
Abstract
Background:
Regional lymph node metastases (LNM) have prognostic significance in differentiated thyroid cancer (DTC). However, there was no distinction between N1a and N1b in the final staging classification in the eighth edition of the tumor-node-metastasis (TNM) staging system. This study aimed to evaluate the prognostic implication of N1b classification for predicting disease-specific survival (DSS) in DTC patients with stage I/II disease.
Methods:
A total of 3089 patients with stage I/II DTC who underwent thyroid surgery between 1996 and 2005 were included. DSS was evaluated according to N classification and number of LNM. A modification of the TNM was assessed that classified N1b cases in patients aged ≥55 years as stage IIB and the remaining cases as stage IIA.
Results:
The mean patient age was 45.6 years, and the median follow-up period was 10.0 years. In patients aged ≥55 years, patients with N1b had significantly poorer DSS compared to those with N0 (hazard ratio [HR] = 11.0; p < 0.001) and N1a (HR = 4.2; p = 0.013). The large-volume LNM group had significantly poorer DSS compared to the N0 (HR = 10.1; p < 0.001) and small-volume LNM (HR = 3.9; p = 0.019) groups. When patients were reclassified using the modified TNM staging system, DSS was significantly poorer in stage IIB patients than in stage IIA patients (HR = 2.9; p = 0.030).
Conclusions:
N1b classification has a significant prognostic implication in patients with stage I/II DTC, especially in older patients. Modified TNM staging employing N1b classification could be more useful for the prediction of DSS.
Introduction
R
AJCC/UICC, American Joint Committee on Cancer and International Union Against Cancer; TNM, tumor-node-metastasis.
Recently, the eighth edition of the TNM staging system (TNM-8) was published came into effect from January 2018. In the TNM-8, the distinction between central (N1a) and lateral neck (N1b) LNM was not adopted for the final staging classification (Table 1) (9). TNM staging has been widely accepted in patients with DTC, based on its usefulness in predicting disease mortality after surgery and providing guidance for treatment planning (12). Patients with higher-stage disease should receive more aggressive treatment than those with lower-stage disease. DTC patients with lateral LNM require more extensive surgical treatment, whereas those without lateral LNM need a more limited extent of thyroid surgery. However, the recently updated TNM staging system classified a significant number of patients with and without N1b disease in the same stage. Therefore, there are concerns about under-staging in patients with N1b disease, which may affect recurrence and disease mortality.
This study aimed to evaluate the disease-specific survival (DSS) according to the status of LNM in patients with stage I and II DTC. According to the age classification of the TNM-8, DSS was also evaluated by dividing patients based on age (55 years). The modification of TNM-8 staging is also suggested, considering lateral LNM in older patients.
Materials and Methods
Patients
A total of 3189 consecutive patients with DTC who underwent initial thyroid surgery at the Asan Medical Center (Seoul, Korea) from January 1996 to December 2005 were screened. Within this cohort, 100 patients were excluded who were <18 years old (n = 27) or who were classified as stage III or stage IV according to TNM-8 (n = 73). Finally, 3089 patients were eligible for this analysis. All patients had pathologically proven papillary thyroid carcinoma (PTC) or follicular thyroid carcinoma (FTC), including Hürthle cell carcinoma. The study protocol was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Korea.
Definitions
Patients were classified into three groups based on the N classification of the TNM-8: N0 (no LNM), N1a (metastasis to level VI or VII LNs), and N1b (metastasis to level I, II, III, IV, and V, or retropharyngeal LNs) (9). Patients with N1 were further divided into two groups according to the number of metastatic LNs: small-volume LNM (≤5 metastatic LNs) and large-volume LNM (>5 metastatic LNs) (12).
For better prediction of survival in the TNM staging system, stage II was subdivided using a modified TNM staging system. N1b cases in patients aged ≥55 years were re-staged as stage IIB, while the remaining cases were staged as IIA.
DSS was defined as the time from the date of surgery until last censoring or death from DTC. Overall survival (OS) was defined as the time from the date of surgery until last censoring or any cause of death.
Surgical treatment and radioactive iodine ablation
From 1996 to 2005, the physicians and surgeons who participated in the management of thyroid cancer patients remained almost identical and shared protocols to maintain uniform treatment and follow-up. As previously reported, prophylactic central compartment node dissection (CCND) was routinely performed, while therapeutic central and lateral neck dissection was performed in patients with clinically apparent lateral cervical LN metastasis (13,14). Preoperative metastatic LN status was evaluated with either high-resolution neck ultrasonography or enhanced neck computed tomography. CCND usually involved level VI LNs. LN dissection of level VII was undertaken only in patients with suspected metastasis in that area. Lateral neck LN dissection included levels II, III, and IV. LN dissection of levels I and V were performed only for suspected metastatic LNs (13). Radioactive iodine (RAI) remnant ablation was performed if indicated at two to three months after the initial surgery according to the protocol established by the Department of Endocrinology and Metabolism of Asan Medical Center (15).
Follow-up protocols
The follow-up protocol after initial treatment for DTC was as previously reported (16 –18). Briefly, patients took levothyroxine for thyrotropin suppression and were regularly followed up with physical examinations, as well as the measurement of thyroid function, serum thyroglobulin (Tg), serum anti-Tg antibody, and neck ultrasound every 6–12 months. Diagnostic whole-body scans with measurement of the serum-stimulated Tg level were also performed 12–24 months after the initial therapy in patients who underwent total thyroidectomy and RAI remnant ablation. Additional diagnostic imaging studies, such as computed tomography, magnetic resonance imaging, or 18-fluorodeoxyglucose positron emission tomography were also performed as needed (17).
Statistics
Statistical analyses were performed using R v3.10 (R Foundation for Statistical Computing, Vienna, Austria;
The proportion of variation explained (PVE) in the Cox proportional hazard model was calculated for the relative predictability of each TNM staging system, as previously described (19). PVE was determined using the mathematical formula PVE = 1 – exp(–G2/n), where G2 is the maximum likelihood ratio that is determined by analysis using the chi-square test associated with the null hypothesis, and n is the total number of valid cases in the study. Harrell's c-index was also calculated to evaluate the predictive capacity of each TNM staging system (20). A model with perfect predictive capacity (sensitivity and specificity of 100%) would have a Harrell's c-index of 1.00. A TNM staging model that exhibited a higher PVE or Harrell's c-index was considered to exhibit a more accurate predictive capacity.
Results
Baseline characteristics of DTC patients with TNM stage I and II disease
The clinicopathologic characteristics of the 3089 DTC patients with TNM stage I and II are summarized in Table 2. The mean patient age was 45.6 ± 11.6 years, and 2709 (88%) patients were female. The majority of patients had PTC (2979 patients; 96%), and only 4% (110 patients) had FTC. The mean primary tumor size was 1.7 ± 1.3 cm. Microscopic extrathyroidal extension (ETE) and gross ETE were found in 1042 (34%) and 412 (13%) patients, respectively. Cervical LNM were present in 1526 (49%) patients; 1563 (51%), 1240 (40%), and 286 (9%) patients were classified as N0, N1a, and N1b according to the N classification of TNM-8, respectively. When patients with N1 classification were stratified by number of metastatic LNs, 1057 (34%) and 469 (15%) patients were classified with small- and large-volume LNM, respectively. Thirty-three (1%) patients had distant metastases of DTC at initial treatment. A total of 2456 (80%) patients underwent total thyroidectomy, and 2353 (76%) patients received RAI therapy. According to TNM-8, 2709 (88%) and 380 (12%) patients were classified as stage I and stage II, respectively. The median follow-up period until censoring or death was 10.0 years (IQR 8.1–11.9 years).
Date presented as n (%), unless indicated otherwise. Small-volume and large-volume LNM is divided by number of metastatic LNs of five.
Nodal stages were classified according to the eighth edition of the AJCC TNM staging system.
DTC, differentiated thyroid cancer; PTC, papillary thyroid cancer; FTC, follicular thyroid cancer; LN, lymph node; LNM, lymph node metastasis; RAI, radioactive iodine; AJCC, American Joint Committee on Cancer; SD, standard deviation; TNM, tumor-node-metastasis.
Survival analysis according to N classification
DSS according to the N classification in stage I/II DTC patients is shown in Table 3 (upper panel) and Figure 1. In patients aged <55 years, 1185 (49%), 1001 (41%), and 238 (10%) patients were classified as N0, N1a, and N1b, respectively. The 10-year DSS rates of patients with N0, N1a, and N1b classifications were 99.6%, 99.8%, and 99.1%, respectively. There was a significant difference in DSS according to N stage (p = 0.003; Fig. 1A). Patients with N1b had significantly poorer DSS compared to those with N0 (HR = 6.2 [CI 1.4–27.6]; p = 0.018) and N1a (HR = 8.2 [CI 1.5–44.7]; p = 0.015).
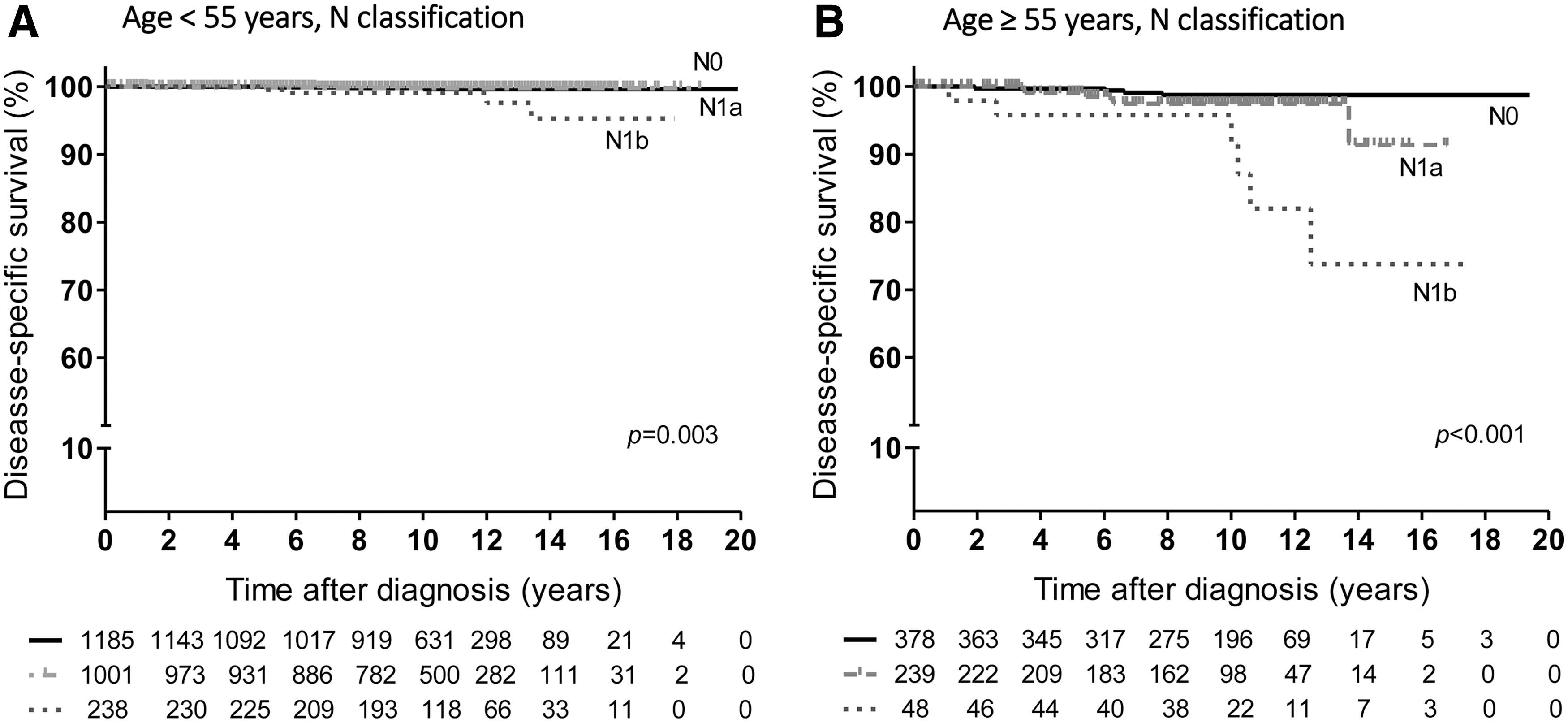
Disease-specific survival (DSS) of patients with stage I/II differentiated thyroid carcinoma (DTC) according to the N classification of the tumor-node-metastasis (TNM) staging system after stratifying by age. (
Patients were classified into three groups based on the N classification of the eighth edition of the AJCC TNM staging system: N0 (no LNM), N1a (metastasis to level VI or VII LNs), and N1b (metastasis to level I, II, III, IV, or V, or retropharyngeal LNs). The patients were also divided into three groups according to the number of metastatic LNs: N0 (no LNM), small-volume LNM (≤5 metastatic LNs), and large-volume LNM (>5 metastatic LNs). Statistically significant values are shown in bold.
N, node; DSS, disease-specific survival; HR, hazard ratio; CI, confidence interval.
In patients aged ≥55 years, 378 (57%), 239 (36%), and 48 (7%) patients were categorized as N0, N1a, and N1b, respectively. The 10-year DSS rates in patients with N0, N1a, and N1b classification were 98.7%, 97.4%, and 91.4%, respectively. DSS was significantly different between the three groups (p < 0.001; Fig. 1B). Patients with N1b had significantly poorer DSS compared to those with N0 (HR = 11.0 [CI 3.1–39.4]; p < 0.001). When the DSS between the N1a and N1b groups was compared, the N1b group also had significantly poorer DSS compared to the N1a group (HR = 4.2 [CI 1.3–13.2]; p = 0.013).
The 10-year OS rates in patients with N0, N1a, and N1b classification in older patients (≥55 years) were 95.8%, 93.4%, and 86.7%, respectively (Supplementary Table S2 and Supplementary Fig. S1). OS was significantly different between the three groups (p < 0.001; Supplementary Fig. 1B), and patients with N1b had significantly poorer OS compared to those with N0 (HR = 4.6 [CI 2.1–9.9]; p < 0.001).
Survival analysis according to the number of metastatic LNs
DSS according to the number of metastatic LNs in stage I/II DTC patients is shown in Table 3 (lower panel) and Figure 2. When examining only younger patients (<55 years), 1185 (49%), 830 (34%), and 409 (17%) patients were classified as N0, small-volume LNM, and large-volume LNM, respectively. The 10-year DSS rates for patients with N0, small-volume LNM, and large-volume LNM were 99.6%, 99.7%, and 99.4%, respectively. There was no significant difference in DSS between the three groups (p = 0.125; Fig. 2A). Small- and large-volume LNM were not associated with poorer DSS compared to N0 (p = 0.93 and p = 0.10, respectively).
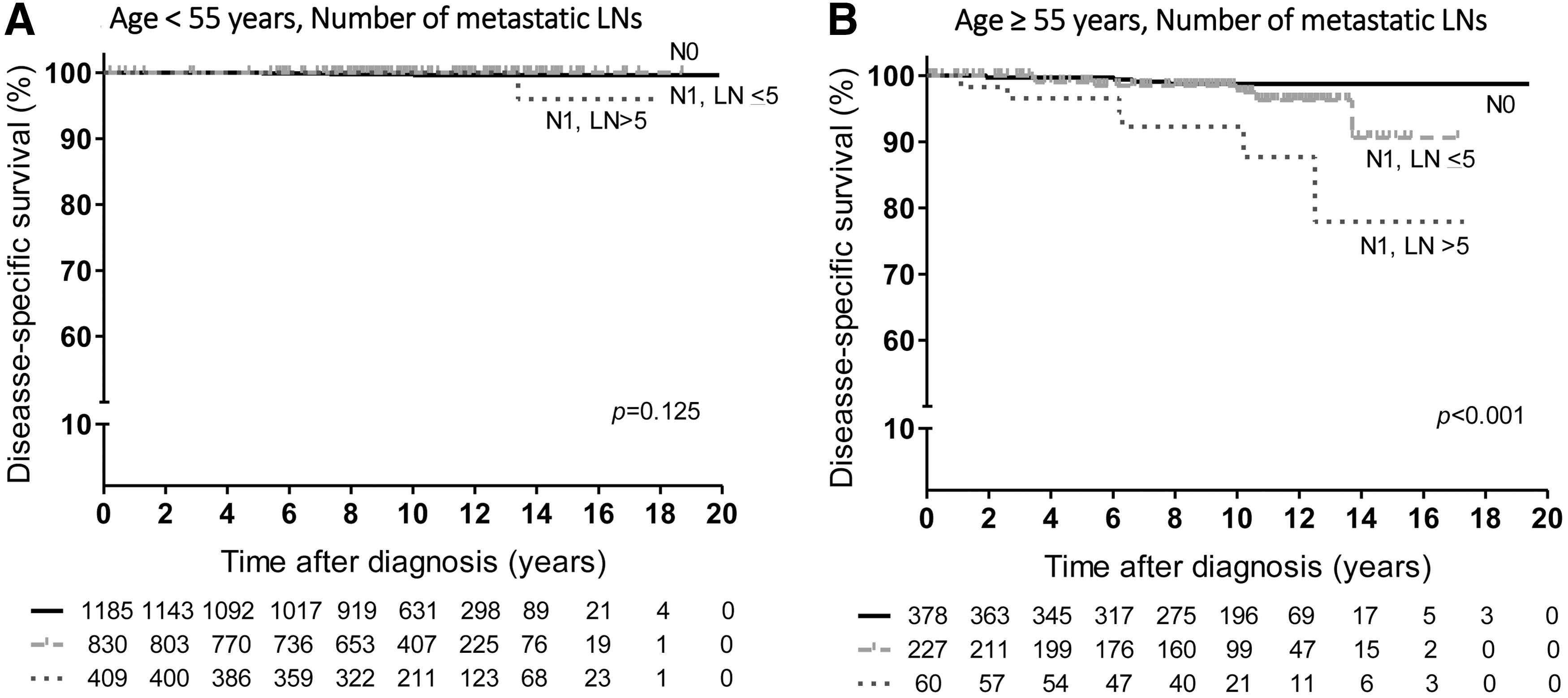
DSS of patients with stage I/II DTC according to the number of metastatic lymph nodes (LNs) after stratifying by age. (
When examining older patients (≥55 years), 378 (57%) patients were classified as N0, 227 (34%) patients as small-volume LNM, and 60 (9%) patients as large-volume LNM group. The 10-year DSS rates of N0, small-volume LNM, and large-volume LNM group were 98.7%, 97.5%, and 92.3%, respectively. DSS was significantly different between the three groups (p < 0.001; Fig. 2B). Patients with large-volume LNM had significantly poorer DSS compared to those with N0 (HR = 10.1 [CI 2.9–36.1]; p < 0.001). When small- and large-volume LNM were compared, patients with large-volume LNM had significantly poorer DSS compared to those with small-volume LNM (HR = 3.9 [CI 1.2–12.0]; p = 0.019).
In older patients (≥55 years), the 10-year OS rates of the N0, small-volume LNM, and large-volume LNM group were 95.8%, 93.2%, and 87.9%, respectively (Supplementary Table S2 and Supplementary Fig. S2). OS was significantly different between the three groups (p < 0.001; Supplementary Fig. S2B), and patients with large-volume LNM had significantly poorer OS compared to those with N0 (HR = 3.7 [CI 1.6–8.5]; p = 0.002).
Survival analysis according to the TNM and modified TNM staging system
DSS was evaluated according to the new TNM (eighth edition) and modified TNM staging system (Table 4 and Fig. 3). According to the TNM-8, 2709 (88%) patients were classified as stage I, and 380 (12%) patients were classified as stage II. The 10-year DSS rates of patients with stage I and stage II disease were 99.8% and 95.4%, respectively. There was a significant difference in DSS according to TNM stages (p < 0.001; Fig. 3A). Patients with stage II had significantly poorer DSS compared to those with stage I (HR = 24.4 [CI 9.7–61.0]; p < 0.001).

DSS of low-stage DTC patients according to (
TNM staging was performed according to the eighth edition of AJCC TNM staging system. Modified TNM staging additionally stratified stage II patients into IIA and IIB. Only N1b patients aged ≥55 years were re-staged as stage IIB, while the remaining patients were stage IIA. Statistically significant values are shown in bold.
The modified TNM staging classifies only N1b patients aged ≥55 years as stage IIB. Based on this modification, 332 (10%) and 48 (2%) patients were re-staged as stage IIA and stage IIB, respectively. The 10-year DSS rates for stage I, IIA, and IIB patients were 99.8%, 96.0%, and 91.4%, respectively. There was a significant difference in DSS between the three groups (p < 0.001; Fig. 3B). Patients with stage IIB had significantly poorer DSS compared to those with stage I (HR = 56.4 [CI 18.2–175.1]; p < 0.001). When the DSS rates between patients with stage IIA and stage IIB were compared, patients with stage IIB also had significantly poorer DSS compared to those with stage IIA (HR = 2.9 [CI 1.1–7.7]; p = 0.030). In patients ≥55 years, patients with stage IIB had significantly poorer DSS compared to those with stage IIA (HR = 3.5 [CI 1.3–10.0]; p = 0.017; Table 4).
OS according to the TNM-8 and modified TNM staging system was also evaluated (Supplementary Table S3 and Supplementary Fig. S3). Stage IIB had significantly poorer OS compared to stage I when analyzing all patients (HR = 11.7 [CI 6.1–22.6]; p < 0.001), as well as in patients ≥55 years (HR = 5.2 [CI 2.3–11.9]; p < 0.001). In older patients (≥55 years), patients with stage IIB had significantly poorer OS compared to those with stage IIA (HR = 2.5 [CI 1.2–5.3]; p = 0.016).
In addition, the PVE and Harrell's c-index of TNM-7 and the modified TNM system were calculated to compare the relative predictability of DSS in patients with stage I/II DTC. The PVE values of TNM-7 and the modified TNM were 2.8% and 2.9%, respectively. The Harrell's c-index of TNM-7 was 0.62 and that of the modified TNM was 0.71.
Discussion
This study demonstrate that the presence of lateral LNM or large-volume LNM was associated with poorer DSS in older patients (≥55 years) with stage I/II DTC. Patients with N1b disease had significantly poorer DSS compared to those with N1a disease. This finding suggests that differentiation between N1a and N1b should be applied to the final TNM staging, especially in older patients. The presence of lateral LNM was also associated with poorer DSS in younger patients (<55 years). However, the 10-year DSS rate of N1b patients was excellent. When the patients were reclassified using a modified TNM staging system, DSS was significantly poorer in patients with stage IIB compared to those with stage IIA. These results indicate that the modified TNM staging system considering N1b classification can improve the predictability of DSS in the TNM staging system.
Metastatic disease in the lateral compartment of the cervical LNs in patients with DTC is known to be a predictive factor of poorer clinical outcomes, particularly in older patients (1 –7,21). Therefore, the degree of LNM was considered as an important variable in the AJCC TNM staging system (11). However, the recently updated TNM staging system (TNM-8) ignores the distinction between N1a and N1b for determining the final staging (9). In this study, the 10-year DSS rates in older patients (≥55 years) with N1b disease was 91.4%, which is lower than that of stage II patients, based on a validation study from the Memorial Sloan Kettering Cancer Center (9). Moreover, N1b disease was associated with significantly poorer DSS compared to N1a disease in older patients. This study only included patients with stage I or stage II disease to minimize the possible impact of T4a, T4b, and M1 disease on DSS. This approach emphasizes the prognostic importance of N1b disease in patients with DTC.
The study also demonstrated that the prognosis deteriorated in older patients with large-volume LNM. Although several studies have shown that the number of metastatic LNs is an independent predictor for the recurrence of DTC, the impact of the number of metastatic LNs on survival has not been well established (1,22). One previous study based on the NCDB and SEER data sets provided evidence that the number of involved LNs may be related to survival (2). Conversely, another study based on data from 10,955 DTC patients from the SEER database suggested that the number of metastatic LNs was not associated with DSS (5). One of the strengths of this study is the longer follow-up duration (median 120 months) compared to this previous study (median 25 months) (5). This allowed more realistic information to be obtained about mortality in patients with DTC. A significant association between DSS and the volume of metastatic LNs is important because prophylactic neck dissection is rarely performed in the lateral neck, and it is not easy to distinguish the anatomic location of metastatic LNs (12). The current TNM staging system only considers the status of LNM in a binary sense (presence vs. absence of metastases) based on anatomical location. However, the degree and quantity of LNM might be considered as a staging variable in the future.
Stage II patients were divided into stage IIA and IIB, defining N1b patients aged ≥55 years as stage IIB. The 10-year DSS rate for stage IIB patients was 91.4%, which was lower than that of conventional stage II patients. In addition, patients with stage IIB disease had significantly poorer DSS compared to those with stage IIA disease. Considering the increased incidence and high prevalence of DTC, changes in survival rate can lead to a significant increase in mortality (2). Therefore, a subclassification based on LNM in patients with stage II DTC will be helpful in predicting disease mortality and establishing a treatment plan.
This study has limitations because of its retrospective design. The study patients were recruited from a single tertiary referral institution, and there is a possibility of selection bias. In addition, patients were treated based on the previous TNM staging system, and some patients who were considered as advanced stage according to the previous TNM staging system were likely to have undergone more aggressive treatment, which influences survival. However, the findings might be helpful for evaluating the actual effect of the presence of lateral LNM or large-volume LNM in low-stage DTC patients when applying the new TNM staging system.
In conclusion, lateral LNM and number of metastatic LNs have a significant prognostic implication in patients with stage I/II DTC, especially in older patients (≥55 years). The study suggests that a modified TNM staging system including N1b would be more useful for the prediction of DSS in patients with DTC.
Footnotes
Acknowledgments
This study was supported by a grant (no. 2017-707) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Author Disclosure Statement
No authors have any conflicts of interest in relation to this manuscript.