heart failure, cerebrovascular diseases, diseases of other arteries and veins, and valvular diseases and cardiomyopathies compared to their age- and sex-matched controls. The thyroidectomized patients had an increased risk of CVD hospitalization due to any CVD, hypertension, and valvular diseases and cardiomyopathies, but not due to any other subgroup of CVDs (Table 3).
Comparison of CVD hospitalizations between the RAI-treated and the thyroidectomized group
The risk of hospital admission due to CVDs after the treatment of hyperthyroidism was somewhat higher among the RAI-treated patients compared to the patients treated with thyroidectomy when adjusted for age, sex, and prevalent CVDs (HR = 1.14 [CI 1.03–1.26]; Table 4). Additional adjustment for the etiology of hyperthyroidism did not change the result (HR = 1.17 [CI 1.05–1.30]; Table 4). The risk of hospitalization due to arrhythmias (HR = 1.21 [CI 1.03–1.42]) and new-onset AF (HR = 1.29 [CI 1.08–1.54]) was also increased in the RAI-treated patients compared to the surgically treated ones, but there were no significant differences in the other CVD subgroups (Table 4).
Statistically significant values are shown in bold.
To test whether the differences in CVD hospitalizations could be due to the geographical differences between the RAI-treated and the thyroidectomized group, the same analyses were performed in the control groups. There was no difference in the risk of hospital admission due to CVDs when the controls of the RAI-treated patients were compared to the controls of the thyroidectomized patients when adjusted for age, sex, and prevalent CVDs (HR = 0.97 [CI 0.91–1.03]), excluding any significant effect of the geographical difference on the results.
Forty-seven percent (n = 855) of the RAI-treated patients started levothyroxine replacement therapy during the follow-up, indicating that RAI treatment had resulted in hypothyroidism. The rest of the patients (n = 959) either had a relapse of hyperthyroidism or became euthyroid without thyroid hormone replacement therapy. In a subgroup analysis including only the patients with RAI-induced hypothyroidism and all the surgically treated patients, there was no difference in the risk of CVD hospitalizations between the treatment groups (relative risk [RR] = 0.95 [CI 0.82–1.09]; Table 4). The result did not change in an analysis including only the patients treated with total (RR = 0.98 [CI 0.79–1.21]) or near-total (HR = 0.96 [CI 0.81–1.13]) thyroidectomy. The patients treated first with near-total and then with total thyroidectomy (n = 44 patients; 1% of all thyroidectomized patients) were not included in these analyses.
CVD mortality
Despite the increased CVD morbidity, there was no difference in the overall CVD mortality between all the hyperthyroid patients and the age- and sex-matched controls (HR = 1.06 [CI 0.96–1.18]; Fig. 3A; p = 0.284). The result remained similar when adjusted for the prevalent CVDs (HR = 0.93 [CI 0.84–1.03]) at the time of treatment, and in subgroup analyses by age and etiology (data not shown). In the analyses of different treatment groups compared to their controls, the patients treated with RAI had a higher CVD mortality rate compared to their respective controls (Fig. 3B; p = 0.004). However, CVD mortality among the patients treated with thyroidectomy (Fig. 3C; p = 0.228) and the patients treated with RAI to hypothyroidism (Fig. 3D; p = 0.053) was comparable to their control groups.

In a Cox regression analysis, cardiovascular mortality was significantly higher in the patients treated with RAI compared to the patients treated with thyroidectomy when adjusted for age, sex, and prevalent CVD (HR = 2.05 [CI 1.69–2.48]). The result was unaffected by adjustment for the etiology of hyperthyroidism (HR = 2.56 [CI 2.08–3.15]) or by including only the patients treated with near-total (HR = 2.05 [CI 1.67–2.52]) or total thyroidectomy (HR = 3.17 [CI 2.16–4.65]).
There was no difference, however, in the mortality rate between the patients treated effectively with RAI (resulting in levothyroxine-treated hypothyroidism) and those treated with total thyroidectomy (HR = 0.58 [CI 0.34–1.00]). In this analysis, there was no statistically significant difference in the subgroup of patients with nodular disease compared to the patients with Graves' disease (HR = 1.48 [CI 0.75–2.92]).
In an additional analysis including only the patients with Graves' disease treated effectively with RAI (resulting in levothyroxine-treated hypothyroidism) and the Graves' disease patients treated surgically, the risk of death due to any CVD was significantly lower in the RAI-treated patients when adjusted for age, sex, and prevalent CVDs (RR = 0.43 [CI 0.23–0.78]). However, by including only the Graves' disease patients treated with total thyroidectomy (resulting in levothyroxine-treated hypothyroidism), there was no difference in mortality rate compared to the Graves' disease patients treated with RAI (HR = 1.37 [CI 0.51–3.70]).
To test for the geographical differences between the two groups of patients, the risk of CVD mortality of the controls of the RAI-treated patients was compared to the CVD mortality of the controls of the thyroidectomized patients and adjusted for age, sex, and prevalent CVDs. There was no significant difference in this analysis (HR = 0.98 [CI 0.89–1.12]), excluding any significant effect of the geographical difference on the results.
Discussion
There are a few previous studies on long-term CVD morbidity and mortality in hyperthyroid patients treated with RAI, but only two of them included patients treated with thyroidectomy for hyperthyroidism (12,13). In the present study study, cardiovascular morbidity already increased several years before the treatment of hyperthyroidism in both groups of patients. The risk was attenuated by both treatment modalities, but the increased CVD morbidity still lasted for two decades after the treatment of hyperthyroidism. The main finding in this study is that of increased CVD morbidity and mortality in the RAI-treated patients compared to those treated with thyroidectomy. Cardiovascular morbidity or mortality did not differ between the treatment modalities if the treatment with RAI resulted in (levothyroxine-treated) hypothyroidism.
After the treatment of hyperthyroidism, the RAI-treated patients had a significantly higher risk of CVD hospitalization and mortality compared to the surgically treated patients. The patients treated with thyroidectomy were younger than those receiving RAI, but the results were adjusted for age and other clinical differences between the groups. Thyroid surgery is an effective treatment modality for hyperthyroidism, offering a predictable, high cure rate (13,14). The onset of euthyroidism is immediate after surgery, and levothyroxine therapy is started without delay if needed. After RAI treatment, thyroid function usually returns to normal within two to six months, and hypothyroidism develops within 4–12 months or even later (15). Thus, the RAI-treated patients may be either hypo- or hyperthyroid for longer time periods, allowing the stress in the cardiovascular system to last longer, compared to the thyroidectomized patients. This might explain the better prognosis of the patients treated surgically for hyperthyroidism. This explanation is supported by the better prognosis of the patients treated effectively with RAI (resulting in levothyroxine-treated hypothyroidism) compared to the patients treated surgically in this study.
Both treatment modalities are widely used, but the patients treated surgically for hyperthyroidism differ from the patients treated with RAI in several aspects. The underlying thyroid disease, patient preferences, as well as the age and the operative risks of the patient are taken into account when choosing the treatment modality. In Finland, most hyperthyroid patients have been treated with RAI over the past few decades. Thyroidectomy may have been chosen if the patient had a large goiter with compressive symptoms, a suspicion of malignancy, severe eye symptoms of Graves' disease, or hyperthyroidism resistant to antithyroid medication during pregnancy. Due to different patient selection for the different treatment modalities, the treatment groups are not totally comparable in a nonrandomized, register-based study, and there is a possibility for confounding by indication. In this study, however, the results were adjusted for the main clinical variables, including age, sex, prior CVDs, and the etiology of hyperthyroidism.
In hyperthyroidism, cardiac output increases substantially as a result of increased heart rate and contractility, together with decreased peripheral resistance and increased venous return and preload (16). Most changes in the cardiovascular system during hyperthyroidism are adaptive responses to increased energy metabolism and heat production in the body. Nevertheless, as a result of this adaptation, the cardiovascular system is strained already in resting conditions, leading to exercise intolerance, even in otherwise healthy persons (17). AF, tachycardia, elevated blood pressure, increased blood volume, and increased oxygen demands of the heart predispose to heart failure and to worsening of the symptoms of a coexisting heart disease (16,18,19). Based on this and previous studies on hyperthyroid patients (1,2,4,7,8), changes in the cardiovascular system during the hyperthyroid phase result in increased CVD morbidity and also mortality, even after restoring euthyroidism, although the mechanisms of the persistent risk remain unclear. In the present study, CVD morbidity was already increased years before the treatment. Similar results have been reported in a Danish study on hyperthyroid patients (20), which emphasizes the importance of a timely diagnosis of hyperthyroidism, especially among patients with cardiovascular symptoms, to prevent permanent impairment. Likewise, these patients should be considered at high risk for future CVDs, despite the treatment of hyperthyroidism. An active follow-up for other risk factors and for new cardiovascular symptoms of previously hyperthyroid patients are warranted.
The risk of new-onset AF remained higher in patients treated with RAI compared to patients treated with thyroidectomy. There was, however, no difference in the risk of new-onset AF between the patients treated with RAI to permanent hypothyroidism and those who underwent thyroidectomy. The risk of AF is increased in hyperthyroidism, and the prevalence also increases with age (21). After thyroidectomy, eu- or hypothyroidism is achieved faster than after RAI treatment, leading to a shorter exposure to the pro-arrhythmic effects of hyperthyroidism. A Danish study showed that the risk of AF is associated with thyroid function across the spectrum of subclinical and clinical thyroid diseases, the incidence of AF increasing with a decreasing thyrotropin (TSH) level (22). The risk of recurrent clinical or subclinical hyperthyroidism is lower after thyroidectomy than after RAI treatment, probably explaining the lower risk of new-onset AF among patients treated with thyroidectomy.
CVD mortality was similar between the hyperthyroid patients and their age- and sex-matched controls. This contradicts previous studies reporting increased CVD mortality in hyperthyroid patients (3 –5,8). The previous studies, however, were conducted mainly on patients treated with RAI. The majority of the patients in this study were treated with thyroidectomy, which may have affected the result. In a previous study on patients treated with thyroidectomy, there was no significant difference in CVD mortality between the patients and their age- and sex-matched controls (1). In the present study, CVD mortality was twice as high in RAI-treated patients compared to the patients treated with thyroidectomy, adjusted for the clinical features (age, sex, the etiology of hyperthyroidism, and prevalent CVDs prior to treatment). The excess risk was eliminated by effective treatment with RAI, resulting in hypothyroidism. The increased CVD mortality among the RAI-treated patients may thus reflect an ineffective or too slow restoration of the normal cardiovascular function after treatment with RAI in many hyperthyroid patients. Nevertheless, levothyroxine-treated hypothyroidism after treatment with RAI seemed to protect against the risk of CVD death. Similarly, decreased cardiovascular morbidity associated with the development of hypothyroidism in RAI-treated patients has been reported previously (5,7,9). This indicates that effective treatment of hyperthyroidism has a major impact on the cardiovascular prognosis of patients. In a large Danish register-based study of TSH measurements in 239,678 individuals, a 9% excess overall mortality was detected for each six-month period with low TSH levels. An excess mortality was also associated with elevated TSH measurements, highlighting the importance of euthyroidism for prognosis (23). Likewise, a recent study based on the same Danish register data reported an increased risk of mortality in both treated and untreated hyperthyroidism. There was an association between cumulative periods of low TSH and mortality. As the authors state, the excess mortality associated with hyperthyroidism may not be due to a lack of therapy, but rather to an inability to keep the patients euthyroid (24). Giesecke et al. (12) presented a similar interpretation of the effect of hyperthyroidism per se and not the treatment modality on CVD morbidity and mortality in a recently published study of 12,239 hyperthyroid patients. They found a 12% increase in CVD morbidity, but also a 27% increase in CVD mortality in hyperthyroid patients treated with either RAI or thyroidectomy compared to patients treated with thyroidectomy for nontoxic goiter.
The strengths of this study are the complete and relatively long follow-up and a large patient cohort. There are, however, some limitations to this study. The results are based on register data. Because of the nature of the study, it was not possible to adjust the results for the common risk factors of CVDs, including smoking, family history, diabetes, or medication. Smoking is a common confounding factor, and it is also a shared risk factor for CVD and hyperthyroidism, mainly Graves' disease (25,26). This may have resulted in overestimation of the risk of CVDs in the patients with hyperthyroidism compared to the age- and sex-matched controls, but is unlikely to have confounded the comparisons between the two treatment modalities because the results were adjusted for the etiology of hyperthyroidism. Information on the results of any laboratory tests after thyroidectomy or RAI was not available. Therefore, it was not possible to identify relapses of hyperthyroidism after thyroid surgery. Information on the treatment response of the levothyroxine treatment after thyroid surgery was also lacking. Both under- and overtreatment of hypothyroidism could increase the risk of CVDs. Finally, the thyroidectomy group consisted of patients treated in the whole of Finland, but the RAI group included only patients treated at Tampere University Hospital. The geographical difference is, however, unlikely to have affected the results due to broad adherence to the national guidelines on the treatment of hyperthyroidism and CVDs in Finland. In line with this view, there was no difference in the risk of CVD hospitalization or CVD mortality between the controls from the Tampere University Hospital catchment area and those from the whole of Finland. Furthermore, virtually all the patients are treated with antithyroid medication before the definitive treatment for hyperthyroidism, regardless of the treatment modality chosen.
In conclusion, hyperthyroidism increases cardiovascular morbidity compared to age- and sex-matched controls. The risk can be decreased by effective treatment of hyperthyroidism. The results underline the importance of an immediate and efficient management of hyperthyroidism and an active follow-up for cardiovascular risks after the treatment for hyperthyroidism.
Footnotes
Acknowledgments
This work was supported by grants from the Competitive Research Funding of the Pirkanmaa Hospital District and Heart Center Co., Tampere University Hospital. We thank Jorma Salmi, MD, and Rauni Saaristo, MD, for the support and enthusiasm, and Esko Väyrynen, MA, for the revision of the language of this manuscript.
Author Disclosure Statement
The authors have nothing to disclose.