
Abstract
Background:
This study sought to investigate the clinical characteristics and outcomes of propylthiouracil (PTU)-induced antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis in patients with Graves' disease.
Methods:
Sixteen patients diagnosed with PTU-induced ANCA-associated vasculitis at the authors' hospital from January 2010 to June 2017 were analyzed retrospectively.
Results:
All 16 patients with PTU-induced ANCA-associated vasculitis were female. The mean age ± standard deviation of the patients was 39.4 ± 15.3 years (range 19–69 years), and the median time of onset was 36 months (range 1–193 months) post-PTU initiation. The median dose at the onset of PTU-induced ANCA-associated vasculitis was 150 mg/day (range 50–300 mg/day). All patients had a positive serum perinuclear staining pattern (p-ANCA) and antibodies directed against myeloperoxidase (anti-MPO). Six patients tested positive for both anti-MPO antibodies and antibodies directed against proteinase-3. Seven (43.8%) patients presented with involvement of a single organ. The kidney was the organ most commonly affected, as 12 (75%) patients were found to have disease involving this organ. PTU was stopped in all patients, corticosteroids were administered to two patients, and immunosuppressive agents and corticosteroids were administered to five patients. Three patients were lost to follow-up. However, the remaining patients achieved remission after a median follow-up period of 38 months (range 6–76 months). Patients who were positive for pANCA and displayed cytoplasmic staining showed negative findings at rates of approximately 53.8% (7/13) and 100% (6/6), respectively, following treatment.
Conclusions:
PTU-induced ANCA-positive vasculitis occurs at varying times and after exposure to various doses of PTU. The condition has a milder course and has a better prognosis after PTU cessation.
Introduction
P
To gain deeper insight into the clinical characteristics and long-term outcomes of PTU-induced ANCA-associated vasculitis, 16 cases of PTU-induced ANCA-associated vasculitis that were managed at a tertiary hospital in China from January 2010 to June 2017 were retrospectively investigated.
Patients and Methods
Study patients and diagnostic criteria
Sixteen patients with PTU-induced ANCA-associated vasculitis who were diagnosed in the authors' department between January 2010 and June 2017 were retrospectively analyzed. Information was obtained regarding the following clinical parameters: age, sex, time to vasculitis onset, PTU dose at onset, tests, treatment details, and follow-up outcomes.
PTU-induced ANCA-associated vasculitis was diagnosed in the following patients (19,20): patients who presented with signs and symptoms of vasculitis after receiving PTU treatment for Graves' disease and whose disease regressed with PTU discontinuation, and patients whose indirect immunofluorescence (IIF) assay and antigen-specific enzyme-linked immunosorbent assay (ELISA) results were suggestive of ANCA positivity. Patients whose clinical symptoms and laboratory examination results were consistent with mimicking vasculitis, including infections, malignancies, and other definable types of vasculitis, were excluded from the study. The diagnosis of Graves' disease was made in patients showing hypermetabolic symptoms, along with high serum triiodothyronine levels and/or high thyroxine levels, low thyrotropin levels, and homogeneous elevated technetium uptake, according to the American Thyroid Association guidelines (21).
Laboratory parameters and treatment and outcome assessments
ANCA was detected by IIF, according to the manufacturer's instructions (Euroimmun AG, Lubeck, Germany). The staining pattern was classified as cytoplasmic (cANCA) or perinuclear (pANCA). Antibodies directed against myeloperoxidase (anti-MPO) and proteinase-3 (anti-PR3) were measured by ELISA (Euroimmun AG). The normal MPO-ANCA and PR3-ANCA concentrations are <5 IU/mL.
Patients with PTU-induced ANCA-associated vasculitis were treated with PTU therapy cessation, corticosteroids, and/or immunosuppressants, depending on their clinical symptoms and the severity of their disease (15,19). Standard radioiodine treatments for Graves' disease and outcome assessments were performed, as previously described (5,21).
This study was approved by the ethics committee of the hospital, and written informed consent was obtained from all patients before they began radioiodine treatment.
Statistical analysis
Data are presented as the median or mean ± standard deviation unless otherwise indicated. Statistical analyses were performed by matched t-tests. p-Values of <0.05 were considered statistically significant. All statistical analyses were performed with SPSS v11.0 for Windows (SPSS, Inc., Chicago, IL).
Results
General clinical characteristics
The clinical data for the 16 patients diagnosed with PTU-induced ANCA-associated vasculitis are presented in Table 1. All 16 patients were women diagnosed with Graves' disease, and the average age of the patients was 39.4 ± 15.3 years (range 19–69 years). The median dose at PTU-induced ANCA-associated vasculitis onset was 150 mg/day (range 50–300 mg/day), and the duration of PTU treatment ranged from 1 to 193 months (median 36 months). Twelve (75%) patients had been taking PTU for more than a year before developing clinical vasculitis, while the other four (patients 2, 8, 11, and 16) presented with vasculitis after taking PTU for four, three, one, and one months, respectively. All the patients developed vasculitis during PTU treatment.
Presented with hemoptysis and radiographic infiltrates, as demonstrated by computed tomography, but showed no evidence of infection.
Presented with elevated serum creatinine concentration.
Determined by renal biopsy.
PTU, propylthiouracil; ANCA, antineutrophil cytoplasmic antibody; pANCA, perinuclear staining pattern of ANCA; cANCA, cytoplasmic staining pattern of ANCA; MPO, myeloperoxidase; PR3, proteinase 3; Hu, hematuria; Pr, proteinuria; F, fever; M, malaise; WL, weight loss; RP, rash or purpura; Ar, arthralgia; My, myalgia; He, hemoptysis; Ul, ulcer.
Most of the patients presented with systemic disease. Of the 16 patients with PTU-induced ANCA-associated vasculitis, nine (56.3%) presented with systemic symptoms such as malaise, eight (50.0%) presented with fever, seven (43.8%) presented with myalgias, and five (31.3%) presented with arthralgias. The clinical presentations of the patients with PTU-induced ANCA-associated vasculitis are shown in Table 2. The kidneys (36.4%), joints (15.5%), and muscles (21.2%) were the organs most frequently affected by vasculitis. Of the 16 patients enrolled in the study, seven (43.8%) had disease involving a single organ, three (18.8%) had disease involving two organs, four (25.0%) had disease involving three organs, and two (12.5%) had disease involving four organs. Disease involving the kidney, which occurred in 12 (75%) patients, was the most common presentation of ANCA-associated vasculitis. Hematuria and proteinuria were present in these patients. However, only two patients (patients 7 and 9) presented with elevated serum creatinine levels. Renal biopsy was performed in four patients (patients 7, 8, 10, and 15). The clinical signs of vasculitis involving the joints, muscle, and skin included migratory arthritis, myalgia, purpura, and rash. Lung manifestations of vasculitis were observed in three patients (patients 5, 9, and 15), all of whom presented with hemoptysis, cough with sputum production, wheezing, or radiographic infiltration, as demonstrated by computed tomography. However, none of the patients displayed evidence of infection (Fig. 1). Mouth ulcers were observed in one patient (patient 12) with skin rash, arthralgias, and myalgias.
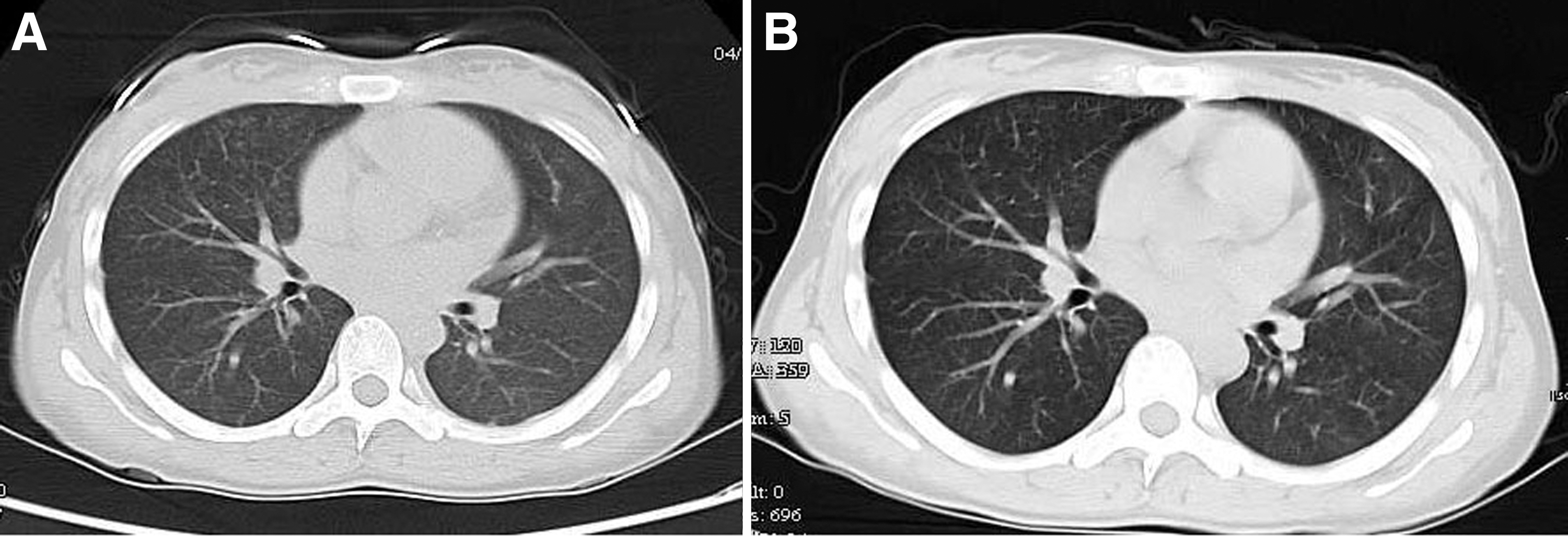
Patient 15, a 19-year-old female with a 36-month history of Graves' disease, for which she was taking 150 mg/day of propylthiouracil (PTU), was admitted for three days' history of malaise, hematuria, and proteinuria and one week's history of hemoptysis. Chest computed tomography revealed diffuse bilateral opacifications consistent with pulmonary hemorrhage (
Treatment and prognosis (Table 3)
PTU was discontinued in all the patients immediately after the diagnosis was established. Nine patients with only constitutional symptoms, including hematuria, proteinuria, arthralgia, myalgia, purpura, and rash, presented with vasculitis after PTU cessation. Corticosteroids were added in two patients (patients 5 and 12). Immunosuppressive agents (cyclophosphamide, azathioprine, Triptergium wilfordii polyglycoside, and mycophenolate mofetil) and corticosteroids were administered to five patients (patients 7, 9, 10, 15, and 16) who presented with either active systemic disease or impaired renal function. Of these patients, one (patient 7) received rituximab, and one (patient 9) received plasmapheresis. The median time to vasculitis resolution after PTU cessation was two weeks (range 1–10 days).
DC, discontinuation of PTU; CS, corticosteroids; C, cyclophosphamide; AZA, azathioprine; TW, Triptergium wilfordii polyglycoside; MMF, mycophenolate mofetil; R, rituximab; PE, plasma exchange; Hypo, hypothyroidism; Sub hyper, subclinical hyperthyroidism; NA, not available.
Two patients (patients 15 and 16) were euthyroid after PTU cessation. The remaining 14 patients were administered radioiodine. Three patients were lost to follow-up. The remaining patients were followed for a period ranging from 6 to 76 months (median 38 months). All the patients achieved remission with respect to their vasculitis, and no patients experienced a relapse of their vasculitis symptoms. Seven patients developed hypothyroidism, two patients became euthyroid, and two patients developed subclinical hyperthyroidism during the follow-up period.
ANCA serology at diagnosis and ANCA detection during follow-up
All 16 patients were pANCA and anti-MPO positive. The anti-MPO titer was 7.8–812 IU/mL (median 72 IU/mL). Seven patients were positive for cANCA, and six patients were positive for both anti-MPO and anti-PR3. The anti-PR3 titer was 1.3–158 IU/mL (median 3.3 IU/mL). Three patients were lost to follow-up. ANCA serologies were available for 13 patients during a median follow-up period of 38 months. At the last follow-up visit, approximately 53.8% (7/13) and 100% (6/6) of patients who were pANCA- and cANCA-positive, respectively, showed negative results. The anti-MPO titer (range 0.8–99.1 IU/mL, median 5.9 IU/mL) decreased in all patients and was within the reference range in six patients. Four patients (patients 2, 6, 11, and 12) who were positive for both anti-MPO and anti-PR3 at diagnosis were positive for anti-MPO at the last follow-up visit. The anti-MPO concentration at the last follow-up visit was significantly different from that at diagnosis (65.8 vs. 26.1; p = 0.01). The anti-PR3 titer decreased to a level that was within the reference range in four patients. The anti-PR3 concentration at the last follow-up visit was not significantly different from that at diagnosis (22.1 vs. 2.7; p = 0.11).
Discussion
The clinical features of PTU-induced ANCA-associated vasculitis have been investigated in a limited number of studies, which reported on different aspects of the disease. The present study retrospectively analyzed 16 patients who were diagnosed with PTU-induced ANCA-associated vasculitis in the authors' department over a period of seven years, and it uncovered several important findings.
First, all 16 patients were diagnosed with Graves' disease. The study did not include any patients with multinodular toxic goiters or toxic adenomas, suggesting that PTU-induced ANCA-associated vasculitis might be restricted to cases with autoimmune hyperthyroidism. A previous study revealed that the prevalence of ANCA was high in patients with Graves' disease but not in patients with toxic multinodular goiters (22). The absence of patients with toxic multinodular goiters and toxic adenomas in this study may reflect the relative rarity of PTU-induced ANCA-associated vasculitis and the epidemiology of thyrotoxicosis causes in an iodine-sufficient area. All the patients diagnosed with PTU-induced ANCA-associated vasculitis who were included in the study were female, and they were predominantly of middle age (average 39.4 years). Similar results have been noted by other studies (19,23 –26), and such predominance may be attributable to the tendency of Graves' disease to affect younger people and women (2). PTU-induced ANCA-positive vasculitis can appear at any time after the initiation of PTU therapy. However, in the present study, the majority of patients (75%) developed vasculitis beyond one year after drug initiation. The risk of developing vasculitis after a longer PTU treatment duration has been reported in previous studies (6,10–11,26). However, four patients in this study developed vasculitis within the first three months after PTU treatment initiation, a phenomenon that has also been reported previously (10,27 –29). The PTU dose at ANCA-associated vasculitis onset was 150 mg/day and ranged from 50 to 300 mg/day. Similar results (median 200 mg/day; range 50–450 mg/day) were obtained in a study by Noh et al. (6). Thus, physicians should have a good understanding of PTU-induced ANCA-associated vasculitis. Specifically, they should understand that the time of onset of the disease and the PTU dose at disease onset vary widely.
Second, ANCA is the serological hallmark of ANCA-associated vasculitis. However, the pathogenesis of PTU-induced ANCA-associated vasculitis is not well elucidated, as the condition is multifactorial and influenced by both genetic susceptibility and environmental factors such as infections. Interactions between PTU and ANCA target antigens, particularly MPO, which shares approximately 44–46% of its nucleotide and amino acid sequences with thyroid peroxidase, have been suggested to contribute to the development of vasculitis (30). Another possible cause of the disease is the MPO-mediated conversion of PTU to PTU sulfonate, which has immunogenic effects on T cells. T cells then activate B cells, leading to p-ANCA production and vascular injury (31,32). Evidence showing that p-ANCA directly induces vasculitis in vivo was reported by one study (33). All the patients in the present study were p-ANCA- and anti-MPO-positive, perhaps because of the pathogenesis of PTU-induced ANCA-associated vasculitis. The study shows that most patients had a lower anti-MPO concentration at the last follow-up visit than at diagnosis. After PTU cessation and/or immunosuppressive treatment initiation, anti-MPO levels remained elevated in some patients but were not associated with vasculitis. Similar results were found in previous studies (34,35). Another study showed that the anti-MPO titer decreased in 98% of patients and became negative in 18% of patients investigated longitudinally, which suggests that no association exists between serum anti-MPO levels and vasculitis severity in ANCA-associated vasculitis following PTU treatment (6). Differences in study results may be related to differences in investigation methods, diagnostic criteria, sample sizes, and the ethnicities of the included patients.
Third, as PTU-induced ANCA-positive vasculitis can affect all organs, the clinical manifestations of the disease are extremely heterogeneous. The kidney (75%) was the organ most frequently affected by the disease in the present study, a finding consistent with those of previous studies, which reported that >50% of their patients had kidney disease on presentation (19,23,25,26,36). Hematuria and proteinuria are common manifestations of PTU-induced ANCA-positive vasculitis. Elevated serum creatinine levels were noted in two patients, and patient 9 underwent plasmapheresis. The data show that joints, muscles, and the skin were other organs commonly affected by the disease. Certain organs, such as the digestive tract, the heart, and the central nervous system, were not found to be affected by the disease in the present study, results similar to those found in previous studies (14,19,23). Patients should be told to notify their physician promptly if they develop malaise, fever, myalgia, arthralgias, skin rash, hematuria, proteinuria, or hemoptysis. When symptoms suggestive of PTU-induced ANCA-associated vasculitis are present, physicians should immediately discontinue PTU and measure ANCA levels, including complete blood count, renal function, liver function, c-reactive protein, and erythrocyte sedimentation rate, which aid in establishing the diagnosis and evaluation of disease severity and activity. Early recognition and treatment of PTU-induced ANCA-positive vasculitis are very important. With immediate discontinuation of PTU, patients should experience improvement in the majority of their clinical symptoms. Decisions regarding corticosteroid and/or immunosuppressant administration should be made based on disease severity and organ involvement.
The present data show that nine (56.3%) patients achieved remission after PTU cessation and that all patients achieved remission during follow-up. No patients progressed to end-stage renal dysfunction or died, results inconsistent with those of previous studies (6 –8,19,24 –26). This difference may be attributable to the fact that the present study population included only patients with PTU-induced ANCA-positive vasculitis who were referred for radioiodine treatment. Other patients may have achieved a euthyroid status or may have died before being referred. Additionally, some previous cases may have gone unrecognized.
In conclusion, PTU-induced ANCA-positive vasculitis occurs at varying times and following various doses of PTU. This condition follows a milder course and has a good prognosis following PTU discontinuation, and experience suggests that early disease recognition and immediate PTU cessation are important for its treatment.
Footnotes
Acknowledgments
This study was supported by the Science and Technology Planning Project of Zhejiang Province (2017KY061, 2016KYB099) and the Natural Science Foundation of Zhejiang Province, China (LY15180007). We would like to thank Drs. Yi-li Yang and Hong-ye Fu for their contributions to the initial study involving this cohort.
Author Disclosure Statement
No competing financial interests exist.