
Abstract
Background:
Iodine is an important element for the synthesis of thyroid hormone, and its deficiency or excessive intake is associated with various thyroid diseases. Little is known about the association between iodine status and thyroid function among children and adolescents living in iodine-rich areas. Therefore, this study analyzed this association using data from a nationwide survey.
Methods:
From the Korea National Health and Nutrition Examination Surveys VI (2013–2015) data, 1288 subjects (711 male) aged 6–19 years who underwent a urinary iodine concentration (UIC) test and 1000 subjects (564 male) aged 10–19 years who underwent a thyroid function test were included in this study. Serum levels of thyrotropin (TSH), free thyroxine (fT4), and thyroperoxidase antibodies (TPOAb) were analyzed. Subclinical hypothyroidism (SCH) was defined as TSH >5.5 μIU/mL with a normal fT4 level. Median daily iodine intake was calculated from the UIC. Daily sodium intake was derived from the nutritional survey data of 1181 subjects.
Results:
The median UIC was 449 μg/L (range 15–21,905 μg/L), and the prevalence rates of UIC ≥300 μg/L and ≥1000 μg/L were 64.9% and 25.0%, respectively. The prevalence rates of a sodium intake >2000 mg/day and iodine intake >2400 μg/day were 75.0% (885/1181) and 12.7% (164/1288), respectively. The prevalence rates of SCH and TPOAb >34 IU/mL were 7.2% (72/1000) and 2.3% (23/1000), respectively. The prevalence of SCH was significantly higher in the iodine deficient and iodine excess groups compared to those in the UIC 100–299.9 μg/L group (p = 0.038). Therefore, there was a U-shaped and inverted U-shaped correlation between serum levels of TSH and fT4 with UIC, respectively. These correlations were especially prominent when UIC was >1000 μg/L. There was no definite correlation between TPOAb and UIC.
Conclusions:
Excess iodine was prevalent in Korean children and adolescents, and it may be associated with SCH. Therefore, monitoring the iodine status and education on adequate intake are needed in iodine-rich areas.
Introduction
I
Although most individuals tolerate a high dietary iodine intake well (1), individuals with antithyroid antibodies have a higher risk of developing thyroid dysfunction when the iodine intake is high (8,9). The association with excessive iodine intake and impaired thyroid function is also found in children in areas with high nutritional iodine intake (10). The relationships between excessive iodine intake and subclinical hypothyroidism in preterm infants was previously reported (11). However, the relationship between thyroid function and iodine intake in subjects who have normal thyroid function is not known, especially in children and adolescents living in iodine-rich areas. The effects of excessive iodine intake can decrease the response of the thyroid to thyrotropin (TSH), acutely inhibit iodide uptake and oxidation, and, at high concentrations, inhibit thyroid hormone secretion (12).
Korea is a peninsula surrounded by iodine-rich water on three sides. The Republic of Korea (South Korea) is regarded as an iodine-sufficient area, but the iodine intake in South Korea is even more than adequate (13 –15). Most ingested iodine is eventually excreted in the urine, and only a small amount appears in the feces (1). Because 90% of ingested iodine is cleared by the kidneys within 24–48 hours (16), median spot urinary iodine concentrations (UIC) are used as a biomarker to determine dietary iodine intake at the population level. This study reports the iodine status in healthy children and adolescents aged 6–19 years. It analyzes the relationship between UIC and thyroid function based on a nationwide survey, the first data of this type in Korea and determines urinary sodium concentrations to assess for an eventual correlation with UIC and to characterize better the source of iodine ingestion.
Methods
Data from the first year (2013) and the third year (2015) of the Korea National Health and Nutrition Examination Surveys (KNHANES) VI were included in the present study. The KNHANES is a national survey based on a health interview survey, nutrition survey, and health examination. Since 1998, the KNHANES has been periodically performed to investigate the health and nutritional status of the Korean population. This survey uses a stratified, multistage, clustered probability sampling method to select a representative sample of the non-institutionalized civilian Korean population.
Of the 1,757,400 primary sampling units (based on the 2010 National Census Registry), 192 sampling units per year, total 576 sampling units were randomly selected during the 2013–2015 surveys. A total of 22,948 individuals participated in the health interviews and examinations, as well as the nutrition survey. Of these, 3782 individuals were aged 6–19 years. All survey participants provided informed consent. The Institutional Review Board of the Korea Centers for Disease Control and Prevention approved using these open data.
Random single-voided urine samples for UIC (μg/L) were collected in one third of subjects aged ≥10 years in 2013 and 2014 and in all subjects aged ≥6 years in 2015. Thyroid function tests (TFTs) were performed in one third of subjects aged ≥10 years in 2013–2015. Therefore, 1297/3872 subjects aged 6–19 years who underwent UIC examination and 1009/1297 subjects who were 10–19 years of age with available TFTs were included in this study. UIC can be expressed in micrograms per liter of urine or as micrograms per gram of creatinine. The results tend to be similar (17). This study used micrograms per liter of urine.
Daily sodium intake (mg/day) was assessed using a 24-hour dietary recall method. Daily iodine intake was calculated using the following formula (18): Daily iodine intake (μg/day) = UIC (μg/L) × 0.0235 × body weight (kg). Anthropometric data were collected from the subjects wearing light clothing without shoes or jewelry. Weight was measured to the first decimal place with a GL-6000-20 digital scale (CAS Korea, Seoul, Korea). Spot urine samples and serum samples were obtained from the subjects and stored at −20°C until analysis. UIC was measured via inductively coupled plasma-mass spectrometry (PerkinElmer, Waltham, MA) and iodine standard (Inorganic Ventures, Christiansburg, VA).
Serum levels of TSH, free thyroxine (fT4), and thyroperoxidase antibodies (TPOAb) were measured using electrochemiluminescence immunoassays (Cobas 8000-E602; Roche, Mannheim, Germany). The normal reference values were as follows: TSH 0.35–5.50 μIU/mL, fT4 0.89–1.76 ng/dL, and TPOAb <34 IU/mL. Subclinical hypothyroidism (SCH) was defined as a serum level of TSH >5.5 μIU/mL with normal fT4 levels (0.89–1.76 ng/dL).
Only euthyroid individuals were included in this study. Subjects with overt hyperthyroidism or overt hypothyroidism were excluded according to diagnostic criteria described as follows: eight subjects who showed hyperthyroxinemia (fT4 >1.76 ng/dL) with TSH suppression (TSH <0.35 μIU/mL), and one subject who showed hypothyroxinemia (fT4 <0.89 ng/dL) with TSH elevation (TSH >5.50 μIU/mL). Therefore, 1288 subjects (711 males and 578 females) were finally enrolled in this study (Fig. 1).
Flow chart of the selection process.
Statistical analysis
All data are presented as medians with ranges (minimum–maximum). Non-normally distributed data, such as UIC, serum levels of TSH, fT4, and TPOAb, were transformed with the natural logarithm before analysis. Student's t-test or the chi-square test was used to compare data between sexes. One-way analysis of variance with post hoc Bonferroni correction was used to compare data between groups according to age or UIC. The Mantel–Haenszel test (linear-by-linear association) was used to compare the prevalence of iodine excess according to age or UIC group. Pearson's correlation coefficient was calculated to test the association between two continuous parameters. The quadratic model was used to describe the best fit of the TSH and fT4 plotted against UIC. All statistical analyses were performed using IBM SPSS Statistics for Windows v21.0 (IBM Corp., Armonk, NY). p-Values of <0.05 were considered significant.
Results
UIC and sodium intake
In a total of 1288 subjects, the median UIC was 449 μg/L (15–21,905 μg/L; (Table 1), and there were no significant differences between males and females (p = 0.480). The prevalence rate of UIC ≥300 μg/L was 64.9% (65.1% in males vs. 64.6% in females; p = 0.859), and the prevalence rate of UIC ≥1000 μg/L was 25.0% (25.9% in males vs. 24.0% in females; p = 0.461). The prevalence rate of iodine insufficiency (UIC <100 μg/L) was 5.4%, and there was a significant sex difference (4.0% in males vs. 7.1% in females; p = 0.019).
Data are expressed as median and ranges (minimum–maximum).
UIC, urinary iodine concentration.
The median sodium intake (n = 1180) and median iodine intake (n = 1288) were 2971 mg/day (239–66,652 mg/day) and 535 μg/day (15–24,606 μg/day), respectively. The prevalence rates of sodium intake >2000 mg/day and iodine intake >2400 μg/day, which are the recommended upper limit values for adult Koreans (19), were 75.0% (885/1180) and 12.7% (164/1288), respectively. There was no relationship between sodium intake and UIC in the simple correlation analysis (p = 0.865).
Prevalence of TFT abnormalities
Of 1288 subjects, 1000 underwent TFTs, and the median (ranges) of serum levels of TSH, fT4, and TPOAb were 2.5 μIU/mL (0.2–11.8 μIU/mL), 1.29 ng/dL (0.81–2.07 ng/dL), and 5.7 IU/mL (5.0–328.4 IU/mL), respectively (Table 2). The prevalence rate of SCH was 7.2% (6.6% in males vs. 8.0% in females; p = 0.373), and the prevalence rate of TPOAb >34 IU/mL was 2.3% (1.6% in males vs. 3.2% in females; p = 0.091). The differences in age distributions were not significant (SCH: p = 0.121; TPOAb >34 IU/mL: p = 0.585). Only one subject showed a TSH <0.35 μIU/mL, but his fT4 level was 1.30 ng/dL.
Data are expressed as median and ranges (minimum–maximum).
Reference ranges: TSH 0.35–5.50 μIU/mL; fT4 0.89–1.76 ng/dL; TPOAb, 0–34 IU/mL.
TSH, thyrotropin; fT4, free thyroxine; TPOAb, thyroperoxidase antibody.
Five subjects had fT4 concentrations >1.76 ng/dL (1.78, 1.81, 1.83, 1.90, and 2.07 ng/dL). This was not considered to be clinically significant because their TSH levels were not suppressed (1.7, 1.6, 2.9, 3.9, and 2.5 μIU/mL, respectively). Six subjects had fT4 concentrations <0.89 ng/dL (0.81, 0.83, 0.83, 0.83, 0.87, and 0.88 ng/dL). This was not considered to be clinically significant because their TSH levels were not elevated (3.8, 3.1, 2.5, 1.3, 3.3, and 4.6 μIU/mL, respectively).
There were only three subjects who showed TSH concentrations >5.5 μIU/mL and TPOAb >34 IU/mL, and no significant difference in the prevalence of SCH between the TPOAb-positive group and TPOAb-negative group was found (p = 0.226).
Correlation between UIC and TFT
The UIC was correlated positively with TSH (r = 0.091; p = 0.004) and negatively with fT4 (r = −0.091; p = 0.004), but the Pearson's correlation coefficients were weak. Therefore, the quadratic model was applied. There were U-shaped and inverted U-shaped correlations between serum levels of TSH (Fig. 2A) and fT4 (Fig. 2B) with UIC, respectively (Fig. 2 uses logarithmic scales for the TSH and fT4 axis). These correlations were more prominent when UIC was >1000 μg/L.
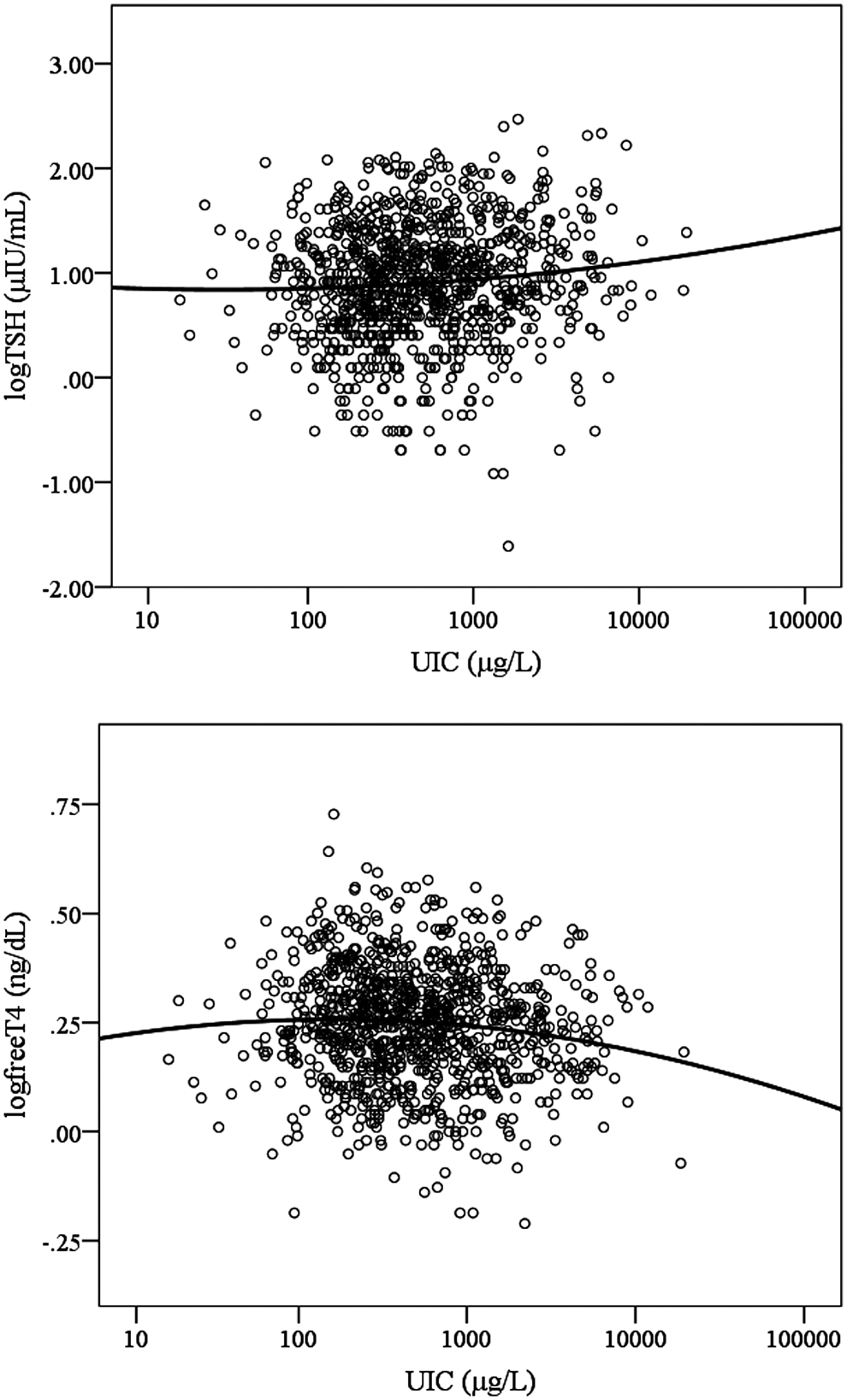
A scatterplot with a trend line of TSH versus UIC (
The subjects were divided into six groups according to UIC: deficient (<100 μg/L), adequate (100–199.9 μg/L), more than adequate (200–299.9 μg/L), and excessive (mild: 300–599.9 μg/L; moderate: 600–999.9 μg/L; and severe: ≥1000 μg/L; Table 3). In contrast to the iodine intake, the sodium intake showed no differences between groups. The serum levels of TSH and fT4 showed significant differences between groups. This trend coincided with that seen in Figure 2A and B. The prevalence of SCH was significantly higher in the iodine-deficient and iodine-excessive groups compared to the group with an UIC of 100–299.9 μg/L (p = 0.038). The serum levels of TPOAb showed no significant differences between groups (p = 0.233).
Data are expressed as median and ranges (minimum–maximum).
TFT, thyroid function test.
Discussion
According to the results of the KNHANES VI, the median UIC of Korean children and adolescents aged 6–19 years was 449 μg/L, and this value corresponds to iodine excess. More than half of the subjects had UIC levels >300 μg/L, and a quarter of subjects had UIC levels >1000 μg/L. Moreover, the prevalence rate of UIC ≥300 μg/L in young children aged 6.0–7.9 years was >80%. Most importantly, there were U-shaped and inverted U-shaped correlations between the serum levels of TSH and fT4 with UIC, respectively. There was no definite correlation between thyroid autoimmunity and UIC in subjects <19 years of age.
The reason for a high UIC is due to excessive intake of iodine. In Korea, iodized salt and seaweed, including laver, sea mustard, and kelp, are easily obtained, and these iodine-rich foods are popular and traditional. From the KNHANES, high daily sodium intakes could be seen among Korean children and adolescents, with median values of >2000 mg/day in children >6 years of age and even >3000 mg/day in children >13 years of age (data not shown). Contrary to expectations, there was no correlation between daily sodium intake and UIC, which implies that the major source of iodine is seaweed rather than iodized salt in Korea. The upper limits for daily iodine intake is 500 μg/day in children (aged 6–11 years), approximately 2000 μg in adolescents (aged 12–18 years), and 2400 μg/day in adults (19), which are higher than those in the United States (20). When these criteria were applied, 46.9% (173/369) of children and 17.3% (141/813) of adolescents were found to consume iodine above the upper limits of dietary reference intakes in Korea. A relatively high prevalence of excessive iodine intake in children may be due to milk and dairy products, which are also important iodine sources (21).
The chronic exposure to excessive iodine already beginning at a young age may impact the incidence of thyroid disease. However, little is known about the long-term consequences of iodine excess, especially when UIC is >1000 μg/L. The results from a study of children aged 8–10 years in China showed an increased goiter rate after universal salt iodization (22). In a study by Gao et al. in children aged 6–11 years, the prevalence of SCH in three groups (mean UIC 631 μg/L vs. 338 μg/L vs. 99 μg/L) showed a higher prevalence of SCH in subjects with high iodine intake (20.5% vs. 14.6% vs. 4.3%) (23). This prevalence was higher than in the present study. More longitudinal studies are needed to determine whether children with continued SCH from exposure to iodine intake that is more than adequate will develop overt hypothyroidism. However, SCH itself needs regular monitoring by TFTs (24), which may result in increasing medical costs.
The mechanism of hypothyroidism resulting from iodine excess, especially in association with autoimmunity, is still controversial. A previous study has suggested that preceding thyroid gland damage from an autoimmune reaction may be an important factor (17), whereas high iodine intake itself may induce thyroid autoimmunity (25). Nevertheless, it is certain that there is a close relationship between excessive iodine status and autoimmune thyroiditis (26,27). Some studies revealed TPOAb as one of the risk factors for SCH after adjustment for age and sex (28), even in children (10). This study also analyzed the correlation between serum levels of TPOAb and TSH with UIC, but no significant association was found. There may be several reasons for this finding. First, the small number of subjects with positive TPOAb in this study may impact the results. According to a previous study, the prevalence of positive TPOAb was 4% in young Korean adults aged 20–29 years (29), which is much lower than in the United States (30). Therefore, further studies are needed to investigate the prevalence of thyroid autoantibodies in Koreans. Second, other thyroid autoimmunity factors such as thyroglobulin antibodies (TgAb) were not evaluated. Latrofa et al. suggested that iodine contributes to thyroid autoimmunity by unmasking a cryptic epitope on thyroglobulin. Therefore, iodine-induced thyroid autoimmunity may perhaps primarily lead to the development of TgAb rather than TPOAb (31). The other mechanism suggested is a non-functional Wolff–Chaikoff effect. In an environment of iodine excess, a slightly elevated TSH may keep the sodium–iodide symporter active (17).
There are some limitations to this study. In the KNHANES, UIC was based on a single random spot urine collection. It is difficult to collect 24-hour urine samples, so spot urine samples are generally used in field studies. However, due to day-to-day variation in iodine intake and hydration, several spot urine collections with mean values of UIC are more reliable (32). Because of this variation, some recommendations state that at least 10 repeat spot urine collections are required to estimate an individual's iodine intake with acceptable precision (33,34). Second, the subjects' pubertal status or bone age, which may impact UIC, was not included in the KNHANES data. Third, other parameters, such as thyroglobulin, TgAb, thyroid volume, goiter, or nodules, were not determined. Thyroglobulin is known as a potential biomarker of iodine status (35), which could provide more information about an individual's iodine status. Despite these limitations, the strength of this study is its nationwide coverage, which may compensate for these weaknesses.
In conclusion, iodine excess was prevalent in Korean children and adolescents, which may result in SCH. Therefore, monitoring of the iodine status and education for an adequate intake is needed in areas of excessive iodine.
Footnotes
Acknowledgments
We thank the Korea Centers for Disease Control and Prevention, who performed the KNHANES.
Author Disclosure Statement
All authors have no conflicts of interest.