
Abstract
Background:
Previous patient studies suggest that thyroid dysfunction affects volumes of particular regions of the brain. So far, population-based data related to this topic are lacking. The aim of this study was to investigate associations of serum levels of thyrotropin (TSH), free triiodothyronine, and free thyroxine (fT4) with total brain volume, gray matter volume, white matter volume (WMV), and hippocampal volume (HV) in a population-based study.
Methods:
Data on 2557 individuals were pooled from two independent population-based surveys of the Study of Health in Pomerania conducted in Northeast Germany. Brain volumes were determined from images derived from 1.5 T magnetic resonance imaging. Low and high TSH were defined using the cutoffs 0.40 and 3.29 mIU/L, respectively. Associations between thyroid hormone levels and segmented brain volumes were analyzed by linear regression models. Further, voxel-based morphometry was conducted to search for associations with thyroid hormone levels in a hypothesis-free way throughout the whole brain. All models were adjusted for confounders.
Results:
Only 9/70 individuals with high TSH had low free triiodothyronine or fT4 levels. Individuals with high TSH had significantly lower total brain volume (β = −26.9 [confidence interval (CI) −49.0 to −4.8]; p = 0.017), WMV (β = −16.1 [CI −29.4 to −2.7]; p = 0.018), and HV (β = −223 [CI −395 to −50]; p = 0.011) than individuals with TSH within the reference range, while low TSH was not significantly associated with any of the brain volumes. Voxel-based morphometry analyses revealed a significant positive association with serum fT4 levels in the left middle frontal gyrus.
Conclusions:
In conclusion, the results of this study indicate that the subclinical hypothyroid state may lead to a reduced brain volume affecting particularly HV in younger subjects and WMV, which might correspond to subtle microstructural changes in white matter fiber tracts or myelination of the axones. Gray matter seems not to be affected by subclinical hypothyroid states.
Introduction
I
So far, the association between thyroid dysfunction and brain volumes has only been investigated in small patient studies, and it is debatable whether these findings can be extended to the general population. Against this background, this study aimed to investigate whether high thyrotropin (TSH) levels are associated with lower GMV, WMV, and HV in data derived from two population-based studies conducted in northeast Germany. Brain volume parameters were derived from brain magnetic resonance imaging (MRI). In the analyses, two approaches were followed. The first approach looked at whether thyroid hormone levels were associated with total GMV, WMV, and HV, while in the second approach, VBM analyses were performed to investigate potential associations of thyroid biomarkers with local GMV in a hypothesis-free approach.
Methods
General population sample
Data from the population-based Study of Health in Pomerania (SHIP) were analyzed (13 –15). The target population of the first cohort was comprised of adult German residents in northeast Germany living in three cities and 29 communities with a total population of 212,157. A two-stage stratified cluster sample of adults with German citizenship aged 20–79 years (baseline) was randomly drawn from local registries. The net sample (without migrated or deceased persons) comprised 6267 eligible subjects, of whom 4308 Caucasian subjects participated at baseline SHIP-0 between 1997 and 2001. The follow-up examination (SHIP-1) was conducted five years after baseline and included 3300 subjects. From 2008 to 2012, the third phase of data collection (SHIP-2; N = 2333) was carried out. In this study, an association of diagnosed hypothyroidism with depression and anxiety was previously demonstrated (6). Concurrent with SHIP-2, a second sample called SHIP-Trend-0 (N = 4420) was drawn from the same area in 2008, and similar examinations were undertaken.
Subjects from SHIP-2 and SHIP-Trend-0 were asked to participate in a whole-body MRI assessment (16,17). After exclusion of subjects who refused participation or who fulfilled exclusion criteria for MRI (e.g., cardiac pacemaker), 1163 subjects from SHIP-2 and 2154 subjects from SHIP-Trend-0 underwent MRI scanning (N = 3317; Fig. 1). SHIP and SHIP-Trend were approved by the local ethics committee. Informed written consent was obtained from all participants.
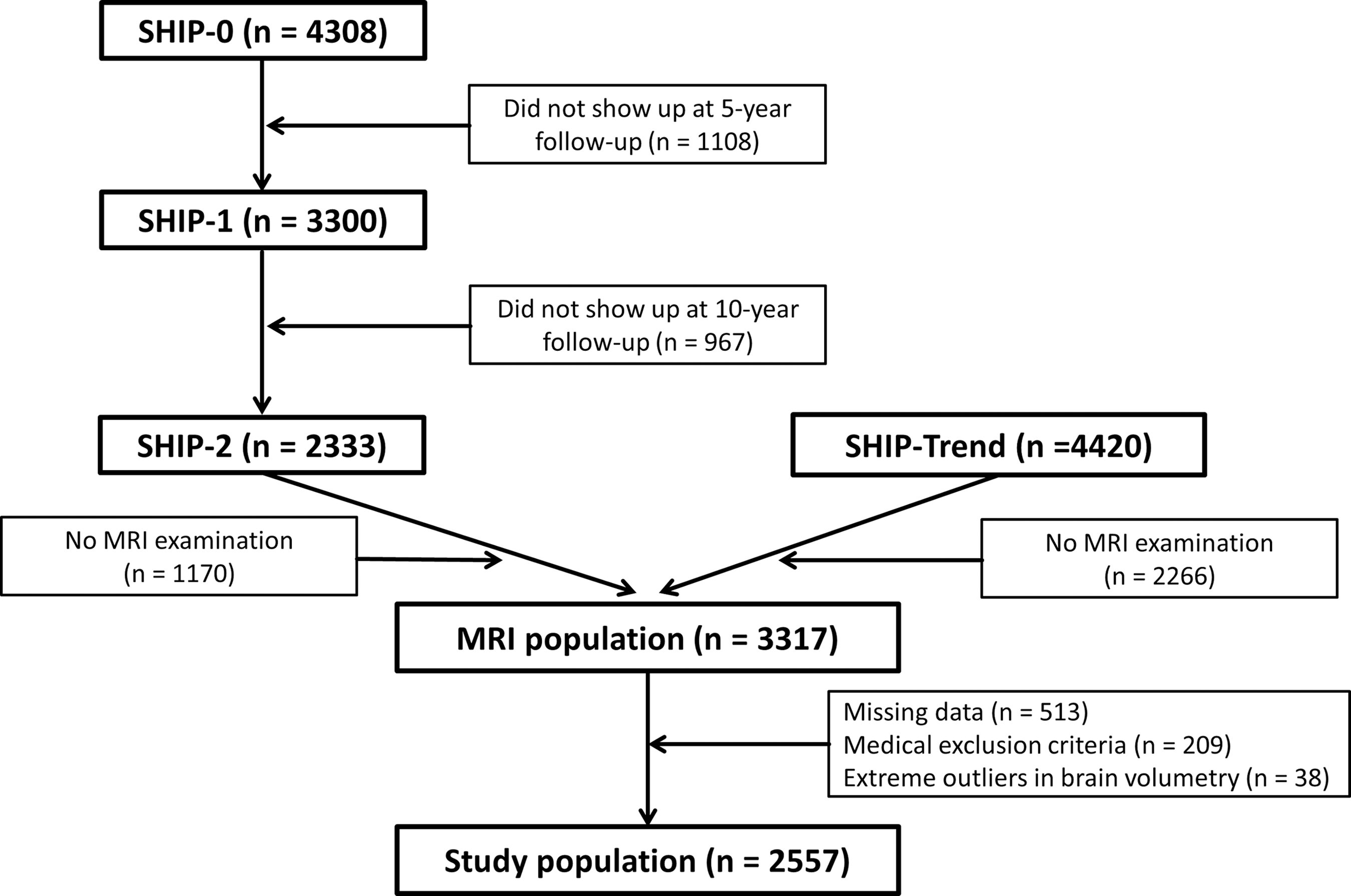
Consort diagram.
Complete data sets, including thyroid levels, education, body mass index (BMI), alcohol consumption, smoking habits, and marital status, were available from 2884 subjects. After exclusion of medical conditions (e.g., a history of cerebral tumor, stroke, Parkinson disease, multiple sclerosis, epilepsy, hydrocephalus, enlarged ventricles, or pathological lesions) or technical reasons (e.g., severe movement artifacts or inhomogeneity of the magnetic field), 2595 subjects were available (Fig. 1). Based on the homogeneity check of the CAT12 toolbox (developed by Christian Gaser, University of Jena, Germany;
Assessments
All images were obtained using a 1.5 T Siemens MRI scanner (Magnetom Avanto; Siemens Medical Systems, Erlangen, Germany) with a T1-weighted magnetization prepared rapid acquisition gradient echo (MPRAGE) sequence and the following parameters: axial plane, TR = 1900 ms, TE = 3.4 ms, and flip angle = 15°, with an original resolution of 1.0 mm × 1.0 mm × 1.0 mm. The HV, GMV, and WMV were determined within the recon-all pipeline of FreeSurfer 5.1. Mean HV was defined as the mean volume of the left and the right hemisphere. TBV was defined as the sum of GMV and WMV.
For the VBM, the images were preprocessed with SPM12 (Wellcome Trust Centre for Neuroimaging, University College London, London, United Kingdom) and the CAT12 toolbox (developed by Christian Gaser, University of Jena, Germany;
Non-fasting blood samples were taken between 7:00am and 4:00pm. Serum TSH, free triiodothyronine (fT3), and fT4 concentrations were analyzed in the central laboratory of the University Medicine Greifswald by a homogeneous, sequential, chemiluminescent immunoassay based on LOCI® technology (Dimension Vista® System Flex® reagent cartridge; Siemens Healthcare Diagnostics Inc., Newark, DE). The analytical measuring range was 0.005–100 mIU/mL, 0.1–8.0 ng/dL, and 0.50–30.00 pg/mL for TSH, fT4, and fT3, respectively. Low and high serum TSH concentrations were defined using the cutoffs 0.49 and 3.29 mIU/L, respectively, which were recently established for the study region (18).
Smoking status, alcohol consumption, and educational status were assessed by computer-assisted personal interviews. Smokers were categorized into three categories: lifetime nonsmokers, former smokers, and current smokers. Alcohol consumption was evaluated as beverage-specific alcohol consumption (beer, wine, and distilled spirits) on the last month preceding the examination, and the mean daily alcohol consumption was calculated using beverage-specific pure ethanol volume proportions (19). Education was categorized according to the German three-level school system: low, <10 years; intermediate, 10 years; and high, >10 years. Height and weight were measured for the calculation of the BMI, being weight (kg)/height2 (m2).
Statistical methods
All results are reported as pooled data of SHIP-Trend-0 and SHIP-2. Stratified by thyroid function status, continuous data are expressed as median and 25th and 75th percentile, and categorical data as absolute numbers and percentages. The association between thyroid hormone tests and brain volumes were analyzed by linear regression models adjusted for age, sex, BMI, alcohol consumption, smoking status, education, and time of blood sampling. Continuous exposure variables (TSH, fT3, fT4) were power transformed to reduce the effect of outliers on the results (20). Multivariable fractional polynomials were tested to account for potential nonlinear associations of exposure or confounders with the outcome. Interactions of thyroid hormones with age and sex were tested for all outcomes. Inverse probability weights were applied to consider dropouts of individuals between SHIP-0 and SHIP-2 and between the basic and the MRI examinations. The intention behind these weights is to weight up the impact of individuals from groups who are more likely to drop out of the study and to weight down the impact of individuals from groups who are less likely to drop out in the regression analyses. To calculate these weights, logistic regression models were used, with participation at the MRI examination as outcome and sociodemographic, behavioral, and cardiovascular risk factors from the core examinations as explanatory variables. Additionally, for SHIP-2 participants, weights were computed for the dropout from SHIP-0 to SHIP-2, and these weights were multiplicatively combined with the MRI weights. This approach aimed to improve the representativeness of the analyses. A p-value of <0.05 was considered as statistically significant. All analyses were performed with Stata v14.1 (Stata Corp., College Station, TX).
For VBM analysis, SPM12 was used to analyze the preprocessed GM segments in three separate regression analyses between GM volume and the power-transformed levels of TSH, fT3, and fT4 adjusted for age, sex, education, BMI, alcohol consumption, smoking habits, marital status, and intracranial volume as covariates in all models. In a VBM analysis, a single statistical test is carried in each voxel of the brain. To take into account multiple testing, family-wise error (FWE) corrected peak-level p-values with a threshold of 0.05 to reach significance were used.
Results
Of the 2557 individuals in the study population, there were 229 with low TSH (47 with high fT3 or fT4) and 70 with high TSH (9 with low fT3 or fT4). There were only two individuals with TSH levels >10 mIU/L. Individuals with low TSH were in median older, more often former smokers, less educated, and reported more often a less good or bad general health than individuals with serum TSH levels within the reference range (Table 1). Median brain volumes differed only slightly between individuals with low TSH and individuals with TSH within the reference range. Individuals with high TSH were more often females, had a lower BMI, smoked more often, and reported more often a less good or bad general health than individuals with serum TSH levels within the reference range. Median brain volumes were lower in individuals with high TSH than in individuals with TSH within the reference range.
Continuous data are expressed as median and 25th and 75th percentile; categorical data are expressed as absolute numbers and percentages.
TSH, thyrotropin; fT3, free triiodothyronine; fT4, free thyroxine.
In multivariable linear regression models adjusted for confounders, serum TSH levels were inversely associated with TBV, WMV, and left HV (Table 2 and Fig. 2). Individuals with high TSH had significantly lower TBV, WMV as well as mean, right, and left HV than individuals with normal TSH. Individuals with low TSH had a significantly lower left HV than individuals with serum TSH levels within the reference range. No further significant associations were observed of low TSH with any of the brain volumes. Likewise, neither serum fT3 nor serum fT4 levels were significantly associated with TBV, GMV, WMV, or HV. All the observed significant association were confirmed after excluding individuals with high TSH but low fT3 or fT4 and individuals with low TSH but high fT3 or fT4.

Association between serum thyrotropin (TSH) levels and brain volumes adjusted for confounders.
Data are expressed as β coefficients and confidence intervals derived from a linear regression adjusted for age, sex, body mass index, smoking status, alcohol consumption, education, and time of blood sampling. Continuous values of TSH, fT3, and fT4 were power transformed to minimize the effect of outliers. Mean hippocampal (HC) volume was calculated as the sum of right and left hippocampal volume.
In comparison to TSH within the reference range.
p < 0.05.
For the outcomes TBV, GMV, and WMV, no significant interactions of TSH were detected with age (TBV, p = 0.664; GMV, p = 0.757; WMV, p = 0.653) or sex (TBV, p = 0.965; GMV, p = 0.603; WMV, p = 0.716), but there was a significant interaction of TSH with age (p = 0.055) but not with sex (p = 0.440) for mean HV. TSH was significantly associated with mean HV for individuals <50 years of age but not for individuals ≥50 years of age (Fig. 3). For right and left HV, similar effects were observed than for mean HV (right HV, p = 0.066; left HV, p = 0.064). For all outcomes, no significant interaction was observed of TSH with current smoking (TBV, p = 0.639; GMV, p = 0.246; WMV, p = 0.748; HV, p = 0.120) or thyroid medication (TBV, p = 0.509; GMV, p = 0.360; WMV, p = 0.724; HV, p = 0.777).
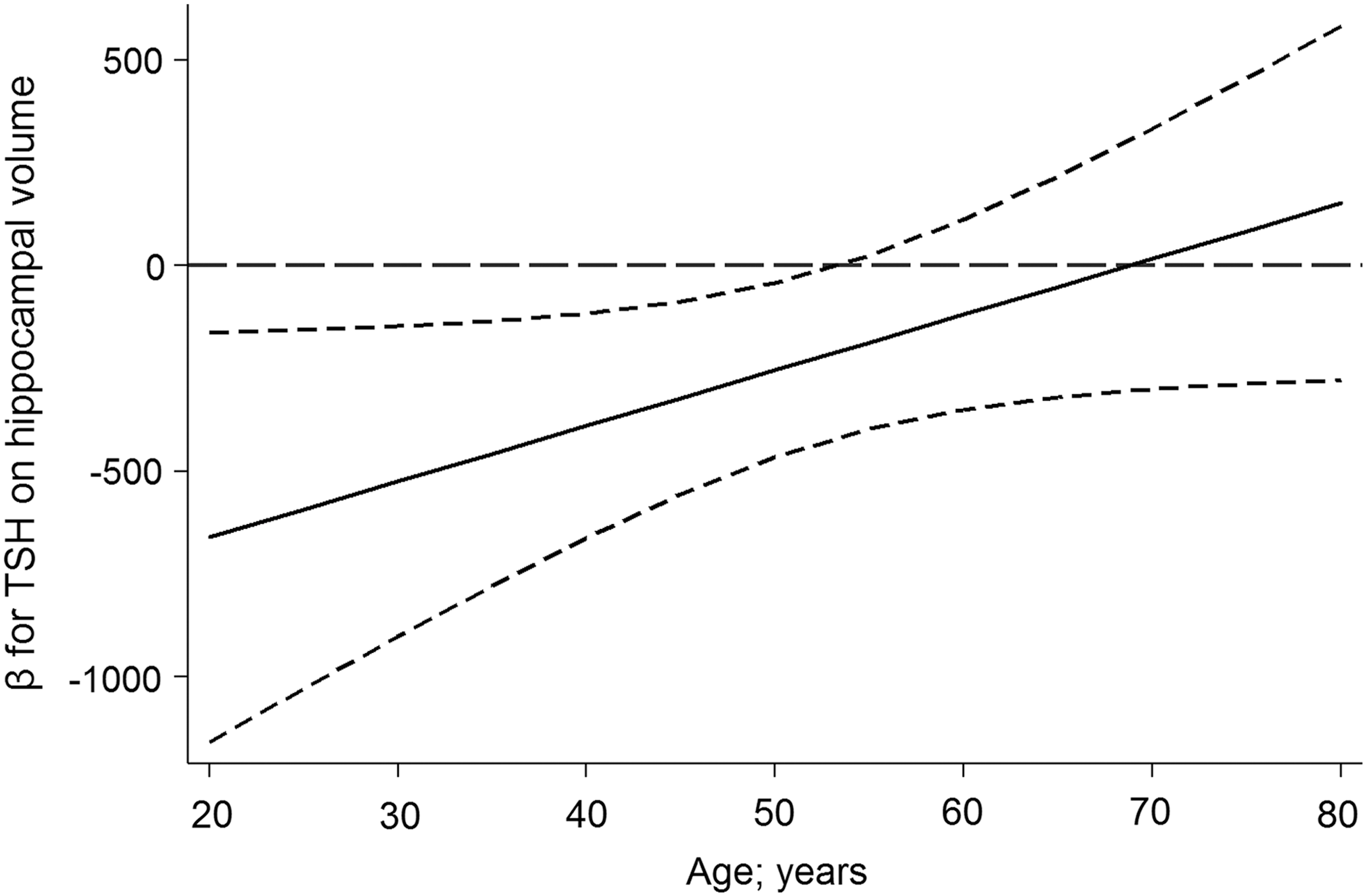
Association between serum TSH levels and hippocampal volume for different ages.
In the VBM analyses, a cluster of five voxels was detected in the left middle frontal gyrus that is significantly positive associated with serum fT4 (p = 0.026; MNI [−42, 24, 42]). The corresponding VBM without the subjects with a thyroid medication showed an even stronger effect in this region (p = 0.007; MNI [−42, 24, 42], 29 voxels). No further significant associations of TSH or fT3 were found in the VBM analyses. Since the significant cluster is part of the Brodmann area 9 (BA9), the GM volume of BA9 was extracted from the CAT12 GM segmentations of the MRI scans. The BA9 volume correlated significantly with the HV (R 2 = 0.39). A significant inverse association of serum TSH levels was found with overall BA9 volume (p = 0.032), whereas serum fT3 (p = 0.888) or fT4 (p = 0.637) levels were not significantly associated with overall BA9 volume.
Discussion
In a population-based cross-sectional sample, inverse associations of serum TSH levels with TBV, WMV and HV, but not with GMV, are demonstrated. Particularly, high TSH levels were associated with a decrease in brain volumes. In contrast, no significant associations of fT3 or fT4 levels were detected with any of the brain volumes. While no significant association of thyroid hormone levels was observed with overall GMV, VBM analyses revealed a positive association of fT4 with a region in the left middle frontal gyrus, which is located in BA9.
These findings are in partial agreement with a patient study in 11 hypothyroid adults and nine age-matched controls, in which right but not left HV was significantly decreased in hypothyroidism (12). The lack of a significant association for left HV in the adult study may be explained by low statistical power (12). In another study, congenital hypothyroidism was significantly associated with right and left HV in children and adolescents (11). In a further study, HV was significantly lower in 24 children aged 9–12 years delivered from mothers with hypothyroidism during pregnancy than in 30 controls delivered from mothers without hypothyroidism during pregnancy (21). In the present study, high TSH was inversely associated with both right and left HV, but the study failed to demonstrate significant associations of serum fT3 or fT4 levels with HV. This might be related to the fact that out of the 70 individuals with high TSH, only nine had low fT3 or fT4 levels. After excluding these nine individuals, the association between high TSH and HV remained statistically significant, suggesting that not only overt but also subclinical hypothyroidism is associated with a reduced HV.
There are several potential mechanisms explaining an association of hypothyroidism with a reduced HV. First, the hippocampus may be an important target region for thyroid hormones because the density of thyroid hormone receptors in the hippocampus is high (22,23). Thus, a lack of thyroid hormones may lead to an inadequate supply of the hippocampus with T3 or T4. Second, animal experiments suggest that adult-onset hypothyroidism affects the pyramidal cells of the hippocampus (24 –26). These studies demonstrated that in hypothyroidism the volume of the pyramidal cell layer in the hippocampal CA3 region is decreased because of an altered neuronal packing (24 –26). Likewise, it has been reported that hypothyroidism reduces the total number of pyramidal cells in the hippocampal CA1 region (24). Furthermore, it has been proposed that hypothyroidism at a younger age may permanently change hippocampal function and in consequence HV (27), which fits well with the present finding of a significant inverse association between TSH and HV mainly for those aged <50 years.
In this study, inverse associations were observed of serum TSH levels not only with HV but also with BA9 volume, suggesting that hypothyroidism may result in cognitive impairment. BA9 is involved in short-term memory (28) and correlates with the hippocampus. In agreement with these findings, two smaller studies conducted in 81 (29) and 337 (30) elderly individuals demonstrated associations of subclinical hypothyroidism with cognitive impairment. The majority of studies, however, failed to substantiate significant associations of subclinical hypothyroidism (31 –33) or serum TSH levels (34,35) with cognitive impairment in population-based data from individuals aged ≥65 years. Results from the Rotterdam Study demonstrated that higher TSH is associated with a lower dementia risk in both the full and the normal range of thyroid function (5). In line with this, that study reported a positive association between serum TSH levels and better global cognitive scores. However, thyroid function was not related to subclinical vascular brain disease derived from MRI, which suggested nonvascular pathways leading to dementia.
In the present analyses, a significant inverse association was observed between high TSH and WMV but no association with overall or region-specific GMV. It might be important to acknowledge that the study largely investigated subjects with subclinical thyroid conditions only. The results do not point to large brain changes, and in fact, the effects on HV were only relevant in younger subjects (<50 years). It is unclear how the association with WMV can be explained. Although white matter hyperintensities were did not analyzed as a correlate of microvascular damage, the study by Chaker et al. found no sign of any association between thyroid function and vascular parameters in 9446 subjects (5). However, Singh et al. detected microstructural changes in the white matter fiber tracts of hypothyroid patients compared to controls in their diffusion tensor tractography study (36). These changes could in part explain the findings of reduced WMV in subclinical hypothyroidism.
In contrast to the current results, Chaker et al. found no significant association between serum TSH levels and TBV or GMV in data from 4683 individuals aged ≥45 years (7). However, they observed that individuals aged 45–70 years with low fT4 levels had lower TBV and WMV than individuals with normal fT4 levels, which somewhat indicates that the hypothyroid state may be associated with reduced brain volumes. In that study, serum fT4 levels were inversely associated with TBV and WMV in individuals >80 years of age (7), an association that points in the opposite direction than in younger individuals of that study. The authors explain their findings by better white matter integrity in younger than in older persons. In this study, no age-dependency of the associations was observed, which may be related to the fact that the study included only eight individuals >80 years.
The present findings are in partial agreement with a small patient study in which 10 untreated hypothyroid patients had significantly lower WMV in the cerebellum, right precentral gyrus, right inferior and middle frontal gyrus, right inferior occipital gyrus, and right inferior temporal gyrus, and significantly lower GMV in the cerebellum and left postcentral gyrus than 10 controls (9). In agreement with the current findings, a study with 25 hypothyroid patients with Hashimoto thyroiditis on levothyroxine treatment did not show any differences in GMV compared to 27 controls (37), indicating that levothyroxine treatment may protect against hypothyroidism-induced vulnerability of the brain. A study with 1047 participants aged >64 years showed that hypothyroidism was associated with lower performance in the mini mental status (38). In that study, half of the hypothyroid participants were unaware of their condition and not treated by thyroid medication. From those findings, it can be concluded that elderly patients with impairment in cognition should be screened for hypothyroidism (38), but to decide on potential therapeutically consequences, randomized controlled trials are needed.
While inverse associations of serum TSH levels were observed with total HV, no significant clusters of the HV were detected in the whole brain VBM analyses of TSH. In the VBM analysis, all p-values are FWE-corrected because of multiple voxel-based comparisons. Thus, VBM-analyses have a lower statistical power than targeted single region volume analyses. Therefore, only large and regionally homogenous clusters or highly significant peak voxels can be discovered in VBM analyses.
To the best of the authors' knowledge, this is the first population-based study associating thyroid hormone levels with brain volumes. Strengths of this study are the large number of individuals investigated and the assessment of brain volumes with gold-standard methods. A limitation is the cross-sectional design of this study allowing no causative conclusions. Furthermore, the range of blood sampling time was eight hours, from 8:00am to 4:00pm. It has been described that thyroid hormones are prone to diurnal variations (39). Therefore, a sensitivity analysis was performed, adjusting additionally for time of blood sampling, which did not change the results significantly. Another limitation of the study is that the onset time of altered thyroid function is unknown. Likewise, no information was available on the intake of “harder” drugs such as heroin or cocaine, but it is believed that the number of individuals taking such drugs was very low in this study. To account for nonparticipation at the MRI examinations, inverse probability weighting was introduced, assuming a “missing at random” mechanism. This means that that the dropout is not completely at random but can be explained by available data. However, a potential selection bias due to a “missing not at random” mechanism cannot be totally ruled out, which means that the dropout is not completely explainable by existing data.
In conclusion, the results of this study indicate that the subclinical hypothyroid state may lead to a reduced brain volume affecting particularly HV in younger subjects and WMV, which might correspond to subtle microstructural changes in white matter fiber tracts or myelination of the axons. GM seems not to be affected by subclinical hypothyroid states. Longitudinal studies are needed to understand better the interaction with age-related parameters and the putative clinical impact of dysregulated thyroid function on brain-related disorders.
Footnotes
Acknowledgments
The Study of Health in Pomerania is part of the Community Medicine Research Network of the University Medicine Greifswald, which was funded by the German Federal Ministry for Education and Research, the Ministry for Education, Research and Cultural Affairs, and the Ministry for Social Affairs of the State Mecklenburg-West Pomerania. MRI scans in SHIP and SHIP-TREND have been supported by a joint grant from Siemens Healthineers, Erlangen, Germany, and the Federal State of Mecklenburg-West Pomerania. The project has received funding from the European Union's Horizon 2020 research and innovation program under grant agreement number 634453.
Author Disclosure Statement
H.J.G. has received speaker's honoraria and travel grants from Fresenius Medical care and Janssen. No other competing financial interests exist.