
Abstract
Background:
The effects of active and passive smoking on thyroid function in the Korean population have not been determined. Furthermore, related research is based on self-reported smoking status, which may be inaccurate, especially among women. The present study aimed at evaluating the association between biochemically verified smoking status and thyroid function in a nationally representative Korean population.
Methods:
This population-based cross-sectional study included 3404 subjects without thyroid disease who were not taking thyroid medication. Smoking status was identified using self-reported data and urinary cotinine levels. Kruskal–Wallis and Jonckheere–Terpstra trend tests were performed to evaluate the association between smoking exposure and thyroid function. Multivariate logistic regression analysis was used to estimate the effect of smoking on subclinical hypothyroidism (SCH).
Results:
Biochemically verified active and passive smoking rates were 43.4% and 23.3% among men and 10.0% and 22.9% among women, respectively. Active smokers had significantly lower iodine levels than passive smokers and nonsmokers. Active smoking was associated with decreased serum thyrotropin (TSH) levels among both sexes, although only men exhibited a dose–response relationship between increasing smoking exposure and decreasing TSH levels. Passive smoking slightly decreased TSH levels, but the decrease was not statistically significant. The risk of SCH decreased with increasing smoking exposure in the multivariate-adjusted analysis (p for trend = 0.027 among men and 0.042 among women).
Conclusions:
Active and passive smoking were associated with decreasing serum TSH levels and a lower risk of SCH in a Korean population. These associations might be related to lower urinary iodine levels in active smokers.
Introduction
T
The major challenge in determining subjects' smoking status, especially in Asian countries, is the reliance on self-reported smoking data that are obtained using self-administered questionnaires or face-to-face interviews because these data can have substantial discrepancies compared to objectively determined smoking status (17 –19). This discrepancy is especially prominent among women. For example, the ratio between cotinine-verified smoking status and self-reported smoking status was 1.12 for Korean men (44.7% vs. 50.0%), but the gap was substantially higher among women (ratio: 2.36; 5.9% vs. 13.9%) (17). Although the issue of misclassification of smoking status should be addressed in study design and analysis, few studies on the effects of tobacco exposure on thyroid function have considered this issue.
Most studies have focused on the association between active smoking and thyroid function, and the target populations were primarily Caucasians who resided in areas with different iodine intakes (12,15,20). Therefore, there is a gap in knowledge regarding the influence of active and passive smoking on the thyroid gland, compared to non-smoking status, among Asian individuals from iodine-sufficient areas. Although two studies have examined the effects of passive smoking on thyroid function among American women, those studies only targeted women of reproductive age and revealed conflicting results (21,22). A previous community-based study in Korea, where individuals consume sufficient amounts of iodine, revealed that active cigarette smoking was only associated with a decreased risk of SCH among women, and the researchers argued that smoking exhibited a negative interaction with the effects of excessive iodine on thyroid follicular cells (23). However, because that study relied on self-reported smoking data, the smoking rate was likely underestimated, especially among women. Moreover, the effect of secondhand smoke exposure was not evaluated, and the amount of iodine intake, which is closely related to thyroid function, was also measured indirectly. Thus, the present study aimed to evaluate the associations of biochemically verified active and passive smoking with thyroid function in a nationally representative Korean population.
Materials and Methods
Study subjects
The Korean National Health and Nutrition Examination Survey (KNHANES) is a nationally representative cross-sectional survey of the non-institutionalized Korean population and is performed annually by the Korean Center for Disease Control and Prevention (KCDC) (24). The survey consists of a health interview, a health examination, and a nutritional survey, which provides data regarding demographic variables, socioeconomic status, health behaviors, quality of life, biochemical profiles, and dietary intake. Stratified multistage clustered probability sampling is used to obtain nationally representative data, and individuals from selected households are included if they are aged ≥1 year.
The present study used data sets from KNHANES 2014–2015, which were the first years that included measurements of thyroid function, urinary iodine (UI) levels, and urinary cotinine levels. A total of 14,930 individuals participated in KNHANES 2014–2015, with response rates of 77.8% in 2014 (7550/9701 subjects) and 77.6% in 2015 (7380/9505 subjects). Serum TSH, free thyroxine (fT4), anti-TPOAb, and UI levels were measured in 2400 randomly selected participants (aged ≥10 years) during each year (n = 4800). A total of 3785 subjects (aged ≥18 years) were identified who had available data regarding self-reported smoking status and urinary cotinine levels. In addition, 381 subjects were excluded for the following reasons: previously diagnosed with thyroid disease (hyperthyroidism, hypothyroidism, thyroid goiter, or Hashimoto's thyroiditis) or currently taking thyroid medication (n = 189), abnormal thyroid function based on fT4 levels (n = 85; reference range 0.89–1.76 ng/mL), pregnant (n = 8), missing information regarding family history of thyroid disease (n = 60), alcohol consumption (n = 24), household income (n = 14), or body mass index (BMI; n = 1). Thus, 3404 subjects (1754 men) were included in the final analyses.
The study's protocol was approved by the Institutional Review Board of the KCDC (Cheongju, South Korea; 2013-12EXP-03-5C and 2015-01-02-6C) and complied with the Declaration of Helsinki. Moreover, all study processes complied with the STROBE guidelines, and written informed consent was obtained from all subjects (Supplementary Data; Supplementary Data are available online at
Data collection and measurement
Information regarding the subjects' socio-demographic characteristics (age, sex, household income, and education) was collected during face-to-face interviews. Data regarding health behavior and family history (alcohol consumption, smoking status, and family history of thyroid disease) were gathered using self-administered questionnaires. Household income was categorized into four groups (lowest, lower middle, higher middle, and highest), and education was also categorized into four groups (middle school, high school, college or higher, and no response). High-risk alcohol consumption was defined as seven or more drinks for men and five or more drinks for women on an occasion. A family history of thyroid disease was defined as any type of hyperthyroidism, hypothyroidism, thyroid goiter, or Hashimoto's thyroiditis.
Trained medical personnel measured the subject's body weight (kg) and height (m) while she/he was wearing light indoor clothes without shoes. BMI was calculated as kg/m2 and was categorized into three groups (<23 kg/m2, 23–24.9 kg/m2, and ≥25 kg/m2) based on the criteria for the Korean population (25).
Based on the smoking status, the subjects were categorized into three groups (active smokers, passive smokers, and nonsmokers) based on self-reported smoking status and urinary cotinine concentrations. Active smokers were defined as subjects who smoked >100 cigarettes during their lifetime and who currently smoked. Passive smokers were defined as subjects who did not actively smoke but were exposed to tobacco smoke either at home or in the workplace during the last week. Nonsmokers were defined as subjects who reported smoking <100 cigarettes during their lifetime, did not smoke currently, and were not exposed to environmental tobacco smoke. Because of the discrepancy between self-reported smoking status and cotinine-verified smoking status in the Korean population (17), urinary cotinine concentrations were used to verify each subject's smoking status. For example, subjects who were classified as nonsmokers based on their questionnaire responses were classified as passive smokers or active smokers if their urinary cotinine levels were >5 ng/mL or >50 ng/mL, respectively. However, subjects with self-reported active or passive smoking were categorized based on their self-reported status, regardless of their urinary cotinine levels. Urinary cotinine is a primary metabolite of nicotine, with a half-life of 18–24 hours, and is a reliable biomarker for nicotine exposure (26). Urinary cotinine levels were measured on the same day that the subjects completed the questionnaire and were analyzed using gas chromatography-mass spectrometry (Perkin Elmer, Waltham, MA) with a detection threshold of 0.28 ng/mL. The cutoff values for active and passive smoking were defined as >50 ng/mL and 5 ng/mL, respectively, based on the values from previous studies (17,27,28).
Venous blood samples were obtained by trained medical personnel to measure serum TSH, fT4, and anti-TPOAb. The separated serum samples were tested within 24 hours in a qualified laboratory using an electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany). The reference intervals were 0.35–5.50 mIU/L for TSH and 0.89–1.76 ng/mL for fT4. Subjects with serum TSH levels of >5.5 mIU/L were defined as having SCH, and a positive result for serum anti-TPOAb was defined as >34 IU/mL based on the kit's reference interval.
UI and the urinary iodine/creatinine (UIC) ratio, which reflects iodine intake, were measured using inductively coupled plasma-mass spectrometry for iodine (Perkin Elmer) and the Jaffe rate-blanked and compensated method for creatinine (Hitachi, Tokyo, Japan). A lower iodine level was arbitrarily defined as the lowest quartile of UI (<148 μg/L) or UIC (<100 μg/g).
Statistical analysis
The KNHANES sampling plan uses a multistage clustered probability design to generate a nationally representative sample of the non-institutionalized Korean population. In addition, the KCDC provides sample weights, which account for the complex survey design, non-responders, and post-stratification (24). Thus, sample weights were applied to all analyses based on the complex survey design.
The subjects' general characteristics were compared between the active, passive, and non-smoking groups using one-way analysis of variance for normally distributed continuous variables, while the chi-square test was used for categorical variables. Non-normally distributed continuous variables (UI, UIC, and urinary cotinine) were evaluated using the Kruskal–Wallis test. Pairwise comparisons of nonparametrically distributed variables were performed using the Mann–Whitney U-test. Based on the different active smoking rates among men and women, overall and sex-stratified differences in serum TSH, fT4, and anti-TPOAb concentrations in each smoking subgroup were calculated using the Kruskal–Wallis test. The dose–response relationships between smoking exposure and serum TSH, anti-TPOAb, or urinary cotinine levels were determined according to the quartile distributions using Jonckheere–Terpstra trend analysis.
Multivariate logistic analysis was used to estimate the associations between cotinine-verified smoking status and SCH, lower iodine levels, and anti-TPOAb. In addition, trend analysis was performed by considering smoking status as a continuous variable. Anti-TPOAb levels and UI levels were included in the analysis as covariates with age, household income, education, alcohol consumption, family history of thyroid disease, and BMI. Analyses with unweighted samples were also performed to identify any differences in the results relative to the weighted analyses. Furthermore, a sensitivity analysis was performed using a recently proposed reference interval from a nationally representative Korean population (serum TSH levels >6.86 mIU/L) (16). All tests were two-tailed, and p-values of <0.05 were considered statistically significant. All analyses were performed using IBM SPSS Statistics for Windows v24.0 (IBM Corp., Armonk, NY).
Results
Based on a combination of the self-reported and urinary cotinine verification data, the 3404 subjects included 1687 (49.6%) nonsmokers, 773 (22.7%) passive smokers, and 944 (27.7%) active smokers. The weighted overall active smoking rate was 28.2% (43.4% among men and 10.0% among women), and the weighted overall passive smoking rate was 23.1% (23.3% among men and 22.9% among women). The mean ages were 41.4 years for active smokers, 43.9 years for passive smokers, and 45.6 years for nonsmokers. Most active smokers were men, while the majority of women were in the non-smoking group. Active smokers had a higher education status than passive smokers and nonsmokers. Obese subjects were more likely to be active smokers than nonsmokers. A trend toward high-risk alcohol consumption was observed with increasing tobacco exposure. Interestingly, UI and UIC, which reflects iodine consumption, were significantly lower among active smokers than among passive smokers and nonsmokers (Table 1).
Data are presented as weighted mean (SE) or weighted percentage (SE), unless otherwise stated. p-Values were calculated with the use of one-way analysis of variance for continuous variables, the chi-square test for categorical variables, and the Kruskal–Wallis test for all other variables.
p-Values <0.05 were considered significantly different: *nonsmokers vs. passive smokers, †nonsmokers vs. active smokers, and ‡active smokers vs. passive smokers.
High-risk alcohol consumption was defined as seven or more drinks for men, five or more drinks for women on an occasion.
Thyroid disease refers to any causes of hyperthyroidism or hypothyroidism, thyroid goiter, and Hashimoto thyroiditis.
SE, standard error; IQR, interquartile range.
Serum TSH concentrations were significantly lower among active smokers than among passive smokers and nonsmokers. There was no significant difference between passive smokers and nonsmokers among either sex. Although active smokers had significantly increased overall fT4 levels, this association was not maintained in the sex-stratified analysis. Compared to male passive smokers and nonsmokers, male active smokers had slightly increased anti-TPOAb concentrations. In contrast, no significant differences were observed among women (Table 2).
p-Values were calculated using the Kruskal–Wallis test.
p-Values <0.05 were considered significantly different: *nonsmokers vs. passive smokers, †nonsmokers vs. active smokers, and ‡active smokers vs. passive smokers.
TSH, thyrotropin; T4, thyrotropin; fT4, free T4; anti-TPOAb, antithyroid peroxidase antibody.
Figure 1 shows the dose-dependent relationships between urinary cotinine-verified smoking exposure and serum TSH or anti-TPOAb concentrations. Among men, serum TSH levels decreased with increasing urinary cotinine levels (p for trend <0.001). However, this relationship was not significant among women. Under the normal reference range, serum anti-TPOAb concentrations increased with greater cotinine-verified smoking exposure among men, although no dose-dependent relationship was observed between urinary cotinine and anti-TPOAb levels among women.
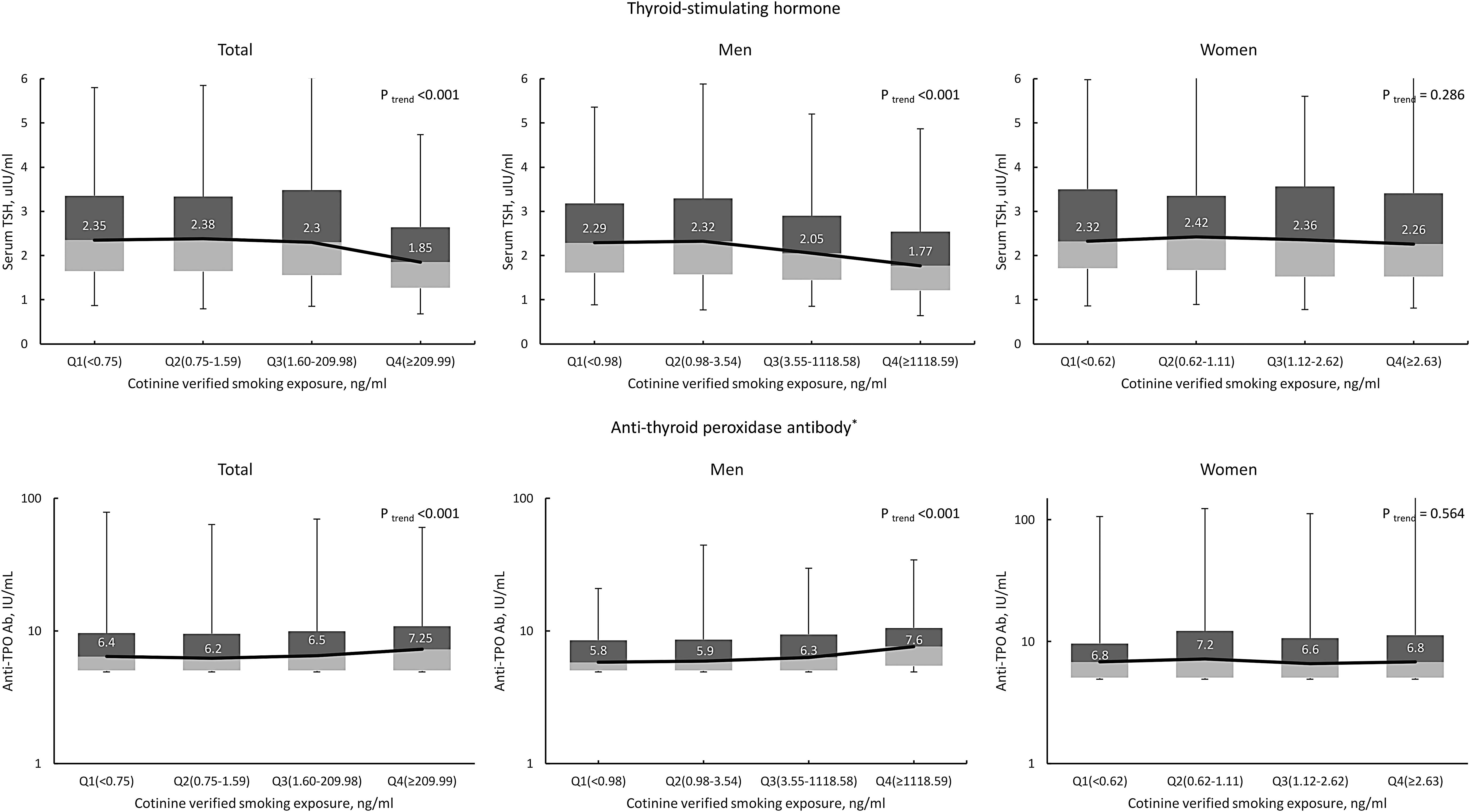
Associations of urinary cotinine-verified smoking exposure with thyrotropin (TSH) and antithyroid peroxidase antibody (anti-TPOAb) levels. Median and interquartile range of TSH and anti-TPOAb are presented with box plots. p trend was calculated with the Jonckheere–Terpstra trend test. *Numbers on the y-axis are presented in log scale.
The prevalence of SCH in the present study was 5.0% (4.2% among men and 6.0% among women), and SCH was less prevalent among male active smokers than among male passive smokers and nonsmokers (Table 3). The risk of SCH tended to decrease with greater smoking exposure in the multivariate-adjusted analysis (p for trend = 0.027 among men and 0.042 among women). In the pairwise comparisons, only active smokers had a decreased risk of SCH. No significant difference was observed between passive smokers and nonsmokers. Moreover, although the magnitude of the association decreased slightly among women, this association persisted in the unweighted analysis (Supplementary Table S1). When a sensitivity analysis was performed using a recently proposed reference value for SCH in the Korean population (>6.86 mIU/L), similar relationships were observed between SCH and active or passive smoking, although these relationships were not statistically significant (Supplementary Table S2).
p-Values were calculated using the chi-square test for SCH prevalence and logistic regression test for OR for SCH.
p-Values <0.05 were considered significantly different: *nonsmokers vs. passive smokers, †nonsmokers vs. active smokers, and ‡active smokers vs. passive smokers.
Age, household income, education, alcohol consumption, family history of thyroid disease, BMI, anti-TPOAb, and urine iodine were adjusted in multivariate analysis.
SCH, subclinical hypothyroidism; OR, odds ratio; CI, confidence interval; BMI, body mass index.
Compared to passive smokers and nonsmokers, active smokers of both sexes were more likely to have lower UI concentrations. However, this relationship was only marginally significant among men (Table 4). The rates and risks of anti-TPOAb positivity did not vary significantly according to smoking status (Supplementary Table S3).
Lower iodine states were arbitrarily defined as the lowest quartile of urine iodine/creatinine (UIC) level <100 μg/g or urine iodine (UI) level <148 μg/L. p-Values were calculated using the chi-square test for lower iodine states prevalence and logistic regression test for odds ratio for lower iodine state.
p-Values <0.05 were considered significantly different: *nonsmokers vs. passive smokers, †nonsmokers vs. active smokers, and ‡active smokers vs. passive smokers.
Age, household income, education, alcohol consumption, family history of thyroid disease, BMI, and anti-TPOAb were adjusted in multivariate analysis.
Discussion
This is the first study to investigate the associations between cotinine-verified active and passive smoking and thyroid function and the risk of SCH among a nationally representative Korean population. It was found that increased smoking exposure exhibited a dose-dependent association with decreased serum TSH levels, and increased smoking exposure was associated with a lower risk of SCH. In addition, increased smoking exposure was associated with lower UI levels and higher serum anti-TPOAb levels, although the relationship with serum anti-TPOAb levels was only significant among men.
Self-reporting is an unreliable method for assessing smoking status in Korean population-based studies, as smoking rates are likely to be underestimated, especially among women (17). For example, several nationwide studies conducted in South Korea have revealed that the cotinine-verified active smoking rate was two to three times higher than the self-reported smoking rate among women, although self-reported active smoking data were acceptably accurate among men (κ = 0.87) (17,19). Moreover, both active and passive smoking rates were underestimated when smoking status was assessed via self-report (28). Although the cause of this discrepancy is unclear, under-reporting of smoking rates can affect the results of smoking-related studies. Thus, to minimize any misclassification that could occur with a self-administered questionnaire, the results were confirmed by testing urinary cotinine levels, an objective biomarker for smoking status. However, because urinary cotinine only reflects tobacco exposure within a short period (48–72 hours) (18), subjects who had been exposed to smoking three to four days before testing may be misclassified as nonsmokers instead of active or passive smokers. Therefore, initially, the subjects' smoking statuses were determined based on their self-reported status, and then the self-reported status was verified using urinary cotinine concentrations.
The present study demonstrates that active and passive smoking were associated with decreased serum TSH concentrations, and this result is consistent with the findings of previous studies (12,15,20). An analysis of NHANES III data revealed that active smokers were relatively less likely to have serum TSH levels >4.5 mIU/L (15), and a population-based Norwegian study (the HUNT study) confirmed that current and former smokers had significantly lower serum TSH levels than never-smokers (12). In addition, a community-based Korean study revealed that current and former smokers had significantly lower serum TSH levels than never-smokers (23). The present study also revealed a dose-dependent relationship between the magnitude of smoking exposure and decreased serum TSH levels among male subjects. Similarly, a previous study revealed a 1.4% decrease in the likelihood of having TSH levels >4.5 mIU/L for every 10 ng/mL increase in serum cotinine levels (15). Although passive smokers had a higher likelihood of decreased serum TSH levels than never-smokers, this association was not statistically significant. Nevertheless, the results of previous studies on the influence of passive smoking on serum TSH levels have been inconsistent. For example, one study revealed that passive smoking was not associated with any significant changes in serum TSH levels among women of reproductive age (22). However, another study of women aged 18–44 years revealed that passive smoking was significantly associated with lower serum TSH levels compared to non-smoking (21). The different definitions of passive smoking may explain these discrepant results. In the present study, passive smoking was defined as being exposed to tobacco smoke during the last week and/or having urinary cotinine levels of 5–49.9 ng/mL. In contrast, previous studies have defined passive smoking based only on serum cotinine levels (1.1–10 ng/mL) (22) or exposure to secondhand smoke during the last six months with serum cotinine levels of 0.54–15 ng/mL (21).
The present study revealed an association between increasing smoking exposure and decreasing SCH, similar to previous studies (12,15,23,29). Furthermore, the magnitude of the decreased risk of SCH in the active smoking group was higher among women than among men, and similar results were revealed in a Norwegian study (12). Nevertheless, although the magnitude of the association was higher among female subjects, the number of female active smokers (n = 179) may be too small to determine statistical significance. Based on the controversy regarding the serum TSH reference interval in the Korean population, the association of smoking with SCH was estimated by applying the upper limit from the recently proposed serum TSH reference interval (>6.86 mIU/L) (16). This approach did not generate a statistically significant result, although the underlying relationship was preserved.
Several theories have been proposed to explain the inverse relationship between smoking and the risk of SCH. First, lower anti-TPOAb concentrations in active smokers may lead to a decreased risk of SCH (14,15), and this theory is supported by a prospective study that showed that smoking cessation increased the likelihood of anti-TPOAb positivity (30). However, the present study revealed that the risk for anti-TPOAb positivity was not lower among active smokers and that a slightly increased concentration was detected among male active smokers below the lower end of the normal reference range (<34 IU/mL). Second, increased fT4 levels after smoking exposure may help explain the influence of smoking on thyroid function (10). A Norwegina study (the 5th Tromsø study) revealed higher fT4 levels in smokers than in nonsmokers, while the results of the HUNT study were similar (12,20). Moreover, an experimental study revealed that one hour of secondhand smoke exposure generated higher serum triiodothyronine and fT4 levels (31). However, there are conflicting results regarding the effects of smoking on T4 concentrations. The present study and a previous Korean community-based study revealed that serum fT4 concentrations did not differ according to smoking status (23). In contrast, two American studies revealed lower T4 levels among female active smokers than among female passive smokers and nonsmokers (21,32). It is also possible that relatively lower iodine levels in active smokers may be partially implicated in the findings. A previous Korean study revealed a positive association between iodine intake and SCH only among nonsmokers. That association was not detected among active smokers, which suggests that tobacco exposure may mitigate excessive iodine intake (23). Thiocyanate from smoking competitively inhibits iodide uptake by the sodium–iodide symporter. Hence, thiocyanate can reduce iodide uptake in thyroid follicular cells (33,34), which may explain the observed protective effect of smoking in individuals with excessive iodine exposure. Although excessive iodine intake is mainly associated with an increased risk of SCH and overt hypothyroidism among subjects with slightly elevated TSH levels or thyroid-stimulating antibodies (8,9,35), no significant differences were observed in anti-TPO positivity according to smoking status. Moreover, the magnitude of the difference in iodine levels between active smokers and nonsmokers (approximately 25 μg/L in the present study) seems unlikely to alter iodine homeostasis in the thyroid gland and decrease the risk of SCH (35).
This study has several limitations. First, the cross-sectional design cannot address temporality. Therefore, the causality of the observed associations should be interpreted with caution. However, several cohort studies have also revealed similar findings (12,20), and it is more likely that smoking affects thyroid function, rather than thyroid function affecting smoking exposure. Second, even though smoking status was classified based on self-reported and urinary cotinine data, the possibility of misclassification remains, as there is no consensus regarding the urinary cotinine cutoff values to differentiate between active smokers, passive smokers, and nonsmokers. Nevertheless, cut-off values (≥50 ng/mL and ≥5 ng/mL) were selected that are widely used in population-based Korean studies and that are supported by findings from other studies (17 –19,27,36). Third, thorough thyroid exams, ultrasonography, and thyroid scans were not performed to detect unidentified or occult thyroid disease, and it is possible that subjects with overt thyroid disease may not have been excluded from the analyses. However, despite these limitations, this study is the first to investigate the associations of cotinine-verified active and passive smoking with thyroid function in a nationally representative Korean population.
In conclusion, active and passive smoking were associated with decreasing serum TSH levels and a decreased risk of SCH in a Korean population. Furthermore, active smokers had significantly lower iodine levels than passive smokers and nonsmokers, which may be related to the decreased risk of SCH among active smokers. Further studies are needed to clarify the mechanisms that underlie these relationships.
Footnotes
Acknowledgments
The abstract for this report was presented during a poster session at the 87th annual meeting of the American Thyroid Association in Victoria, British Columbia, Canada (Short Call 23).
Author Disclosure Statement
All authors declare that they have no conflicts of interest.