
Abstract
An individual with familial dysalbuminemic hyperthyroxinemia (FDH) due to a homozygous mutation (c.653G>A, p.R218H) in the human serum albumin (HSA) gene is reported. The patient was identified during evaluation of abnormal thyroid tests in a large family with multiple levels of consanguinity. He showed a greater increase in total thyroxine (T4) relative to that observed in heterozygous family members. The higher affinity of mutant HSA for T4, together with the large molar excess of HSA relative to thyroid hormones in serum, results in preferential association of T4 with the mutant rather than wild-type HSA in heterozygous individuals. The twofold greater amount of T4 bound to the mutant HSA in the homozygote, relative to heterozygotes, is an adaptive requirement to maintain a normal free T4 concentration.
Introduction
F
Patients
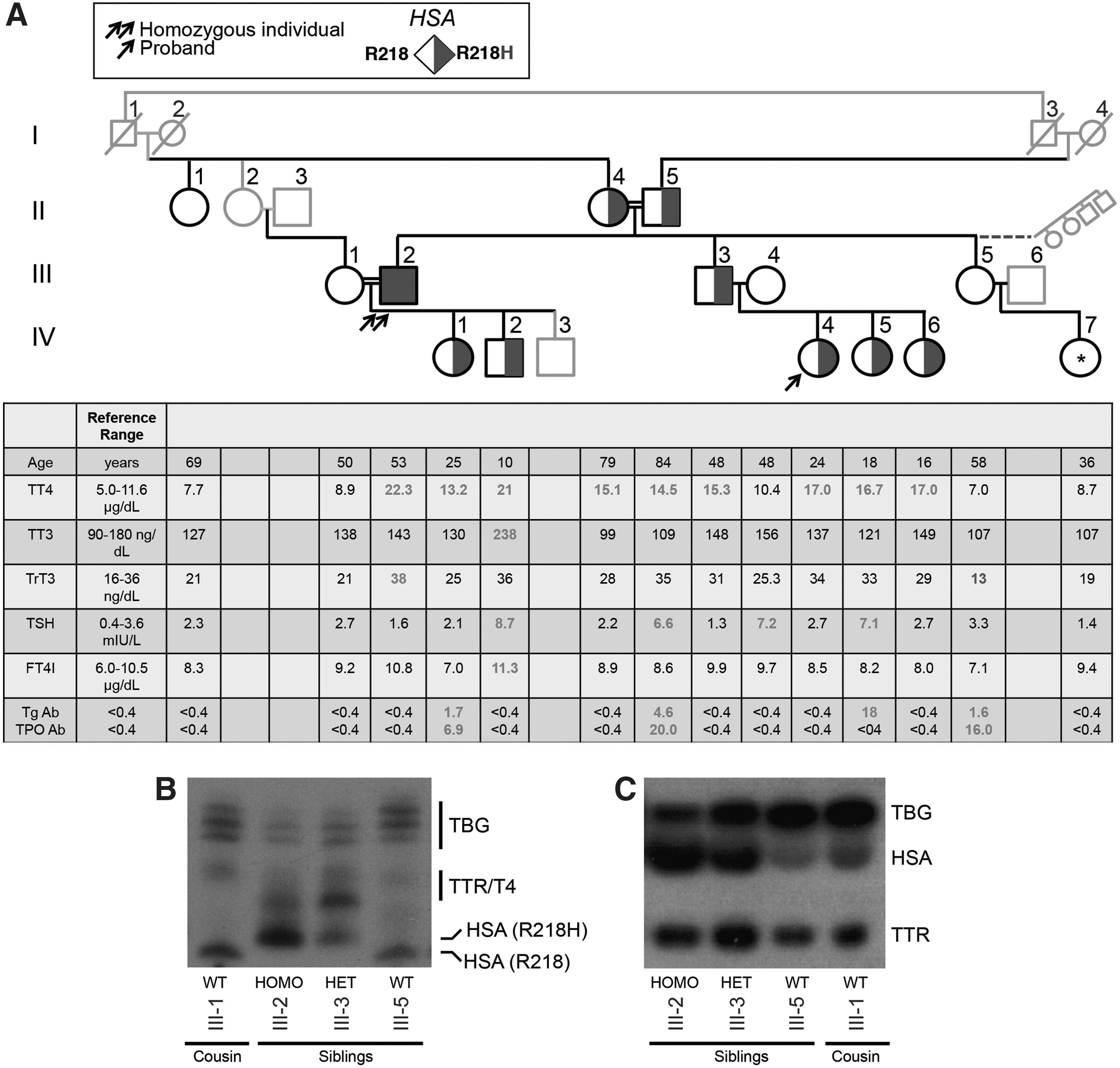
The homozygous individual was an uncle of the proband, a 23-year-old woman who presented to one of the authors (A.K.) for evaluation of hirsutism. She was otherwise asymptomatic. Thyroid tests showed a high free thyroxine (T4) of 2.82 ng/mL (reference range [RR] 0.58–1.25 ng/mL) and triiodothyronine (T3) of 5.36 pg/mL (RR 2.3–4.2 pg/mL), with a normal thyrotropin (TSH) of 2.1 mIU/L (RR 0.4–4.0 mIU/L), raising suspicion for resistance to thyroid hormone beta (RTH-β).
Results
Written consent was obtained in accordance with an Institutional Review Board–approved protocol. As shown in Figure 1A, 9/14 relatives tested had elevated serum total T4 (TT4) with normal free T4 index (FT4I) and total T3 (TT3), except individual IV-2. These results, in the presence of non-suppressed TSH, suggested FDH. Four individuals (II-5, III-4, IV-2, and IV-5) had mildly elevated TSH consistent with subclinical hypothyroidism, and two (II-5 and IV-5) had positive thyroid autoantibodies. Individual IV-2, a 10-year-old boy with obesity, had FT4I and TT3 at 8% and 32% above the adult reference range, respectively (Fig. 1A), consistent with RTH-β. However, sequencing of exons 7–10 of THRB was negative for a mutation.
(
Sequencing of DNA from peripheral leukocytes revealed a mutation in the HSA gene (c.653G>A; Fig. 2A), resulting in substitution of the normal arginine-218 with histidine (p.R218H) in the nine hyperthyroxinemic family members. Interestingly, individual III-2, born to heterozygous parents, was homozygous for the R218H mutation (Fig. 2A). His TT4 was 37% and 161% above the mean TT4 of heterozygous and wild-type (WT) family members, respectively (Fig. 2B). Isoelectric focusing (IEF) of this individual's serum, visualized with radiolabeled T4, identified the mutant HSA protein (Fig. 1B, lane 2). Notably, labeled T4 bound the mutant protein to the exclusion of WT HSA present in sera of a heterozygous sibling (Fig. 1B, lane 3).

(
Non-denaturing polyacrylamide gel electrophoresis of sera from individuals of each genotype with radiolabeled T4 was performed, as described in the legend to Figure 2, to determine the proportion of T4 bound to the three T4-binding serum proteins (Fig. 1C). The effect of sample preparation on the relative distribution of T4 among the T4-binding proteins was determined by applying different amounts of 125I-labeled T4 to a WT serum (Fig. 3A), and by serial dilutions of sera from a WT and homozygous mutant individual (Fig. 3B). Measures varied by <15%, and the ratio of percent T4-bound to the mutant versus WT HSA ranged from 1.9 to 2.3. Quantification revealed that while the percent of transthyretin (TTR)-bound T4 is stable across genotypes, there is a stepwise increase in the percent of T4 bound to HSA in the WT (average 20%), heterozygous (36.4%), and homozygous (47.9%) individuals, and a concomitant reduction in T4-bound T4-binding globulin (TBG; Fig. 2C). Serum HSA and TBG were measured and used to estimate the relative quantity of T4 bound to each protein. Binding to HSA was six- and threefold higher in the homozygote and heterozygote relative to the WT. In contrast, the amount of T4 bound per milligram of TBG was similar in all genotypes (Table in Fig. 2C, rows 4 and 5).

Radioautographs and quantification of relative T4 associated with TBG, HSA, and TTR separated by non-denaturing PAGE in serum from (
Discussion
FDH is a well-characterized condition, producing abnormal thyroid tests in euthyroid individuals (1 –4). The R218H mutation was first identified in a large Amish kindred (5) and is the most common of five HSA variants causing FDH (1). Substitution of R218 for a smaller residue electrostatically stabilizes the T4-binding site and thereby promotes increased affinity for T4 (6). Individuals with R218H have elevated serum TT4 and, to a lesser degree, reverse T3 due to increased mutant HSA binding affinity for these iodothyronines, but normal dialyzable free T4 and a non-suppressed TSH. Mutant HSA can interfere with indirect methods of measuring free T4 and T3, producing falsely elevated values (7), leading to inappropriate treatment and explaining the elevated free T4 and T3 levels in the proband at presentation.
To the authors' knowledge, this is the first report of a biallelic HSA mutation causing FDH. As HSA is present in 6000-fold molar excess relative to T4, T4 binds exclusively to mutant HSA, as shown by IEF, despite representing only half the total HSA in heterozygotes. Quantification of the T4 bound to HSA showed that the homozygote had a twofold increase in T4 binding per gram of HSA compared with heterozygotes (Fig. 2C), including subject IV-2 (1.3 μg T4/g HSA). Thus, biallelic expression of the mutant HSA requires twice the amount of bound T4 to maintain a normal free T4.
Footnotes
Acknowledgments
This study was supported in part by grants from the National Institutes of Health, R37DK15070 to S.R. and R01DK110322 to A.M.D. M.S.M. was supported by a Ruth L. Kirschstein National Research Service Award for Individual Postdoctoral Fellows T32DK007011. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Diabetes and Digestive and Kidney Diseases or the National Institutes of Health. The authors wish to thank Quest Diagnostics for performing serum quantification of TBG and HSA. Thanks are due to Miles Tracy for the determination of thyroid tests and to Prof. Roy E. Weiss for useful discussion. A.K. acknowledges Dr. Isilay Taskaldiran for the referral of the proband and her mentor Prof. Dr. Nese Ersoz Gulcelik for advice.
Author Disclosure Statement
M.S.M. declares that her spouse receives salary and stock from AbbVie, Inc. The authors declare no competing financial interests exist.