
Abstract
Objective:
The aims of this study were to stratify the risk of malignancy in thyroid incidentalomas detected on 18F-fluorodeoxyglucose positron emission tomography with computed tomography (18F-FDG PET/CT) using ultrasound features according to guidelines for thyroid nodules and to develop a subsequent management plan.
Methods:
From a historical cohort of 96,942 consecutive patients who underwent 18F-FDG PET/CT between October 2008 and September 2015, 1342 patients with 1364 nodules underwent ultrasound evaluation for focal uptake in thyroid gland, with a final diagnosis made for 877 patients with 907 nodules, which were included in this study. Ultrasound images were retrospectively reviewed, and they were stratified according to the American Thyroid Association and Korean Thyroid Image Reporting and Data System guidelines. The calculated malignancy risks were compared with the estimated risks suggested by the guidelines.
Results:
The overall malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT was 54.7%. When stratified according to the American Thyroid Association guidelines, the malignancy risks of thyroid incidentalomas with high and intermediate suspicion (93.2% and 45.2%, respectively) were higher than those indicated in the guidelines. The malignancy risks of thyroid incidentalomas with low and very low suspicion (8.1% and 0%, respectively) were within the guideline ranges. These findings were also noted when thyroid incidentalomas were stratified according to the Korean Thyroid Image Reporting and Data System, and in a subgroup of nodules >1 cm.
Conclusions:
Ultrasound examinations can be used to stratify the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT. The risk of malignancy did not increase in thyroid incidentalomas with low and very low suspicion, indicating that only selective biopsies may be needed in these categories of thyroid incidentalomas.
Introduction
18F-
Ultrasound examinations are widely used to assess thyroid nodules and guide biopsies (11,12). Several previous studies have evaluated the utility of ultrasound features for the evaluation of thyroid incidentalomas detected on 18F-FDG PET/CT, demonstrating that the risk of malignancy varies according to the ultrasound features. The risk of malignancy is lower when ultrasound features appear to be benign rather than suspicious (13 –17), which is a similar finding to that for thyroid nodules detected on ultrasound. Several ultrasound risk stratification systems have been developed to assess the malignancy risk and decide on management plans for thyroid nodules (10,18,19). These provide simplified clinically feasible guidelines for the stratification of thyroid nodules according to the risk of malignancy. In these guidelines, thyroid nodules are categorized as high suspicion, intermediate suspicion, low suspicion, or very low suspicion (or benign nodules) of malignancy on the basis of their ultrasound patterns, including the integrated solidity, the echogenicity, and suspicious ultrasound features (10,19). However, for thyroid incidentalomas detected on 18F-FDG PET/CT, the malignancy risk stratification according to ultrasound features has not been fully characterized. Thus, the aim of this study was to use ultrasound features to stratify the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT and thereby suggest management plans.
Methods
This observational study was approved by the Institutional Review Board of the authors' institution, and the requirement for informed consent was waived for data evaluation. Written informed consent for routine thyroid ultrasound and ultrasound-guided biopsy procedures was obtained from all patients before each ultrasound examination. The methods and reporting of results are in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (20). There was no external financial support for this study.
Study population
The study population was obtained from a historical cohort of 96,942 consecutive patients who underwent 18F-FDG PET/CT at the authors' institution between October 2008 and September 2015. The inclusion criteria used to select patients were (i) underwent 18F-FDG PET/CT for workup of non-thyroidal malignancies or diseases, (ii) had an incidentally detected focal uptake in the thyroid gland on 18F-FDG PET/CT, (iii) underwent ultrasound and biopsy, and (iv) had a thyroid nodule as the final diagnosis. Patients were excluded from the study population if they (i) had known thyroid disease, (ii) did not undergo ultrasound and biopsy, (iii) had a thyroid nodule with an indeterminate biopsy result, or (iv) had a thyroid nodule <5 mm (Fig. 1). Finally, 907 thyroid nodules from 877 patients were included in the study population. A final diagnosis of a benign or malignant nodule was made when one of the following criteria was met: (i) confirmation using a surgical specimen or (ii) a conclusive result on FNA or core-needle biopsy (CNB), which was reported based on the Bethesda system for FNA (21) and the “pathology reporting system” as proposed by The Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group for CNB (22). The definition of a conclusive result included Bethesda categories II (benign), V (suspicious for malignancy), and VI (malignancy).
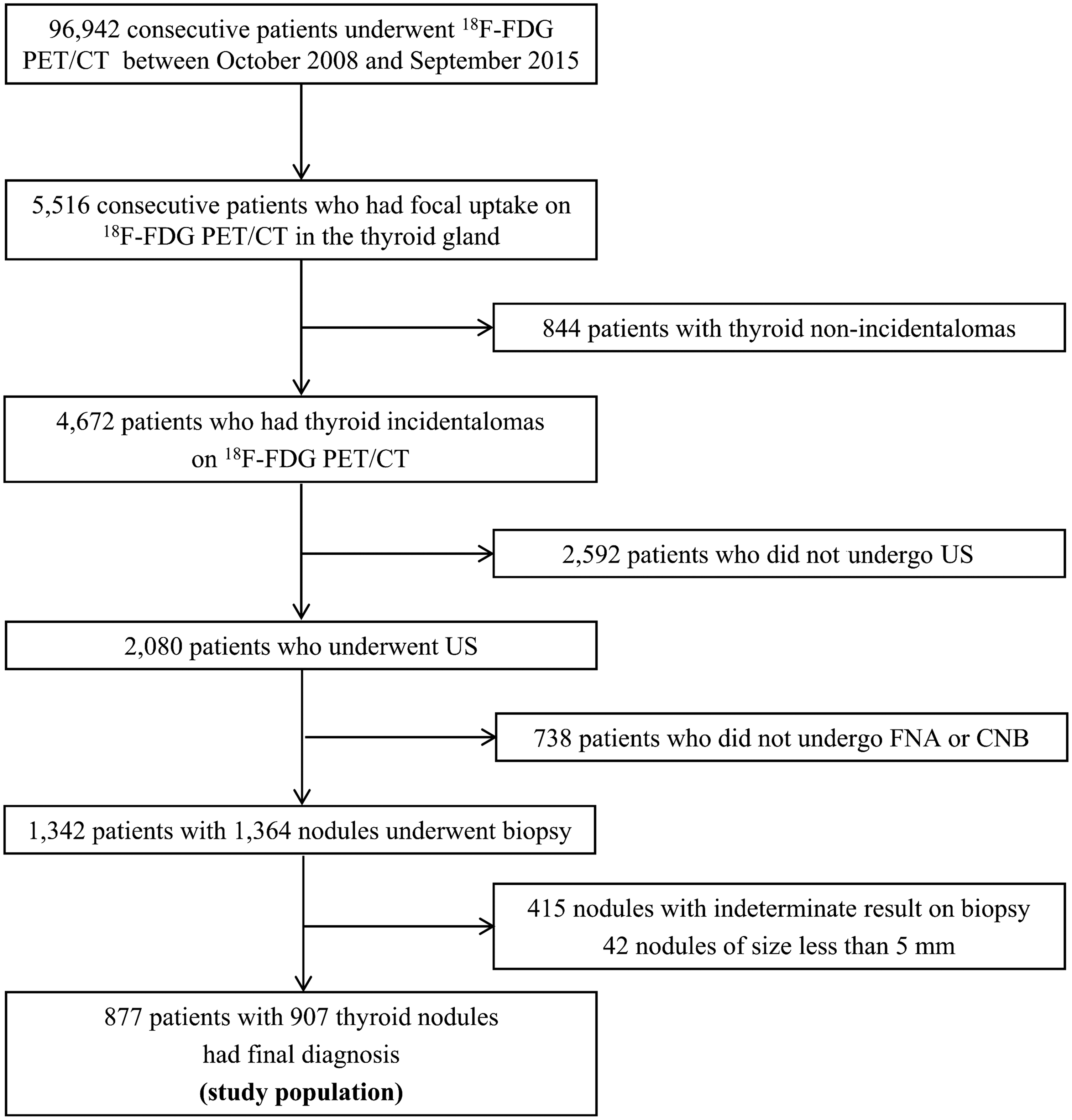
Flow diagram for patient enrollment.
18F-FDG PET/CT acquisition and image analysis
All patients fasted for at least six hours before their 18F-FDG PET/CT examination. Patients were injected with 370–555 MBq of 18F-FDG. Venous blood glucose levels were controlled to ensure that they were <150 mg/dL. Patients were allowed to rest in a sitting or supine position for 60 minutes prior to scanning. Thereafter, PET/CTs were obtained using a Biograph Sensation 16, Biograph Truepoint 40 (Siemens Healthcare, Erlangen, Germany), Discovery STe 8, Discovery 690, Discovery 690 Elite, or Discovery 710 (GE Healthcare, Waukesha, WI) scanner. CT scans were performed first, followed by a PET acquisition from the upper thighs to the skull base. The CT scan parameters were as follows: 120 kVp, Care dose 4D, and a slice thickness of 5 mm for the Biograph Sensation 16 and Biograph Truepoint 40 scanners, and 140 kVp, auto mA, and a slice thickness of 3.75 mm for the Discovery STe 8, Discovery 690, Discovery 690 Elite, and Discovery 710 scanners. No intravenous contrast agent was used. PET images were reconstructed by an iterative algorithm with attenuation correction. Voxel sizes were 3.91 mm × 3.91 mm × 5.0 mm for the Biograph Sensation 16, 2.98 mm × 2.98 mm × 5.0 mm for the Biograph Truepoint 40, 3.91 mm × 3.91 mm × 3.75 mm for the Discovery STe 8, and 2.60 mm × 2.60 mm × 3.75 mm for the Discovery STe 8, Discovery 690, Discovery 690 Elite, and Discovery 710. CT images, attenuation-corrected PET images, and combined PET/CT images were evaluated visually by experienced nuclear medicine board-certified physicians (>10 years of clinical experience) using a dedicated workstation (True D for Siemens; AW for GE Healthcare).
Analysis of the ultrasound findings
The ultrasound images were independently reviewed by two radiologists. Neither reviewer received any information regarding the patients' clinical histories, previous imaging results, or histologic results. Any diagnostic discrepancies between the two reviewers were resolved by consensus. The ultrasound findings of the nodules were evaluated for the following features: size (maximum diameter); composition (solid, partially cystic, or cystic); shape (oval-to-round, irregular, or taller-than-wide); margins (well-defined, ill-defined, or spiculated); echogenicity (hyperechoic, isoechoic, hypoechoic, or marked hypoechoic); presence of echogenic dots suggestive of microcalcifications; and the presence of macrocalcifications. The ultrasound features were used to stratify the malignancy risk of the thyroid incidentalomas detected on 18F-FDG PET/CT into the five categories of the ATA guidelines (high suspicion, intermediate suspicion, low suspicion, very low suspicion, or benign) and the four categories of the Korean Thyroid Image Reporting and Data System (K-TIRADS; high suspicion, intermediate suspicion, low suspicion, or benign; Supplementary Table S1; Supplementary Data are available online at
Outcome measures
The primary study outcomes included the stratification of the malignancy risk of the 18F-FDG PET/CT detected thyroid incidentalomas according to the ATA guidelines and the K-TIRADS for ultrasound features, and comparison of the observed malignancy risks with the estimated malignancy risk presented in the guidelines. The secondary outcome measures included determination of independent predictors for malignancy from the demographic and ultrasound characteristics showing statistical significance.
Statistical analysis
Statistical analysis was performed using SAS software v9.4 (SAS Institute, Cary, NC), with statistical significance being defined as p < 0.05. Continuous variables were expressed as means ± standard deviation (SD), and categorical variables as percentage. A z-test was used to compare the estimated malignancy risks presented in the ATA guidelines and the K-TIRADS with the observed malignancy risks for thyroid incidentalomas detected on 18F-FDG PET/CT. A subgroup analysis of thyroid incidentalomas >1 cm was performed, taking into account the fact that the current guidelines recommends FNA only for nodules >1 cm, even if the nodules are classified as suspicious.
A multivariate logistic regression analysis was performed to determine the independent risk factors associated with malignancy of thyroid incidentalomas detected on 18F-FDG PET/CT. The potential risk factors were age, sex, and ultrasound characteristics, including the nodule size, composition, spongiform nature, shape, margin, echogenicity, and calcifications.
Results
Figure 1 presents a flow diagram for this study. During the study period, 4670 focal thyroid incidentalomas detected on 18F-FDG PET/CT were identified from 96,942 patients, with a prevalence of 4.8%. A final diagnosis was made for 907 thyroid nodules: 411 benign nodules and 496 malignant nodules (453 classic-type papillary thyroid carcinomas, 13 follicular variant papillary thyroid carcinomas, 11 follicular carcinomas, 11 metastases, 5 medullary thyroid carcinomas, and 3 others). The malignancy risk for thyroid incidentalomas was 54.7% (496/907).
Risk stratification of thyroid incidentalomas detected on 18F-FDG PET/CT using ultrasound features
The malignancy risks of thyroid incidentalomas detected on 18F-FDG PET/CT were stratified into the five categories of the ATA guidelines and four categories of the K-TIRADS according to the ultrasound features (Table 1). The overall malignancy risks in the very low suspicion, low suspicion, intermediate suspicion, and high suspicion categories of the ATA guidelines were 0%, 8.1%, 45.2%, and 93.2%, respectively, while for the benign, low suspicion, intermediate suspicion, and high suspicion of the K-TIRADS, they were 0%, 10.1%, 52.1%, and 93.5%, respectively. When these results were compared with the estimated malignancy risks suggested by the ATA guidelines and the K-TIRADS, the malignancy risks of thyroid incidentalomas detected on 18F-FDG PET/CT with intermediate to high suspicion were significantly higher than the estimated malignancy risks suggested by the ATA guidelines and the K-TIRADS (p < 0.0001 for both). However, the malignancy risks for thyroid incidentalomas detected in the low suspicion category and below (the very low suspicion of the ATA guidelines and benign of the K-TIRADS) were within the range of estimated malignancy risks suggested by the ATA guidelines and the K-TIRADS, with no significant differences being found. These findings were also noted when we stratified the thyroid incidentalomas into those >1 cm in diameter (Table 1).
Comparison of the malignancy risks from estimated reference values (ATA and K-TIRADS) and observed values from thyroid incidentalomas detected on 18F-FDG PET/CT.
ATA, American Thyroid Association; 18F-FDG PET/CT, 18F-fluorodeoxyglucose positron emission tomography with computed tomography; K-TIRADS, Korean Thyroid Image Reporting and Data System; NE, not evaluable; NA, not available; CI, confidence interval.
Risk factors for malignancy of thyroid incidentalomas detected on 18F-FDG PET/CT
The results of the univariate and multivariate logistic regression analyses for the risk factors associated with malignancy of the thyroid incidentalomas detected on 18F-FDG PET/CT are listed in Table 2. The ultrasound features associated with malignancy of thyroid incidentalomas detected on 18F-FDG PET/CT were the same as the known suspicious features of thyroid nodules: a taller-than-wide shape, a spiculated margin, hypo- or marked hypoechogenicity, and micro- or macrocalcification (p < 0.05 for all). Additionally, old age (≥ 55 years), male, and small size (<1 cm) were independent risk factors for malignancy of the thyroid incidentalomas.
Macrocalcification including rim calcification.
Discussion
This study used ultrasound features to stratify the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT according to the ATA guidelines and the K-TIRADS. It was found that the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT in the intermediate and high suspicion categories ranged from 45% to 93%, while in the low and very low suspicion categories, the risks ranged from 0% to 10%. When these results were compared with the guidelines, the malignancy risks of thyroid incidentalomas detected on 18F-FDG PET/CT in the intermediate to high suspicion categories were significantly higher than the estimated malignancy risks suggested by the guidelines. However, the thyroid incidentalomas in the low and very low suspicion categories were within the range of malignancy risk suggested by the guidelines. This means that thyroid nodules in these categories did not have an increased risk of malignancy, even though they demonstrated focal 18F-FDG uptake. Given that the ATA guidelines recommend performing FNA for all focal thyroid incidentalomas >1 cm detected on 18F-FDG PET/CT (10), an ultrasound-based risk stratification for thyroid incidentalomas detected on 18F-FDG PET/CT could reduce unnecessary biopsies.
An incidence of focal thyroid incidentalomas detected on 18F-FDG PET/CT of 4.8% was found, with these incidentalomas having a malignancy risk of 54.7%. These values are within the range of incidence (0.2–8.9%) and malignancy risk (8–64%) previously reported (23). The high risk of malignancy suggests that thyroid incidentalomas detected on 18F-FDG PET/CT should be subjected to further diagnostic workup. It is therefore necessary to establish an appropriate diagnostic tool and management plan to evaluate thyroid incidentalomas detected on 18F-FDG PET/CT.
Several ultrasound-based thyroid nodule risk stratification systems have been developed to assess malignancy risk and decide on a management plan (12,18,19,24). This study selected two commonly used thyroid nodule risk stratification systems—the ATA guidelines (24) and the K-TIRADS (19)—and stratified thyroid incidentalomas detected on 18F-FDG PET/CT according to these two guidelines. The results showed that the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT could be stratified effectively according to these guidelines. Furthermore, a multivariate analysis showed that taller-than-wide shape, spiculated margin, hypo- or marked hypoechogenicity, and the presence of micro- or macrocalcifications were identified as significant risk factors for predicting malignancy in thyroid incidentalomas detected on 18F-FDG PET/CT. These ultrasound features are well known as suspicious features for predicting thyroid cancer (10 –12,18,19,24). Thus, the results show that suspicious ultrasound features known to be associated with thyroid cancer are also applicable to thyroid incidentalomas detected on 18F-FDG PET/CT.
The current guidelines for thyroid nodules have not established specific management plans for thyroid incidentalomas detected on 18F-FDG PET/CT. Only the ATA guidelines state that focal uptake within a sonographically confirmed thyroid nodule conveys an increased risk of thyroid cancer, and that FNA is recommended for those nodules ≥1 cm (18,19,24,25). In the present study, the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT in the low or very low suspicion (benign on the K-TIRADS) categories did not show an increase in malignancy (malignancy risk: 0–10%) when compared with the estimated malignancy risks of these categories suggested by the guidelines. The thyroid incidentalomas belonging to these categories accounted for 30–32% of the total ([276–290]/907; the range in the numerators corresponds to the slight differences between the ATA guidelines and the K-TIRADS). Thus, it could be considered unreasonable to perform FNA unconditionally for thyroid incidentalomas belonging to these categories. To reduce unnecessary biopsies, future studies need to determine which thyroid incidentalomas detected on 18F-FDG PET/CT in the low to very low suspicion categories should be biopsied. Contrastingly, thyroid incidentalomas detected on 18F-FDG PET/CT with intermediate to high suspicion showed an increase in malignancy in comparison with the estimated malignancy risks suggested by the guidelines. Therefore, thyroid incidentalomas detected on 18F-FDG PET/CT in intermediate to high suspicion categories should be biopsied.
This study has several limitations. First, the retrospective design and single specialized center study may have led to selection bias. The results might be different in a community hospital. To reduce this selection bias, data from a large population were used. Second, only patients who had a final histological diagnosis were included, which may have overestimated the malignancy risk. A future well-designed prospective multicenter study is needed to validate the current results. Third, the use of CNB histology or FNA cytology as the reference standard allows the possibility of false-negative results. However, these were the methods used in routine clinical practice, and this limitation was unavoidable. Fourth, in clinical practice, sub-centimeter incidentalomas detected on PET/CT are evaluated with ultrasound-guided biopsy only if they have suspicious features on ultrasound, whereas larger (>1 cm) incidentalomas are generally biopsied, regardless of the ultrasound findings. This means that among sub-centimeter thyroid incidentalomas, those nodules with histologic confirmation are likely to have a suspicious feature, which is thought to increase the risk of malignancy. Considering this bias and the current guidelines, additional analysis of those nodules >1 cm in size was performed. Finally, we did not evaluate the maximum standardized uptakes values (SUV), as the data had been acquired on a variety of different PET/CT scanners. The scanners had different manufacturers, manufacturing dates, and specifications, and, accordingly, different imaging protocols. Because the SUV is a semi-quantitative value, it can be affected by several of these factors. Furthermore, differentiating malignant thyroid incidentalomas from benign ones using the SUV is controversial, as the results of previous studies have been inconsistent (23).
In conclusion, the malignancy risk of thyroid incidentalomas detected on 18F-FDG PET/CT was effectively stratified according to the ultrasound features. Thyroid incidentalomas detected on 18F-FDG PET/CT with low or very low suspicion (or benign) showed malignancy risks ranging from 0% to 10%, which were not above the estimated malignancy risk levels suggested in the guidelines. Thus, thyroid incidentalomas detected on 18F-FDG PET/CT with low or very low suspicion (or benign) characteristics, which account for approximately 30% of the total detected, should be biopsied selectively not unconditionally. This could avoid unnecessary biopsies and the potential of associated complications, ultimately leading to an added overall healthcare benefit and significant cost saving.
Footnotes
Author Disclosure Statement
No competing financial interests exist.