
Abstract
Background:
Recently, thermal ablation has been proposed for treating primary papillary thyroid carcinoma (PTC), triggering an extensive debate. This study aimed to analyze surgical outcomes of post-ablation cases to investigate the effectiveness and safety of thermal ablation in primary PTC.
Methods:
Primary PTC patients treated with thermal ablation were retrospectively searched for from the authors' medical record database prior to August 2017. The surgical patients met the following criteria: (i) primary PTC treated with thermal ablation, (ii) findings suspicious for malignancy of the post-ablation lesions on ultrasound or malignancy confirmed by cytology, or with clinical evidence of cervical lymph node metastasis (LNM), (iii) written informed consent for surgery, (iv) preference for definite diagnosis of the post-ablation lesions for the patients without evidence for malignant findings, and (v) tolerance of a thyroidectomy and without severe illness. Moreover, a systematic review of the literature was made to analyze relevant cases.
Results:
Twelve patients with an average age of 41.0 ± 13.6 years constituted the Fudan University Shanghai Cancer Center cohort in this study. Twenty-two foci with a mean size of 1.3 ± 0.7 cm were ablated percutaneously under ultrasound guidance. Residual PTCs were confirmed in all cases by histopathology, and LNM was present in 66.7% (8/12) of the patients. Intraoperatively, adhesion of the post-ablation lesions with the strap muscles was observed in six cases. Strap muscles were found to be cauterized in five cases, and notably the recurrent laryngeal nerve was involved in one case. Furthermore, seven relevant studies from Korea, Italy, and China were retrospectively reviewed, and incomplete ablation of primary PTC and omission of LNM by thermal ablation were observed frequently.
Conclusions:
Surgical therapy demonstrated incomplete ablation of primary PTC and omission of LNM by thermal ablation in this cohort of patients. Thermal ablation should be recommended with caution as treatment of operable patients with primary PTC.
Introduction
O
Materials and Methods
Patients
Primary PTC patients treated with thermal ablation were retrospectively searched for from the authors' medical record database. A total of 12 patients who received surgical therapy at Fudan University Shanghai Cancer Center (FUSCC), Affiliated Hospital of Jiangsu University, and Tumor Hospital of Mudanjiang City from March 2014 to August 2017 were enrolled in the present study. The surgical patients met the following criteria: (i) primary PTC treated with thermal ablation, (ii) findings suspicious for malignancy of the post-ablation lesions on ultrasound (US) or malignancy confirmed by cytology or with clinical evidence of cervical LNM, (iii) written informed consent for surgery, (iv) preference for definite diagnosis of the post-ablation lesions for the patients without evidence for malignant findings, and (v) tolerance of a thyroidectomy and without severe illness. Those primary PTC patients treated with thermal ablation who did not meet the above criteria received active surveillance in the hospitals. Seven nonsurgical patients with primary suspicious PTC treated previously with thermal ablation were collected from the outpatient database at FUSCC. The medical records were reviewed for the collection of clinical, radiological, surgical, and pathological data, and data on clinical information (age and sex), US features, thermal ablation methods, cytological diagnosis, intraoperative findings, and histopathological outcomes were abstracted from the patients' records. The US results were recorded according to the risk stratification of Thyroid Imaging Reporting and Data System, as described in a previous study (18), and cytological diagnoses were evaluated based on The Bethesda System for Reporting Thyroid Cytology (19), including six categories: (i) nondiagnostic/unsatisfactory (ND/UNS), (ii) benign, (iii) atypia/follicular lesion of undetermined significance, (iv) follicular neoplasm/suspicious for follicular neoplasm, (v) suspicious for malignancy, and (vi) malignant. The patients were staged using the updated 2016 TNM classification of the American Joint Committee on Cancer/International Union against Cancer (eighth edition) for DTC (20). The cervical compartment of lymph node regions (levels II–VI) referred to the Memorial Sloan Kettering Cancer Center's classification (21). Each patient provided a written informed consent for his/her specimens and information to be used for research and stored in the hospital database. All the procedures performed in the study were in accordance with the ethical standards of the institutional research committee and the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Surgical therapies
The surgical procedure was performed based on the sonographic findings and cytological results of the enrolled post-ablation cases. According to US results, a hemithyroidectomy was usually performed for patients with unilateral lesions suspicious for PTC, and the next surgical procedures were guided by the pathological outcomes of frozen sections. If the lesions proved to be malignant, an ipsilateral central lymph node dissection (CLND) was then performed. A total thyroidectomy was performed on patients with bilateral lesions suspicious for PTC or with unilateral high-risk malignancy. A modified lateral lymph node dissection (LLND) was performed only in the cases with clinically evident lateral neck LNM (levels II–V).
Literature review
A systematic review of the literature was made to analyze relevant cases. PubMed, EMBASE, and Ovid were used to identify potentially relevant articles published prior to August 2017. The literature was searched using the keywords “thyroid” and “tumor/cancer/carcinoma” and “radiofrequency ablation” or “microwave ablation” or “laser ablation” or “thermal ablation.” Retrospective and prospective studies and case reports were included that investigated surgical and histopathological outcomes of post-ablation patients with primary thyroid carcinoma. The study selection criteria were as follows: (i) primary suspicious thyroid tumor treated with thermal ablation, (ii) receiving surgical therapy, and (iii) availability of histopathological outcomes. Some original articles and review articles that failed to provide complete medical records of patients were excluded.
Statistical analysis
Continuous variables are expressed as means ± standard deviation (SD). Categorical results are summarized with frequencies and percentages. The occurrence rates of residual tumor and LNM were analyzed in the FUSCC cohort and the literature cohort, respectively. Statistical analyses were performed using IBM SPSS for Windows v22.0 (IBM Corp., Armonk, NY).
Results
Clinical features of ablation cases
A total of 12 patients (10 females) with an average age of 41.0 ± 13.6 years (range 21–60 years) were enrolled in the study. Twenty-two foci with a mean size of 1.3 ± 0.7 cm (range 0.3–2.5 cm) were ablated percutaneously under US guidance in the 12 patients. Moreover, it was found that thermal ablation was also performed on metastatic lesions in two cases (cases 4 and 12) with suspicious LNM on US. As shown in Table 1, all 12 patients were diagnosed with lesions highly suspicious for PTC on US before thermal ablation, and nine of them were confirmed to be malignant or suspicious for malignancy by ultrasound-guided fine needle aspiration biopsy. After thermal ablation, the post-ablation lesions of the 11 patients (cases 2–12) remained suspicious for malignancy on US during follow-up (Fig. 1). In three cases (cases 2, 11, and 12), the lesion was suspicious for malignancy on cytology, and notably there was one case (case 3) who developed suspicious LNM in cervical region VII after one year of follow-up. The 11 patients required surgical therapy in the authors' hospitals. For case 1, there was no suspicious feature for malignancy on US, but the patient preferred surgery to obtain a definite diagnosis of the post-ablation lesions. The clinical features of the ablation cases are summarized in detail in Table 1.
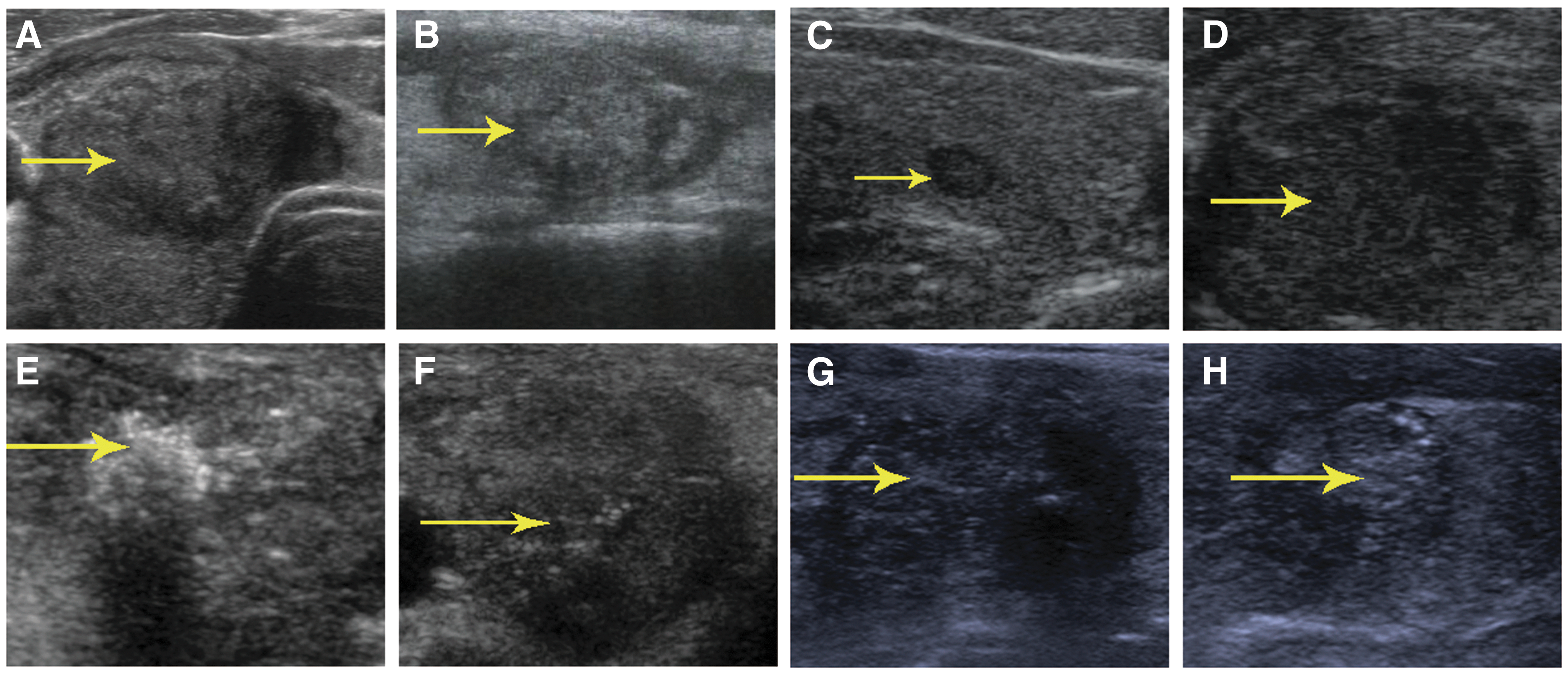
The ultrasound (US) pattern images of the post-ablation lesions in the surgical cases. (
PTC, papillary thyroid carcinoma; US-TIRADS, ultrasound-thyroid imaging report and data system; US-FNAB, ultrasound-guided fine-needle aspiration biopsy; SM, suspicious for malignancy; ND/UNS, non-diagnostic/unsatisfactory; RFA, radiofrequency ablation; MWA, microwave ablation.
Additionally, of the seven nonsurgical patients with primary PTC treated previously with thermal ablation, two patients harbored no malignant evidence in the post-ablation lesions on US during follow-up. Suspicious features of the post-ablation lesions were observed in the other five patients, and one patient showed growth of the post-ablation lesion after 19 months of follow-up. However, these patients refused immediate surgery and preferred active surveillance. Supplementary Table S1 and Supplementary Figure S1 (Supplementary Data are available online at
Surgeries and intraoperative findings
Six out of the 12 patients underwent total thyroidectomy, while the others were operated with hemithyroidectomy. CLND was performed ipsilaterally in all patients. LLND was performed in cases 4 and 12 with suspicious LNM in the lateral neck on US imaging, and level VII dissection was conducted in case 3. Intraoperatively, adhesion of the post-ablation lesions with the strap muscles was observed in six cases (cases 1, 4, 6, 10, 11, and 12). As shown in Table 2, the strap muscles were found to be cauterized in cases 1, 4, 10, 11, and 12, and notably the recurrent laryngeal nerve was involved in case 10. The involvement of perithyroidal tissues through the ablation process is shown in Figure 2. Tumor extension was also observed in cases 2 and 10, whereas there was no evidence of extension on the preoperative US and computed tomography (CT). Figure 3 shows the post-ablation outcomes on CT imaging and the gross findings of two lesions after resection in case 11, and Figure 4D shows the left post-ablation lesion of case 12.
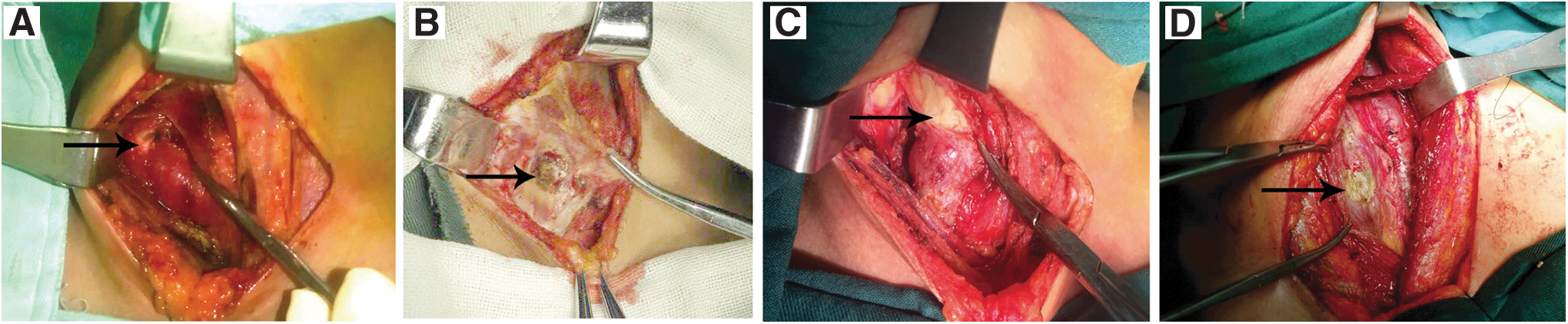
Involvement of perithyroidal tissues after percutaneous thermal ablation. (
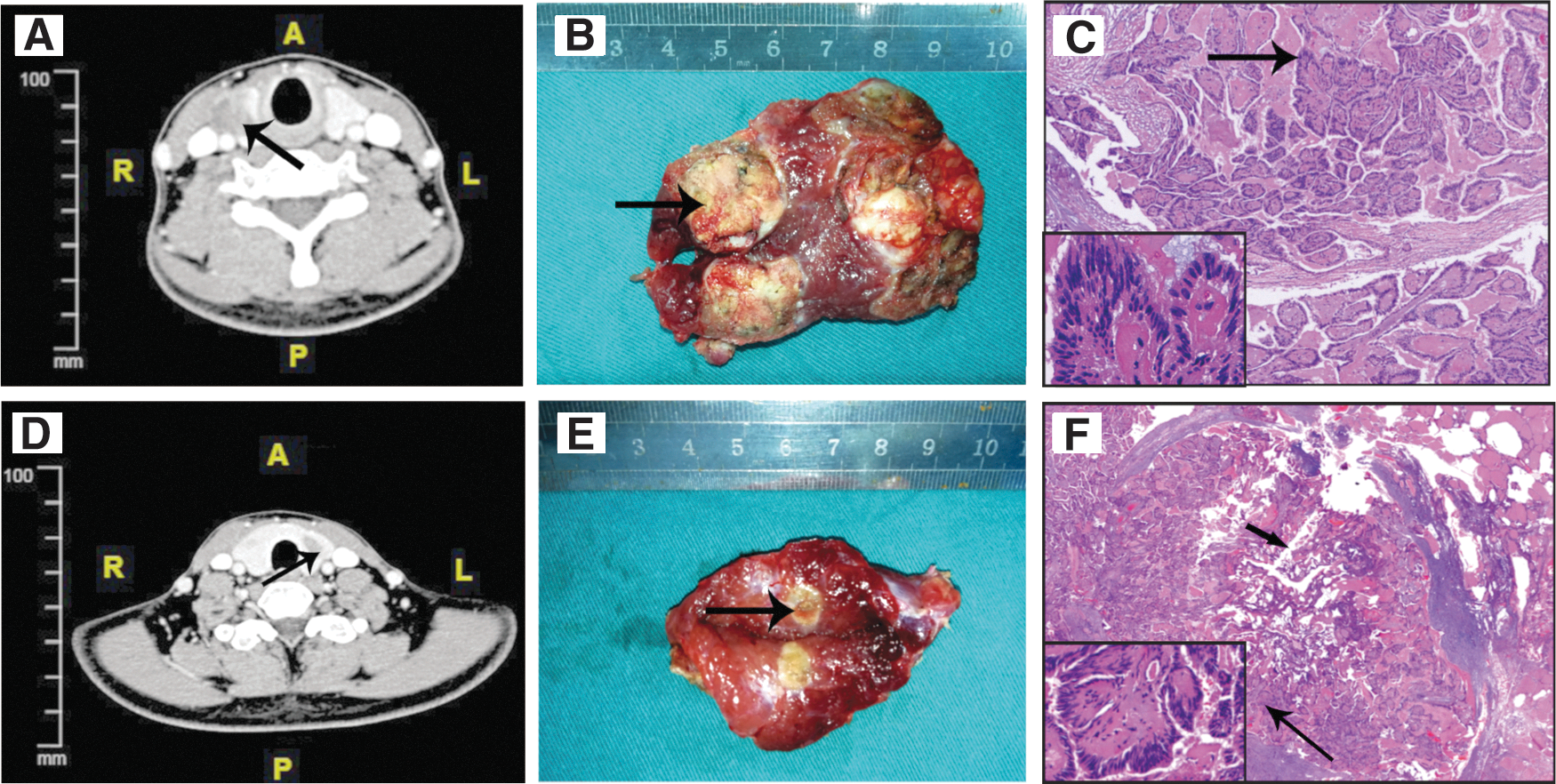
Computed tomography (CT) image, gross findings, and histological outcomes of the post-ablation lesions in case 11. (
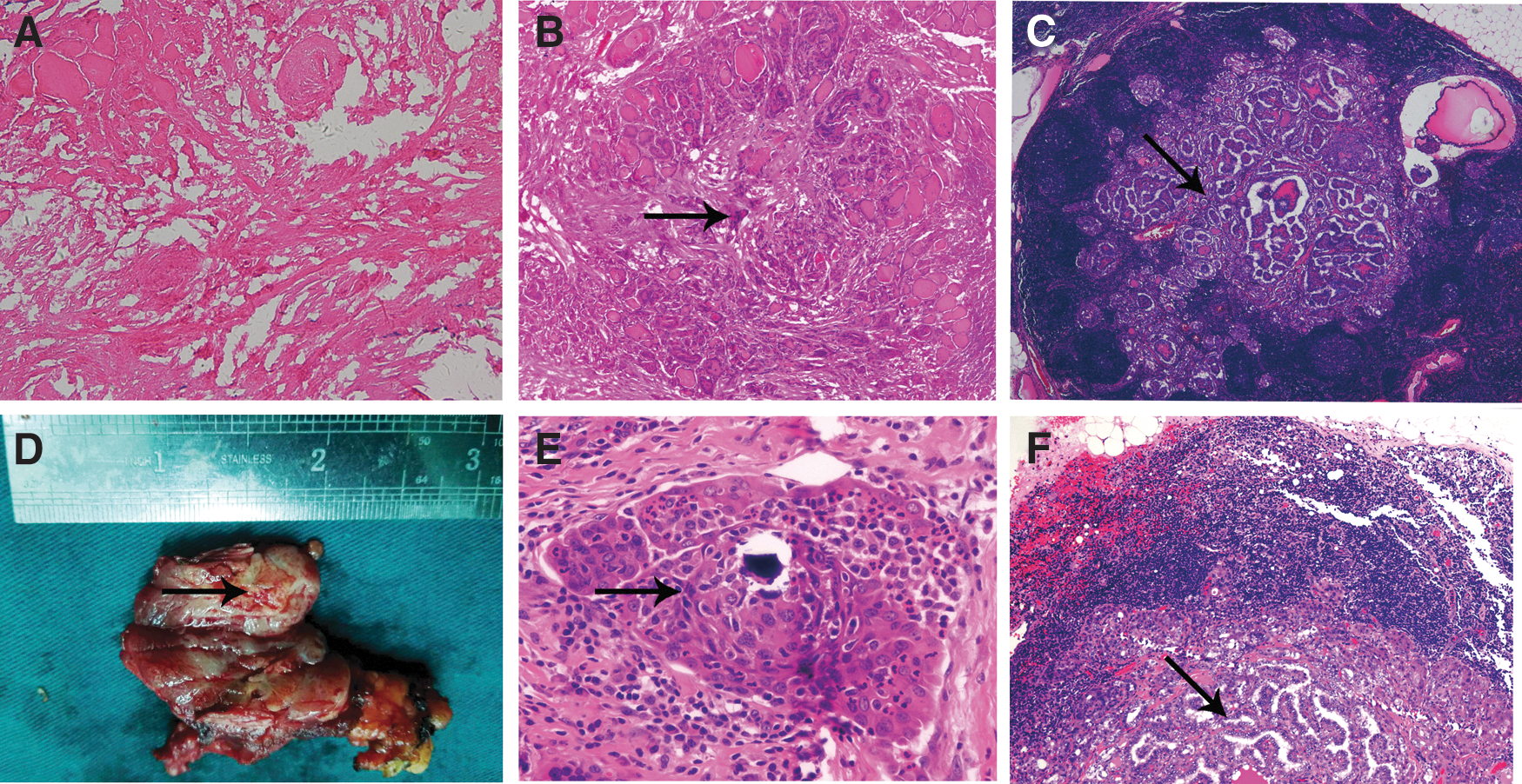
Histological confirmation of primary PTC and LNM in cases 9 and 12. (
pMultifocality, pathological multifocality; pTNM stage, pathological tumor-node-metastasis stage; FN, follicular neoplasm.
Histopathological results of surgical cases
As shown in Table 2, residual PTCs were confirmed in all 12 cases by histopathology. Histological features of the post-ablation lesions in cases 10, 11, and 12 are shown in Figures 3 and 4. Of the 12 patients with residual foci, multifocality was present in nine cases (75.0%), and tumor extension was found in two cases (16.7%). Furthermore, the rates of pT1, pT2, and pT3 were 58.4%, 33.3%, and 8.3% of all cases. LNM was found in 66.7% (8/12) of the patients, with pN1a in six patients and pN1b in two patients. Figure 4 shows the histopathological features of the LNM in cases 9 and 12. The post-ablation residual findings and LNM of the cohort are shown in detail in Supplementary Table S1.
Literature review
Through searching electronic databases, seven studies were identified that addressed surgical and histopathological outcomes after ablation of primary thyroid carcinomas. As shown in Table 3, the seven studies included 17 cases, and they consisted of three prospective studies and four retrospective studies from Korea, Italy, and China. After undergoing thyroidectomy, eight cases (47.5%) were confirmed to have residual PTC by histopathology, and interestingly two out of the nine cases with no identification of residual tissue after ablation were found to have remaining PTC. Of the 17 cases, seven cases (41.2%) proved to harbor LNM after surgery (Supplementary Table S2).
FTC, follicular thyroid carcinoma.
Discussion
Thermal ablation techniques have been demonstrated to be effective and safe in volume reduction for benign thyroid nodules (22 –24). Additionally, local disease control can be achieved in inoperable patients with recurrent thyroid cancers (5), and selected distant thyroid cancer metastases can be treated by thermal ablation (15). In recent years, extensive debate about the role of thermal ablation in primary thyroid carcinomas has arisen. Some authors (6 –8,12,14,25) have highlighted the potential of thermal ablation treatment in the management of PTMC, considering the indolent course and good prognosis of PTMC. Several studies from multiple centers have investigated the use of thermal ablation in PTMC, demonstrating its effectiveness and safety in low-risk patients during short-term follow-up (6 –8,12,14,25). However, a number of surgeons and researchers have raised concerns that thermal ablation may result in incomplete treatment and potentially additional surgeries for patients with primary thyroid carcinomas because of a high incidence of multifocality and LNM in PTC. Lee et al. (9) and Oddo et al. (10) reported a case of local tumor seeding after percutaneous ablation for a primary thyroid carcinoma. It has been shown that several cases of primary PTC have been treated incompletely with RFA by subsequent surgeries in case reports by Kim et al. (11) and Dong et al. (26).
In this study, all 12 cases were confirmed to be incompletely treated by RFA based on histopathology findings, although several foci were thoroughly ablated. Not only were primary lesions confirmed to have residual tumor but metastatic lymph nodes were also identified that were not submitted to ablation in some cases. During surgery, adhesion of post-ablation lesions with the strap muscles was observed in six cases, and the cauterization of the strap muscles was seen in five cases. This increased the difficulty of the surgical intervention, as described in previous reports (11,26).
The incomplete treatment of the above cases draws attention to the following aspects. First, thermal ablation should not be recommended for the management of primary PTC patients with clinical suspicious LNM such as cases 4 and 12. According to the recommendation of the 2015 ATA guidelines (15), thyroidectomy plus lymph node dissection is the first-line therapy for PTC with LNM. Thermal ablation treatment for LNM is a “berry picking” approach that is against the principle of cancer therapy in operable patients. Second, as a therapeutic approach for primary PTC in clinical trials or practice, thermal ablation should be selectively used for low-risk patients with intrathyroidal PTC with full patient consent who meet one of the following criteria: (i) refusing surgery, (ii) intolerance of surgery, and (iii) older patients with comorbidities, since PTC has a relatively high incidence of LNM, multifocality, and tumor extension. In this study, LNM was found in 66.7% of patients, and multifocality was present in nine cases (75.0%). Cervical LNM is very common in PTC, but the sensitivity of detection of LNM by US and CT is relatively low (27). In this cohort, the rate of LNM reached 41.7% in patients with clinically negative node status (cN0). The relatively high incidence of LNM in this study may be partially explained by the limited number of cases and selection bias in this cohort, but as reported in a previous study, the rate of LNM in cN0 PTC patients was 11.7–63.8% (28). Therefore, the potential omission of treating metastatic foci in primary PTC limits the indications of thermal ablation. Moreover, the accuracy of US examination for tumor extension is limited in PTC (29), which increases the possibility of residual tumor and ablation injury of perithyroidal tissues if thermal ablation is used for patients with tumor extension. This study shows incomplete ablation in two cases with tumor extension, and especially in case 10, the strap muscles were cauterized, and the recurrent laryngeal nerve was involved. Hoarseness occurred in case 10 after thermal ablation, and laryngoscopic examination confirmed right vocal-cord paralysis. Though PTMC, defined as tumor size ≤1 cm, is one type of low-risk PTC, the rate of LNM reaches 25.9–38.1% in cN0 PTMC patients, as mentioned in a previous study (28). It was found that three PTMC cases in this cohort (cases 1, 3, and 9) had incomplete treatment of the primary tumors and omission of metastatic lymph nodes, and the ablation caused injury of the strap muscles in case 1. Therefore, thermal ablation can be associated with incomplete ablation if it is not used selectively to treat PTMC.
A limitation of the current study is that there was a failure to analyze the surgical outcomes of ablation cases with primary PTC in a randomized controlled pattern. The clinical considerations of increased surgical complexity and difficulty and economic and psychological burden brought by surgery and patient preference determine surgeries cannot be performed on all patients treated with ablation and suspicious findings. Due to the limitations and disadvantages of thermal ablation for treating primary PTC, the 2016 Chinese expert consensus and guidelines for the diagnosis and treatment of PTMC (16) do not recommend thermal ablation as a routine treatment for PTMC. The Chinese expert consensus and guidelines approve that “efficacy of ablation treatment for PTMC in strictly intrathyroidal cases with full patient consent under the operation of qualified professionals still awaits more scientific observations” (16).
This retrospective study demonstrates potential problems associated with thermal ablation of primary PTC such as locally incomplete ablation, incapability of addressing cervical lymph node metastases, and increased difficulties if a surgical approach is necessary for the treatment of post-ablation lesions. Therefore, this study indicates that percutaneous thermal ablation should be recommended with caution in the treatment of operable patients with primary PTC.
Footnotes
Acknowledgments
This study was supported by the Science and Technology Commission of Shanghai Municipality (16411966700) and the National Science Foundation of China (81502317 to W.W., 81472498 and 81772851 to Y.W., and 81572622 to Q.J.).
Author Disclosure Statement
The authors declare that no competing financial interests exist.