
Abstract
Background:
Therapy with radioactive iodine (131I) is a well established treatment method for postsurgical differentiated thyroid carcinoma (DTC). A fixed discharge time is generally set, regardless of individual differences in residual body radioactivity (RBA). This study aimed to investigate the RBA of each patient to find the attenuation law and to identify underlying factors in order to predict the time point for a safe, scientifically sound discharge plan.
Methods:
A total of 231 DTC patients undergoing 131I treatment were all treated with 3.7 GBq (100 mCi) of 131I. RBA was estimated by measuring the external body dose rate (EDR) at a distance of 1 m from the body surface between 0 and 72 hours after oral administration of 131I. Data from each patient were used to establish a time–EDR value (h–μSv/h) curve. Software was developed to predict the time when a patient's dose equivalent meets the national safety standard by including six time points between 40 and 60 hours. Several factors that might affect that time were analyzed.
Results:
The EDR attenuation law in patients could be described with a double exponential decay model, and the cutoff value was set as 23.3 μSv/h, upon which the predictive software was developed. Student's t-test showed there was no statistical difference between predicted values and the actual measured values (p > 0.05). Correlation analysis found that serum thyroglobulin, total triiodothyronine, total thyroxine, free triiodothyronine, free thyroxine, thyrotropin, 2- and 24-hour iodine uptake rate of the thyroid, scores of 99mTc-pertechnetate thyroid scan, scores of 131I whole-body scan, scores of ultrasound scan, and gastrointestinal residues were associated with attenuation speed. A further multiple linear regression analysis found that 24-hour iodine uptake (X 1), residual thyroid grading by 131I whole-body scan (X 2), blood free triiodothyronine (X 3) and free thyroxine (X 4) predominantly influenced the decline of the EDR. The regression equation was Ŷ = 2.091X 1 + 6.370X 2 + 4.529X 3 + 2.466X 4 – 8.614 (F = 44.03, p < 0.01).
Conclusions:
An effective and convenient method was created to measure and predict the individual safety time for discharge. This could play a significant role not only for scientific hospital discharge planning, rational use of medical resources, and better individualized management, but also in public radiation protection.
Introduction
T
As an adjuvant therapy to surgery and an essential approach for the therapy of patients with advanced carcinomas, radioactive iodine (RAI; 131I) has been used in thyroid cancer for >70 years (4). After oral administration of 131I, most of the radioiodine is taken up and concentrated into the thyroid tissue. 131I is a beta-decaying nuclide, emitting 99% β-rays and 1% γ-rays. The maximum energy of the β-ray is 0.6065 MeV (89% abundance), and the main γ-ray energy is 0.364 MeV (81% abundance) (5). The ablation function of 131I mainly depends on β-rays, with an average range of 0.4 mm in soft tissue, which can destroy thyroid follicular cells to clear residual thyroid tissue after surgery (6). However, γ-rays cause relatively little ionization but have far greater penetrating power, leading to some radiation safety issues concerning the surroundings (7). The International Atomic Energy Agency indicates that patients who receive radioactive iodine therapy should not be discharged until the remaining activity of radioiodine has decreased to an acceptable level (8). This means patients undergoing 131I treatment cannot be discharged until their residual body radioactivity (RBA) drops to a safe level. In China, the current level considered to be safe is set at 400 MBq, according to the latest official document on patient radiological protection in nuclear medicine. This implies that the external body dose rate (EDR) at 1 m must be <23.3 μSv/h (9).
However, the attenuation rate of RBA varies from patient to patient because of a variety of factors. At present, most hospitals set a unified admission and discharge time regardless of individual differences. In this study, the changes of EDR of patients at different time intervals were examined to estimate RBA and to find its attenuation law. Furthermore, several factors were analyzed that may affect the external radiation dose rate, and predictive software was developed to assist physicians to predict the time at which the radiation dose of each patient meets the national standard. This information would allow a more scientific and individualized discharge plan to be made.
Methods
Patients
Two hundred and thirty-one DTC patients (n = 231) who underwent 131I ablation of residual thyroid tissue at Shanghai Ren Ji Hospital, P.R. China, between February 2015 and May 2017 were enrolled in this study. All patients had pathologically confirmed DTC and underwent a total or near total thyroidectomy with or without additional central and/or lateral lymph node dissection. The following information was analyzed and recorded for every patient: age, sex, tumor pathology, regional or distant metastases, approach, and time of surgery, as well as levels of thyroid stimulating hormone (TSH), baseline thyroglobulin (Tg), and anti-Tg antibodies (TgAb).
Surgical specimens of all patients were analyzed and classified according to standards prevailing at the time of initial treatment. The present study used the histological and tumor-node-metastasis (TNM) classification given in the original pathology report (the eighth edition of the TNM system until 2017) (10). The thyroid 131I uptake rate was determined before RAI treatment, and patients with a thyroid remnant uptake >10% were excluded (11,12). No patients underwent contrast-enhanced computed tomography scans within two months prior to RAI treatment.
Patient management and measurement of EDR
Before RAI treatment, all patients stopped taking levothyroxine for about four weeks and were instructed to follow a low-iodine diet and to stop any drugs containing iodine. 131I treatment would not start until the patient's serum TSH was >30 mIU/L. All patients were treated with an activity of 3.7 GBq (100 mCi) 131I for ablation of residual thyroid tissue.
The patients took 131I orally at 2:00pm on the second day of hospitalization. EDRs were measured at a distance of 1 m from the body anterior surface of each patient and at a height of 1.5 m above the floor at time intervals of 0, 2, 4, 6, 18, 20, 24, 26, 28, 30, 42, 44, 48, 50, 52, 54, 66, 68, and 72 hours after administration of 131I. The chosen times allowed measurements to be avoided while patients were sleeping. The initial measurements were performed immediately after 131I administration before the onset of renal clearance. The study also concurrently measured the background EDR and calculated the patient net value at the same time for each measurement. The EDRs were measured with the Ludlum Model 375 area monitor detector system (BqSv; Becquerel & Sievert Co. Ltd., Beijing, P.R. China).
The EDR data for all patients were recorded in accordance with the time–radiation residue (h–μSv/h) for the horizontal and vertical coordinates. Data of 19 time points fitted a curve for each patient, but for a minority of patients, some uncollected data points might result from complicated circumstances and some accidents; for example, some patients missed the measurement because of sleeping too early or bathing at those time points. Some absent data played an insignificant role in data processing and had no effect on overall radioactivity of attenuation law, sufficient data were measured for each patient. The complete data vector of residual activity was: at =0, at =2, at =4, at =6, at =18, at =20, at =24, at =26, at =28, at =30, at =42, at =44, at =48, at =50, at =52, at =54, at =66, at =68, and at =72. A total of 19 samples were taken in the 72-hour interval, and the data could be described by a residual radioactive descent model. The suitable characterization of the law and accurate prediction depends on the selection of models. As the decay law of radioactive material follows an exponential decay model and the drug's in vivo metabolism approximately follows an exponential decay model, a decision was made to use the double exponential decay model to describe the attenuation law of RBA after RAI treatment (13). Using this function model, predictive software was developed.
All patients were hospitalized for three days in shielded rooms. Their serum Tg, total triiodothyronine T3 (TT3), total thyroxine (TT4), free triiodothyronine (fT3), free thyroxine (fT4), TgAb, and TSH were measured on the first day of hospitalization before administration of 131I. Patients were encouraged to drink water and urinate regularly to accelerate the excretion of free iodine after oral administration of iodine solution. All patients underwent 131I whole-body scans on day 3 after administration. The patients were started on hormone suppression treatment with levothyroxine on day 4 after the administration of RAI.
The postoperative Technetium-99m (99mTc)-pertechnetate thyroid scanning images and 131I whole-body scanning images were visually and semi-quantitatively analyzed. The size of the residual thyroid was divided into three levels based on the uptake of 99mTc or 131I, and scored as follows: 0, no uptake in the bed of thyroid glands; 1, faint uptake; 2, moderate uptake; and 3, intense uptake. Radioactivity in the digestive tract was scored as follows: 0, no uptake; 1, uptake limited to the stomach or unilateral intestinal uptake; 2, both gastric and unilateral intestinal uptake or bilateral intestinal uptake; and 3, both gastric and bilateral intestinal uptake. Pretreatment ultrasound scores were established based on the detection of residual thyroid tissue: 0, negative results; 1, positive results.
Statistical analysis
Data analysis was performed with PASW Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL). All data are shown as the mean ± standard deviation (SD), with ranges given if necessary. Continuous variables were compared with an unpaired t-test, and categorical variables were compared with the chi-square test. The relationship between radiation dose rate and clinical or laboratory variables was evaluated with a multivariate linear regression model. The R 2 coefficient of determination measures how well the regression predictions approximate the real data points. The larger the R 2, the better the regression model fits the data. Repeated measurements were assessed using analysis of variance (ANOVA). All tests were two-tailed. The results were considered significant at the 5% level of significance and strongly significant at the 1% level of significance.
Results
A total of 231 DTC patients (155 [67.1%] females) were included in this study to take 131I ablation therapy and to measure their radiation dose rate. The median age was 42.66 years (range 20–70 years), and 24.24% (n = 56) were >55 years old. Among all patients, 180 underwent only one surgery, 46 underwent a secondary surgery, and five underwent three operations. One hundred and fifty-four patients underwent total thyroidectomy, and 77 patients underwent a total thyroidectomy of one lobe and a subtotal thyroidectomy of the contralateral lobe. All patients underwent central lymph node dissection, and 45.02% (n = 104) also underwent cervical lateral node dissection. The postoperative pathology showed that the most common pathological type was PTC, accounting for 97.4% (n = 225) of the cases, and the remaining six cases were follicular thyroid carcinomas. The patient characteristics are presented in Table 1. As shown in Table 2, the M ± SD values for the patients' age, serum TSH, Tg, TgAb, the dose of levothyroxine, and withdrawal time were 42.66 ± 12.45 years, 112.69 ± 35.13 mIU/L, 23.14 ± 65.07 ng/mL, 77.80 ± 276.12 IU/mL, 98.76 ± 21.48 mg/day, and 28.57 ± 2.46 days, respectively.
TSH, thyrotropin; Tg, thyroglobulin; TgAb, anti-Tg antibodies.
EDR values of each patient were recorded and included into the statistical analysis to estimate RBA. Different patients showed different decay rates with the same dose of radioactive drug. When the safe level of RBA is set as 400 MBq, the corresponding EDR value is 23.3 μSv/h, which meets the national safety standard. As shown in Figure 1, more than half of the patients reached the safe level at 50–80 hours; nearly 30% of patients reached the safety value after 80 hours.

The time for patients to reach the safe value (μSv/h). More than half of the patients reached the safe level at 50–80 hours.
The data for each patient were used to generate a “time–EDR value” (h–μSv/h) curve, and the cutoff value was set as 23.3 μSv/h (Fig. 2). A double exponential decay model was used to describe this radioactive attenuation law; the function formula is:
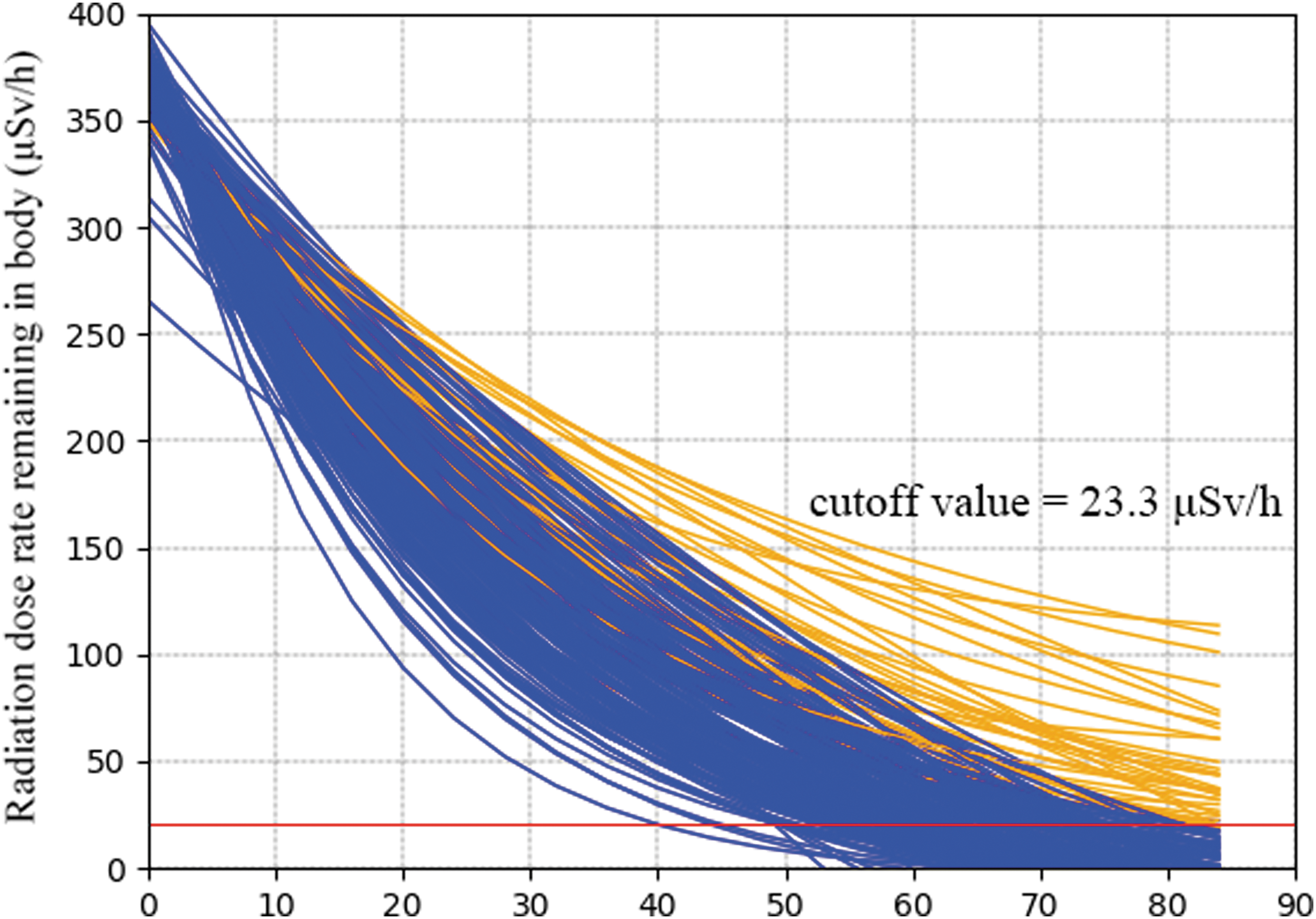
All the external body dose rate (EDR) data were measured at a distance of 1 m from the patients' body surface. Each patient corresponds to a “time–EDR value” (h–μSv/h) curve, and the cutoff value was set as 23.3 μSv/h. The blue curves indicate that the EDR value met the safety standard at discharge time. Patients represented by the orange curves did not.
In this study, the mean EDR values of the 19 time points were divided into two groups on the basis of reaching the cutoff value 23.3 μSv/h or not at discharge, which corresponded to two different suitable radioactive attenuation curves. The function curves are shown in Figure 3. The function formulas for the two groups are:
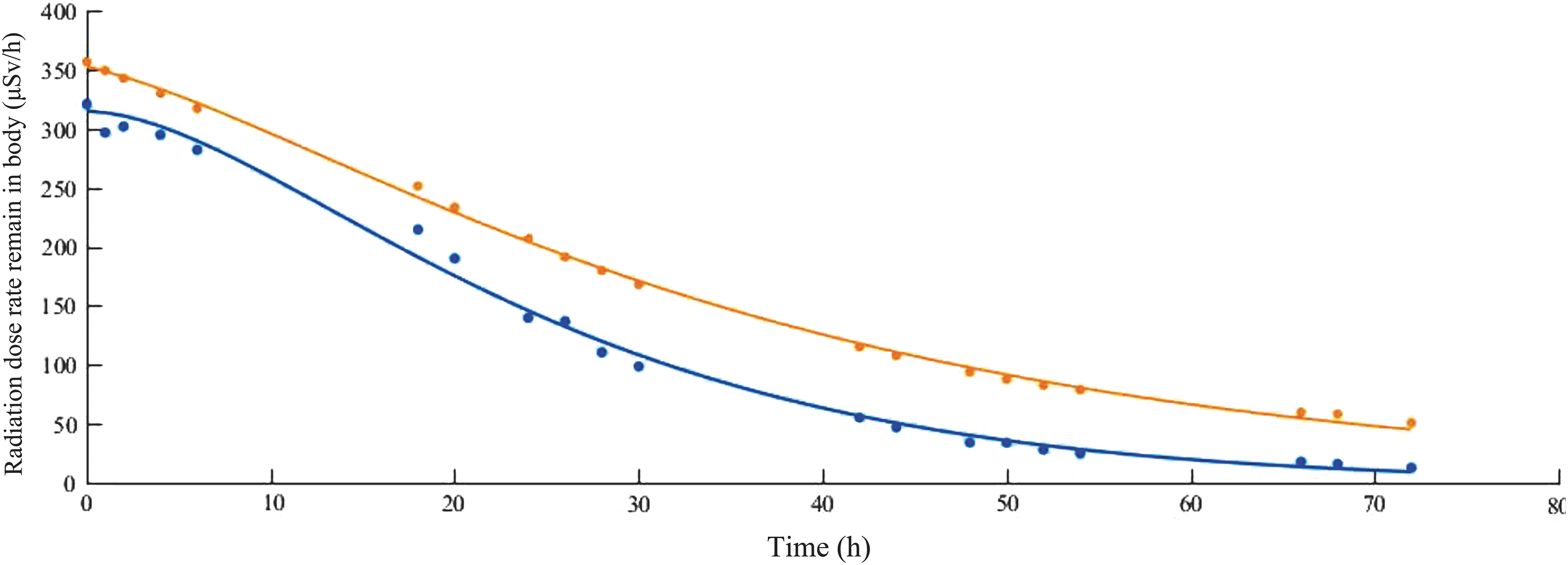
A double exponential decay model (y = a·e b·t + c·e d·t ) was used to describe the attenuation law of two groups' residual activity after 131I therapy. Mostly, values of 19 points were input to fit the function. The blue curve represents the group that reached the safe level (23.3 μSv/h) at discharge time; the orange curve represents the group that did not.
where EDR1 represents the function formula for patients reaching the national standard target value when leaving the hospital, EDR2 represents the function formula of the patient group who did not reach the target value, and t represents the time after 131I administration.
Simple predictive software was developed to predict the time when a patient's RBA reaches the national safety standard. For a single patient, six EDR values of any time points between 40 and 60 hours can be integrated to obtain a prediction for when a safe time for discharge will be reached (Fig. 4). Prediction accuracy was tested by performing a paired-sample t-test to compare the predicted values and the actual measured values in a period of 72 hours. The M ± SD values were 28.33 ± 27.97 and 28.44 ± 30.00, respectively. No statistical difference between the two groups was found (t = 0.220, p > 0.05).
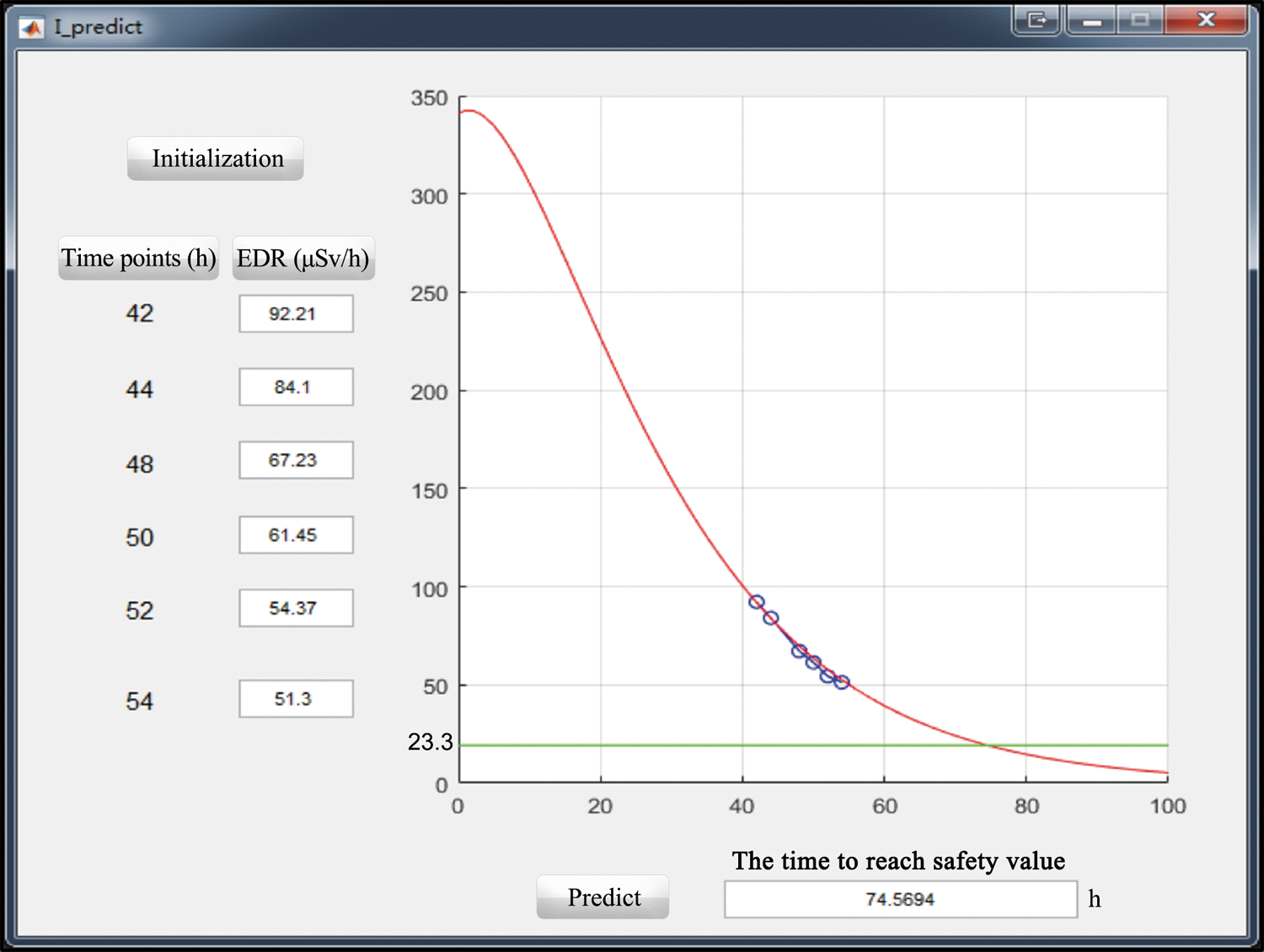
The interface of the predictive software. Six values were input between 40 and 60 hours to obtain the time when the EDR value of this patient would reach the safe level (23.3 μSv/h). Every patient's unique decay curve equation could be calculated via six data vectors of EDR: V origin = yt =42, yt =44, yt =48, yt =50, yt =52, yt =54. The following function formula was used: y = a·e b·t + c·e d·t = 23.3 μSv/h.
Considering that some clinical and laboratory factors could affect the EDR values and decay law, some common indicators of thyroid function were analyzed. The time to reach the target level (23.3 μSv/h) represents the EDR attenuation speed. Correlation analysis showed that 12 factors were associated with the attenuation speed to a variable degree: serum Tg, TT3, TT4, fT3, fT4, TSH, 2- and 24-hour radioiodine uptake, scores of 99mTc-pertechnetate thyroid scan, scores of 131I whole-body scan, ultrasound scores, and gastrointestinal uptake (the grading criterion is detailed in Supplementary Table S1 and Supplementary Figs. S1–S3; Supplementary Data are available online at
EDR, external body dose rate; TT3, total triiodothyronine; TT4, total thyroxine; fT3, free triiodothyronine; fT4, free thyroxine.
Considering that correlation analysis is affected by the interaction of variables, multiple linear regression analysis was used. It was found that 24-hour iodine uptake rate (X
1), residual thyroid grading by 131I whole-body scan (X
2), and blood fT3 (X3) and fT4 (X4) predominantly influenced the decline of the EDR. The regression equation was:
where Ŷ represents the time to reach the safe level of 23.3 μSv/h.
ANOVA found a significant difference in 99mTc-pertechnetate thyroid scan scores, 131I whole-body scan scores, gastrointestinal uptake, and 24-hour iodine uptake between groups (p < 0.05). Student's t-test was used to analyze ultrasound scan and TT3 between groups (p < 0.05), as shown in Table 4.
The reference value is given in parentheses.
ANOVA, analysis of variance.
Discussion
Postoperative 131I remnant ablation or therapy is commonly performed after thyroidectomy in patients with DTC, in particular for those who have lymph node or distant metastases (2). However, the incidence of DTC has substantially increased, and in many countries, such as China, radioiodine therapy requires isolation and hospitalization of patients, which may lead to a shortage of specialized units. Whether patients should be released or have contact with others depends on precautions and regulations with regard to remaining activity and associated exposure rate (14). Although the metabolic clearance rate of radiopharmaceuticals and the amount of residual thyroid tissue varies substantially among individuals, thereby resulting in variable clearance rates (15), most hospitals set a unified admission and discharge time regardless of individual differences. At the authors' hospital, patients are usually discharged after 72 hours. However, a fixed discharge time appears to be problematic. While the majority of patients have reached the required national safety standard, a small group of patients may not reach the acceptable value for discharge (Figs. 1 and 2). This group of patients must continue to be isolated at home and be educated to protect family members and neighbors from possible radiation exposure (16).
This study recorded EDR values of all patients in accordance with the “time–radiation residue” (h–μSv/h) for the horizontal and vertical coordinates and used a double exponential decay curve to depict the law of radioactive attenuation. The results of accuracy prediction showed the appropriateness of this double exponential decay model. The study tried to predict the exact time when each patient reaches a safe value by measuring fewer EDR values in order to avoid excessive interventions and to decrease the workload of medical staff. A database of EDR values and curves was constructed for all patients. It was then found that the curves have the best distinction in the interval of 40–60 hours. To obtain the unique decay curve equation for each patient, six data points were then included: V origin = yt =42, yt =44, yt =48, yt =50, yt =52, yt =54. This allowed us to develop a model for predicting when a patient would reach the cutoff value of 23.3 μSv/h (Fig. 4).
Previous studies have analyzed the relation between EDR and RBA of DTC patients undergoing 131I therapy. Zhang et al. (17) found that there was a significant positive correlation between EDR at a given distance, and the RBA was calculated in their study. Measuring EDR around patients is only one of the established methods to estimate RBA. Thomas et al. (18) compared three methods of evaluating RBA and concluded that the direct EDR method was an accurate, reliable, and safe method for monitoring a patient's 131I RBA. Compared to other studies, the patients in the current study all received 100 mCi radioiodine and thus an identical activity at the onset. However, there are some methodological limitations. First, only determined EDR data at 1 m was involved. EDR values at distances of 2 and 3 m from patients' thyroid glands have begun to be measured. Once enough data have been collected, more work will be done. Second, the urinary system was generally considered the major path of 131I excretion (19). Therefore, evaluating RBA by measuring activity in the urine will be conducted in future work.
Among the 12 variables for correlation analysis, TSH and Tg are important laboratory indicators for prognostic evaluation for DTC patients. In particular, Tg is a reliable indicator for early detection of residual or recurrent disease (20). 99mTc-pertechnetate thyroid scan and 131I whole-body scan are two effective radionuclide imaging modalities to predict whether the tissue is radioiodine avid and thus are important before 131I therapy to reveal the ability of thyroid tissue to take up radioiodine (21,22). The correlation coefficients of these 12 variables were all >0.2, except the Tg level, which was 0.147. The best correlation reaching 0.544 was found with the 24-hour iodine uptake rate. Further multiple regression analysis demonstrated the importance of 24-hour iodine uptake rate, 131I whole-body scan, and serum fT3 and fT4 in predicting the speed of radioactive decay. A higher 24-hour iodine uptake rate, higher 131I whole-body scan scores, and higher fT3 and fT4 values suggest slower EDR descent. 99mTc-pertechnetate thyroid scanning is a key means for diagnosis of DTC patients, and it can also be used for the evaluation of patients with Graves' disease or thyroiditis (23,24), but the uptake of 99mTc does not truly reflect the volume of residual thyroid, and it is thus less related to the EDR decline law.
During RAI treatment of patients with DTC, radioiodine not only accumulates in thyroid tissue, but other tissues may also take up radioiodine or are exposed otherwise (25). Therefore, during hospitalization, patients are asked to take acidic foods such as lemons or plums and to chew gum to reduce the risk of potential damage to the salivary glands through accelerating salivary secretion. Drinking water increases urine excretion to protect the kidneys and bladder. After discharge from hospital, patients need to follow home-care precautions to limit radiation exposure to family members. The American Thyroid Association has proposed some specific recommendations. For example, it is suggested that patients sleep in separate beds at least six feet apart throughout the night-time. Patients are recommended to shower every day and to avoid intimacy, such as kissing and sexual intercourse. After using the toilet, the seat should be cleaned, and the toilet should be flushed a few times (26).
For the future application of this study for individualized management guidance, EDR measurements need to take different distances into account and measurement accuracy needs to be improved further improve. Ultimately, this will permit the development of more scientific discharge plans and patient education handouts in light of their EDR measurements.
Conclusions
This work has established a stable and reliable model to estimate RBA by dynamically monitoring EDR values in DTC patients after RAI treatment. Efficient software has been developed to predict an optimal and scientific discharge time. The proposed methodology allows the systematic development of a database for experimental evaluation of clinical practice guidelines for reducing radiation exposure. The optimal time point for a safe and scientifically sound discharge guideline would play a significant role in public radiation protection, and in the rational use of medical resources and improved individualized patient management.
Footnotes
Acknowledgments
This work was supported by National Natural Science Foundation of China (81471708, 81771861), cross-research fund for medical engineering of Shanghai Jiao Tong University (YG2016MS55), and Shanghai Municipal Education Commission—Gaofeng Clinical Medicine Grant Support (no. 20172010). Thanks to Prof. Xiuying Wang from the University of Sydney for assistance in the revision of linguistic accuracy.
Author Disclosure Statement
The authors have declared that no competing interests exist.