
Abstract
Background:
Molecular markers are increasingly used as diagnostic tools in the management of thyroid nodules. There is a paucity of studies evaluating the prevalence of molecular markers in benign lesions.
Patient Findings:
A 68-year-old woman with hypothyroidism presented with a right thyroid nodule, which was atypia of undetermined significance on cytology. The fine-needle aspirate of the nodule was examined with next-generation sequencing and found to harbor a C228T mutation in the TERT gene, a Q61R mutation in the HRAS gene, and an A113_splice mutation in the EIF1AX gene. Right thyroid lobectomy was performed, with final pathology showing follicular adenoma. All three mutations detected in the original fine-needle aspirate specimen were detected in the final surgical specimen as well.
Conclusions:
A rare case of TERT, HRAS, and EIF1AX mutations is reported in a patient with follicular adenoma. TERT promoter mutations may be an early genetic event in the molecular pathogenesis of follicular thyroid carcinoma.
Introduction
M
Patient
A 68-year-old woman with a history of hypothyroidism presented with a right thyroid nodule palpated on routine examination. Ultrasound revealed a 2.4 cm × 2.4 cm nodule within the right thyroid lobe without suspicious features. Fine-needle aspiration (FNA) cytology was atypia of undetermined significance. The tumor was examined with next-generation sequencing (NGS) and found to be positive for the following: a C228T mutation in the TERT gene, a Q61R mutation in the HRAS gene, and an A113_splice mutation in the EIF1AX gene. Given the mutations found on NGS, the patient underwent right thyroid lobectomy, and the final pathology was consistent with a follicular adenoma (Figs. 1 and 2). The lesion was entirely submitted for microscopic evaluation, and multiple levels were performed on all blocks containing the capsule. There was no evidence of capsular or vascular invasion. Genomic analysis of the surgical specimen confirmed the previous cytological analysis showing a C228T mutation in the TERT gene, a Q61R mutation in the HRAS gene, and an A113_splice mutation in the EIF1AX gene. In addition, conventional Sanger sequencing was also performed on both the FNA and surgical specimen, and this confirmed the C228T mutation in the TERT gene. The patient will be followed closely with serial ultrasonography and clinical examinations.
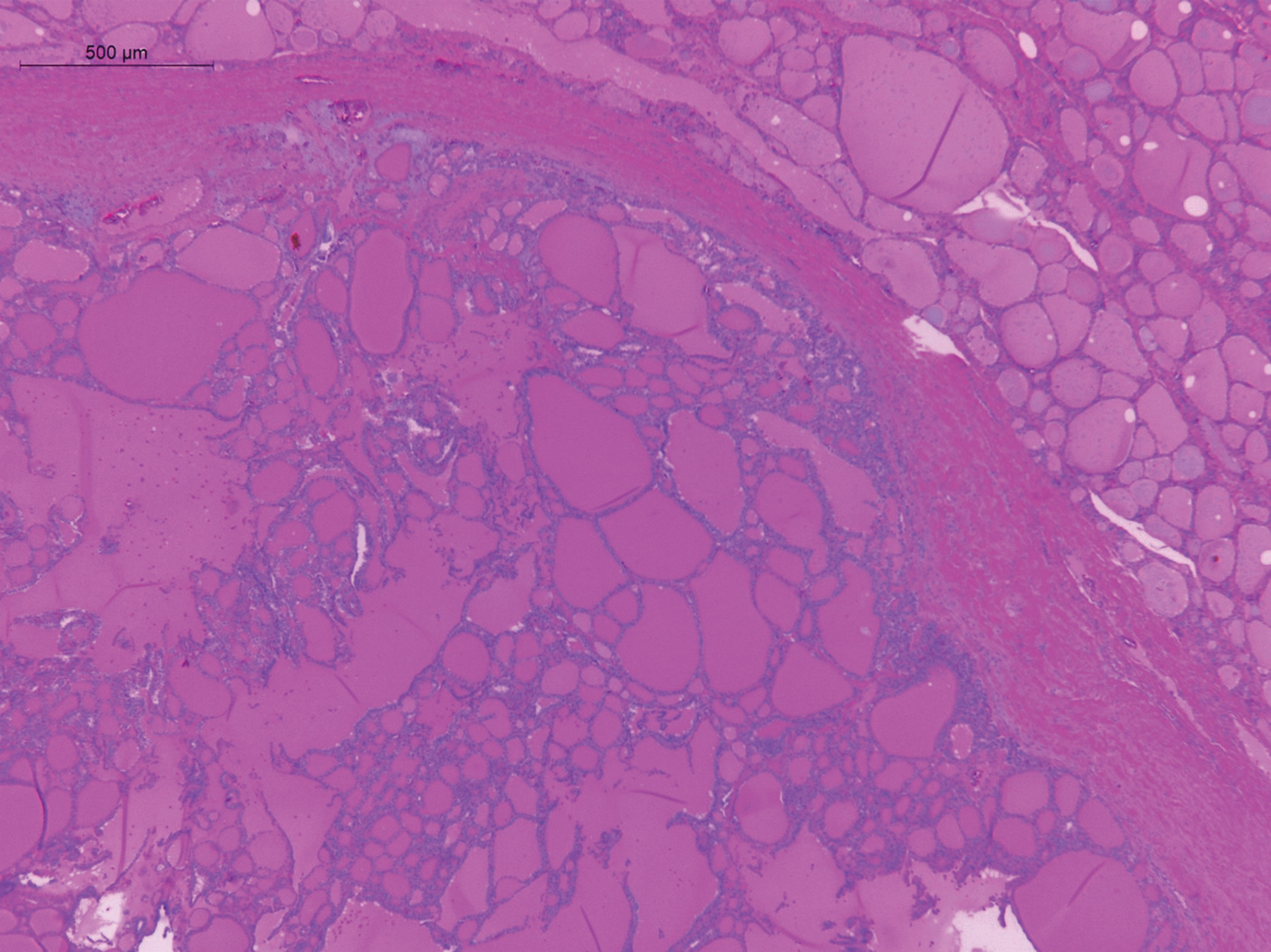
Low-power view (20 × ) showing an encapsulated follicular neoplasm with surrounding normal thyroid. No capsular or vascular invasion was identified.

Intermediate-power view (200 × ) showing the nuclear detail in the nodule and normal thyroid. No nuclear atypia is identified in the nodule.
Methods
FNA sample and formalin-fixed and paraffin-embedded (FFPE) tumor tissue from this patient were extracted for DNA with the QIAamp DNA Micro Kit and QIAamp DNA FFPE Tissue Kit, respectively (Qiagen, Valencia, CA). The NGS panel used to sequence the above-mentioned specimens uses a TruSeq custom amplicon panel designed to detect somatic mutations in 24 thyroid cancer-related genes (AKT1, APC, AXIN1, BRAF, CDKN2A, CTNNB1, DNMT3A, EGFR, EIF1AX, GNAS, HRAS, IDH1, KRAS, NDUFA13, NRAS, PIK3CA, PTEN, RET, SMAD4, TERT promoter, TG, TP53, TSHR, and VHL). The panel covers the full-length coding sequence plus splice sites for tumor suppressors and mutational hotspots for oncogenes. Base calling, mapping, and variant annotation was performed using Illumina's suite. Variant filtering and interpretation was performed using an in-house informatics pipeline (ClinMut Reporter). Given that both the FNA specimen and the final surgical specimen with the follicular adenoma were found to harbor the exact same three mutations, it was concluded that the mutations were genuine.
This report was exempt from Institutional Review Board approval, as it was a case report reporting on preexisting data.
Discussion
A case is reported of follicular adenoma in a nodule with an ominous molecular profile including mutations in the TERT, HRAS, and EIF1AX genes. The TERT promoter mutations C228T and C250T have been identified in thyroid carcinomas to enhance TERT gene transcription and telomerase activation, resulting in sustained cell proliferation (5,6). Traditionally, the presence of a TERT promoter mutation definitively diagnoses a thyroid nodule not only as cancer, but also identifies a cancer with aggressive potential. To the authors' knowledge, there is only a single case of a TERT promoter mutation reported in a benign follicular adenoma (7).
A large study found TERT promoter mutations in 0% (0/179) of benign thyroid nodules and 7.0% of differentiated thyroid cancer (8). Nearly 80% of nodules with TERT promoter mutations were cancers with aggressive clinicopathologic behaviors, such as extrathyroidal invasion, lymph node or distant metastases, disease recurrence, or patient death (8). Among papillary thyroid carcinomas, TERT promoter mutations have been shown to be a risk factor independently for anaplastic transformation (9). In addition, a recent study found that 54% of anaplastic thyroid carcinomas harbored TERT promoter mutations (10).
The present patient also harbored mutations in the EIF1AX and HRAS genes. While EIF1AX mutations have been associated with shorter survival and larger tumors in poorly differentiated thyroid cancers (11), the EIF1AX mutation has also been reported to be present in 7.4% of follicular adenomas (12). RAS mutations have a lower positive predictive value for cancer, with benign nodules positive for the RAS mutation typically being follicular adenoma on final surgical pathology (13). A recent review found that the prevalence of RAS mutations in benign thyroid lesions ranged from 0% to 48%, identifying nine studies that found RAS mutations in >20% of benign lesions (4). Given the presence of molecular markers in benign lesions, further studies are needed to characterize the prevalence of these markers better.
It should be noted that the one prior documented case of a TERT promoter mutation in a follicular adenoma was a patient who ultimately developed tumor recurrence and died of FTC (7). While this may have been due to misdiagnosis at the initial histopathological evaluation, the authors suggested that TERT promoter mutations may occur as an early genetic event in follicular thyroid tumors that have not developed malignant features on routine histopathologic workup (7). Although follicular adenomas are classified as benign, there is evidence that suggests that they may represent a precancerous lesion that may progress to malignancy (3,13). In addition, RAS mutations may synergize the role of TERT promoter mutations through activating the PI3K pathway (8). Therefore, the plan is to observe this patient closely with serial ultrasounds and examinations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.