
Abstract
Background:
Patients with excellent response to initial therapy have a low rate of tumor recurrence. The objectives of this study were to evaluate the rate of early tumor recurrence in patients with intermediate-risk papillary thyroid cancer who had an excellent response to initial treatment and to identify risk factors.
Methods:
This retrospective cohort study included 217 patients with American Thyroid Association intermediate-risk papillary thyroid cancer who had a documented excellent response to initial treatment (total thyroidectomy and adjuvant therapy with 100–150 mCi [3.7–5.5 GBq] of radioactive iodine [RAI]). The assessed outcome was recurrence, defined as new evidence of disease after any disease-free period. Multivariate logistic regression and Cox regression models were used to determine the factors associated with recurrence upon recording clinical, surgical, and pathology variables.
Results:
Sixteen (7.4%) cases of recurrent disease were documented after a median follow-up period of 42 months (range 17–88 months). Structural recurrence was documented in 10 (62.5%) patients, and biochemical recurrence was documented in the remaining six patients. The logistic regression model identified a significant association between early recurrence and pN1b involvement (odds ratio [OR] = 10.81 [confidence interval (CI) 1.87–62.59]), lateral neck RAI uptake (OR = 6.06 [CI 1.67–22]), and pre-ablation thyroglobulin >10 ng/mL (OR = 4.01 [CI 1.16–13.85]). Variables that proved significant in the Cox regression model were: pN1b involvement (hazard ratio = 9.6 [CI 1.91–48.52]) and lateral neck RAI uptake (hazard ratio = 5.95 [CI 1.86–18.97]).
Conclusion:
The observed early recurrence rate of 7.4% is uncharacteristically high for a population of patients who had an excellent response to initial treatment. The significant association that was found between recurrent disease and lateral neck lymph node metastasis, lateral neck I131 uptake in post-therapy whole-body scan, and pre-ablation thyroglobulin levels >10 ng/mL indicates that early recurrence (<5 years) most likely indicates progression of micrometastatic disease already present at diagnosis and unsuccessfully eradicated with initial therapy.
Introduction
T
The rate of long-term recurrence is reported to be <4% once an excellent response to initial treatment is achieved (4 –7), regardless of the initial risk estimate. Intermediate-risk patients are clinically characterized by having suspected albeit unrecognized residual disease. Early recurrence (<5 years) most likely indicates progression of micrometastatic disease already present at diagnosis and unsuccessfully eradicated with initial therapy (8).
It is not sufficient simply to classify patients as intermediate risk, and it is important to separate patients with “lower-risk features” from those with “higher-risk features” in order to personalize optimal treatment and monitoring. Traditional risk-stratification systems are not sufficiently reliable (1,9) for at least two reasons: (i) they are primarily based on information from surgical pathology, inherently limited by the extent and completeness of surgical resection (10) and the accuracy of specimen labeling; and (ii) the effect of therapy is not integrated into risk assessment (4 –7), including information provided by post-therapeutic RAI whole-body scanning about the presence and staging of residual disease and RAI avidity. In addition, there is a paucity of data regarding treatment of intermediate-risk patients. Therefore, the objective of this investigation was to identify risk factors associated with early tumor recurrence in a cohort of patients with intermediate-risk thyroid cancer with documented excellent response to initial treatment.
Methods
Upon obtaining approval from the Institutional Research Board, the physical and electronic medical records of all patients with differentiated thyroid cancer (DTC) referred to the National Cancer Institute (Instituto Nacional de Cancerología) in Bogota, Colombia, between January 2009 and December 2013 were retrospectively reviewed. Patients >18 years of age with ATA 2009 intermediate-risk papillary thyroid cancer (PTC) evident on surgical histopathology whose initial treatment included total thyroidectomy and RAI therapy were identified. Surgical procedures performed within one year of the first surgery to optimize control of locoregional disease were considered as part of the initial treatment. To reduce heterogeneity, only patients staged between T2N1 and T3N1 were included. All patients had been treated with an administered RAI activity between 100 and 150 mCi (3.7 and 5.5 GBq) in accordance with the institution's guidelines (11). Most patients received RAI therapy after two to four weeks of levothyroxine withdrawal (thyrotropin [TSH] ≥25 IU/L), and 11% received RAI therapy after preparation with 0.9 mg intramuscular recombinant human TSH (rhTSH) on two consecutive days, followed by RAI on the third day and post-therapeutic scanning on the fifth day. Patients were excluded if they had not received RAI therapy within 15 months of the first surgery, or if follow-up was <12 months after RAI therapy, or if thyroglobulin (Tg) levels were <1 ng/mL in the presence of Tg antibodies (TgAb) persistently >60 ng/mL, or if their medical records had insufficient information to allow initial risk stratification and response to initial treatment. At least one year of follow-up was required after treatment response assessment, or until disease recurrence was documented, whichever occurred first. Only patients with excellent response to initial treatment were recruited. To establish response to initial treatment, all patient data obtained between 6 and 24 months after initial RAI therapy were examined, incorporating results from clinical exams, neck ultrasounds, fine-needle aspiration (FNA), RAI whole-body scans, and measurements of stimulated and suppressed Tg using a chemiluminescent assay (Immulite 2000 Thyroglobulin; Diagnostic Products, Los Angeles, CA) with a functional sensitivity of 0.2 ng/mL. Starting in 2011, all Tg values were measured using the ECLIA electrochemiluminescence assay (Roche Diagnostics International, S.L., Barcelona, Spain) with a functional sensitivity of 0.04 ng/mL. An excellent response required (i) both suppressed and stimulated Tg levels <1 ng/mL, (ii) anti-TgAb <60 ng/mL (6), (iii) neck ultrasound showing no evidence of disease (NED), and (iv) negative cross-sectional images or RAI whole-body scan (4). The primary outcome was recurrence, defined as new evidence of biochemical, structural, or functional disease after any disease-free period. Biochemical recurrence was defined as suppressed Tg levels ≥1 ng/mL or stimulated Tg levels ≥2 ng/mL, or a progressive increase in TgAb in consecutive follow-up exams. Structural recurrence required evidence of disease confirmed by cytology or histology, or conclusive findings from ultrasound, cross-sectional images, RAI whole-body scans or fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) (4). Other data obtained from medical records included age, sex, TNM staging, extrathyroidal extension, multifocality, vascular invasion, histological changes, thyroid capsule invasion, positive ink margins, lymph node involvement, extranodal extension, surgical extent, reoperative surgery, extent of lymphadenectomy, RAI administered activity, post-therapeutic whole-body scan results, and TSH, Tg, and TgAb levels.
Statistical analysis
A multivariate logistic regression model was used to identify the factors associated with the risk of recurrence. In addition, recurrence-free survival was estimated using the Kaplan–Meier method. The log-rank test was used to compare bivariate survival functions. Cox proportional hazard regressions were used to assess the risk associated with recurrence. Hazard ratios (HR) and confidence intervals (CI) were calculated in the model, and the proportionality assumption was evaluated by the Schoenfeld residual analysis. The multivariate models included variables that were significant in the bivariate analysis and those that were clinically relevant according to the literature and/or expert opinions. The analyses were performed using Stata v11.2 (StataCorp, College Station, TX).
Results
Patients
A total of 441 patients were identified with intermediate-risk papillary thyroid cancer and extent of disease between T2N1 and T3N1. Of these, 52 (11.7%) cases were excluded because they were lost to follow-up before response to therapy was determined. Of the 389 remaining patients, an excellent response was documented in 217 (56%), which constituted the study cohort. Patient and tumor characteristics are described in Table 1. Most of the patients were females (93.1%). The average age was 51 ± 11.8 years, and the most common tumor features were size ≤2 cm (68.2%), microscopic extrathyroidal extension (90.8%), and involvement of the central lymph nodes (59%). Few cases of aggressive histological variants (6%) or vascular invasion (1.8%) were documented. All of the patients were treated with total thyroidectomy (86.2% with prophylactic central neck dissection) and RAI therapy (100–150 mCi). Overall, 118 (54.4%) patients had an initial surgery performed in a non-specialized institution before referral to the authors' center. Most of these surgeries were total thyroidectomies performed by competent surgeons. Twenty such patients plus one of the authors' own required a reoperation, either because of an initially partial surgery (2 lobectomies and 11 hemithyroidectomies) or a postoperative diagnosis of residual disease in lateral neck lymph nodes (n = 8) after total thyroidectomy (including a patient initially operated in the authors' center).
rhTSH, recombinant human TSH; TSH, thyrotropin; Tg, thyroglobulin; SD, standard deviation.
Outcomes
The median follow-up time for the whole cohort was 42 months (range 17–88 months; interquartile range 35 months). Disease recurrence was documented in 16 (7.4%) cases, as shown in Table 2. The recurrence was structural in 10 (62.5%) cases, nine of them in cervical lymph nodes outside the initial surgical field and the last one in the soft tissues of the thyroid bed. Nodal recurrences were treated with lymphadenectomy in eight patients (followed by RAI therapy in five patients). One patient died before surgery due to an unrelated cardiac event. Soft-tissue local recurrence was treated with RAI therapy. At the last follow-up, five patients with structural recurrence had been rendered disease free (including the patient with local recurrence), whereas four had persistent disease (three structural and one biochemical persistence). Six (37.5%) patients were diagnosed with a biochemical recurrence. One of them was treated with empiric RAI therapy but 40 months later displayed FDG-avid structural progression in neck lymph nodes. Two additional patients further progressed to structural recurrence (one in the thyroid bed and one in the lungs). Both received a second dose of RAI. At the time of final follow-up, they were still under surveillance awaiting evaluation in terms of response to treatment. Of the three remaining patients, two displayed persistently detectable Tg levels (suppressed/stimulated Tg levels: 0.04/1.95 ng/mL and 2.11/25.4 ng/mL) with no evidence of structural disease, and the other was lost to follow-up.
Final status at last follow-up checkpoint (December 2016).
Tg (off), pre-ablation TSH-stimulated Tg value (ng/mL); RAI, radioactive iodine; NED, no evidence of disease; BED, biochemical evidence of disease; SED, structural evidence of disease; D, death from unrelated causes.
Multivariate logistic regression model
Multivariate analysis included variables that displayed a p-value of <0.20 in bivariate analyses, that is, tumor size (p = 0.059), TNM lymph node staging (p = 0.011), pre-ablation stimulated Tg value (p = 0.032), and lateral neck RAI uptake in post-therapy whole-body scans (p = 0.007). Backward elimination and stepwise regression was applied with an input probability of p < 0.05. Prognostic factors for recurrence (p < 0.05) were pN1b involvement, pre-ablation Tg >10 ng/mL, and lateral neck RAI uptake (Table 3).
OR, odds ratio; CI, confidence interval.
Cox regression model
Cox analysis included variables that displayed a p-value of <0.20 in bivariate analyses, that is, tumor size (p = 0.128), TNM lymph node staging (p = 0.001), use of rhTSH (Genzyme, Cambridge, MA; p = 0.062), pre-ablation stimulated Tg value (p = 0.062), and lateral neck RAI uptake in post-treatment whole-body scans (p = 0.003). Prognostic factors of recurrence were pN1b involvement and lateral neck RAI uptake (Table 4 and Fig. 1). The chi-square test used to test for non-proportionality of hazards in the Cox model showed non-violation of the assumption (p = 0.6685). Schoenfeld residual plots were made for each variable included in the model. There was no violation of the proportionality hypothesis (p = 0.6322 for N1b and p = 0.9168 for lateral neck RAI uptake).
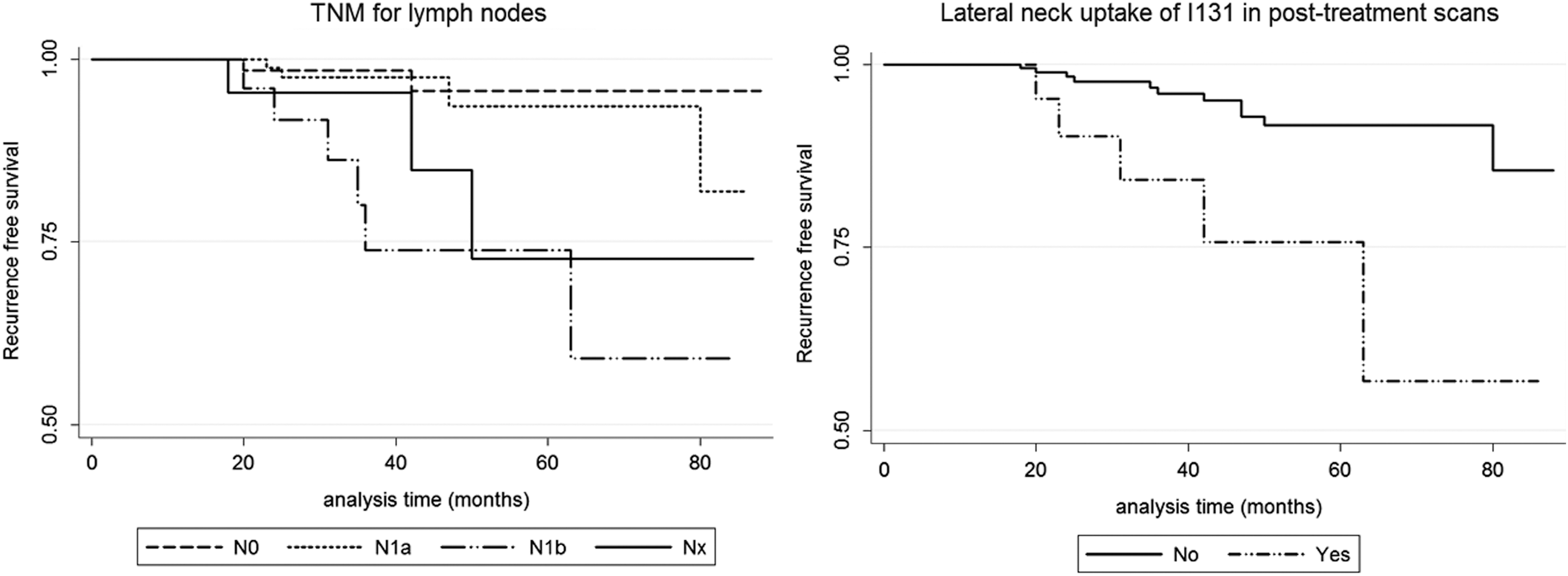
Survival curves based on TNM lymph node staging and lateral neck uptake of 131I in post-therapy whole-body scans.
HR, hazard ratio.
Recurrence-free survival
Kaplan–Meier recurrence-free survival could not be estimated for 50% of the cohort due to the infrequent occurrence of the event. The incidence density was 1.97 events per 100 person-years [CI 1.20–3.21]. Recurrence-free survival at three years was 94.7% (range 18–80 months; median = 36 months). Patients who were recurrence-free as of December 2016 and those who were lost to follow-up were censored, since their status could not be established.
Discussion
In a strictly clinical sense, a true recurrence is defined as biochemical or structural identification of disease in a patient previously thought to have no clinical evidence of disease (NED) following treatment (12). Nevertheless, according to our results, some patients with NED may in fact harbor unrecognized microscopic persistent disease that may go undetected at the time of response to treatment assessment only to be diagnosed months later upon progressing to a macroscopic scale or after reaching the threshold of clinical detection (8,13). Patients with DTC that achieve clinical remission after initial treatment have a low risk of long-term recurrence, regardless of their initial risk stratification (4 –7). In the series by Tuttle et al., the few recurrences that occurred after an excellent response to initial therapy were diagnosed between 4 and 11 years after initial treatment (4). In the present study, the rate of recurrent disease after a period of NED was 7.4%, which is higher than expected for a relatively short median follow-up of 42 months, raising the question about the existence of occult (i.e., persistent) disease since the onset (8,13). Incomplete tumor resection is a prognostic factor associated with high risk of recurrence (1). In fact, early reoperations within months of the initial thyroidectomy most likely reflect persistent rather than recurrent disease (13). Twenty-one patients required reoperations either for completion thyroidectomy or dissection of previously unrecognized involved lymph nodes. Recurrent disease was eventually documented in three (14%) of these patients. Reoperations are technically demanding because of the need to dissect on scarred and fibrotic tissue where anatomical planes have been altered by the initial surgery. They have a higher risk of complications (12) and have been independently associated with all-cause and disease-specific mortality (13). Nonetheless, this variable did not reach significance in the multivariate analyses, maybe because of the small sample size.
Establishing an excellent response is not always straightforward, especially in retrospective studies, where not all biochemical examinations are performed in the same center and may not be comparable. Tg antibodies can affect Tg measurements (14), whereas ultrasound findings are not always specific and results from FNA are not always conclusive. Even after obtaining negative biochemical and imaging results at predetermined time points (usually first 24 months after initial therapy), there is still a chance that persistent disease may go undetected.
Two very closely related variables, tumor involvement of the lateral neck lymph nodes and lateral neck RAI uptake in post-treatment scans, were significantly prevalent in the multivariate analysis in both the logistic and the Cox regressions. In addition, the multivariate logistic regression model established a statistically significant association between tumor recurrence and pre-ablation stimulated Tg >10 ng/mL (Tables 2 and 3).
Meer et al. reported that lateral neck lymph node involvement is a prognostic factor for recurrent disease (15). Other authors found that not only the localization but also the number and size of positive lymph nodes, the presence of extranodal extension, and the size of the tumor focus are prognostic factors that influence the risk of recurrence (16,17). These factors have recently been incorporated into the 2015 ATA guidelines (18), but they could not be assessed in this study.
Lateral neck RAI uptake in post-treatment scans is almost invariably associated with residual tumor in neck lymph nodes or soft tissue. Nevertheless, the effectiveness of RAI therapy in this scenario is unreliable and less effective for macroscopic residual lymph node metastases (19,20). The recent introduction of hybrid single photon emission computed tomography/CT images has helped to clarify the role of RAI therapy to treat lymph node metastases (21,22). Schmidt et al. (21) addressed the relationship between the size of involved lymph nodes and the success rate of RAI therapy. They found that 94% of RAI-avid nodal metastatic deposits <0.9 mL were successfully eliminated by radioiodine.
Pre-ablation Tg (i.e., quantitated approximately 30 days after surgery) has been found to be an important predictor of recurrence for patients with DTC (23 –29). Park et al. reported that patients with a pre-ablation Tg ≥10 ng/mL were 25.5 times more likely to experience therapeutic failure than those with a Tg <10 ng/mL ([CI 5.43–119.60]; p < 0.001) (23). In a recent meta-analysis, Webb et al. (24) found a positive predictive value (PPV; or probability of having persistent disease) of only 47% for a pre-ablation Tg >10 ng/mL (24). This seemingly low PPV can be explained by the fact that normal remnant thyroid tissue, present in nearly all patients, continues to synthesize and release Tg after thyroidectomy. On the contrary, patients with postoperative pre-ablation Tg values <10 ng/mL only had a 6% likelihood of having persistent disease (24). In fact, 85% of our patients had a pre-ablation Tg <10 ng/mL.
Limitations of this study include its retrospective nature and a short duration of follow-up. A median follow-up of 42 months may be too short because most true recurrences are expected to occur after the first five years in patients with an excellent response. An effort was made to control information bias through a meticulous data collection process conducted by only one researcher. By following a pre-established treatment protocol (11), it was possible to obtain uniform records of patient staging, treatment, and follow-up. Only patients who had an excellent response to initial treatment were included in order to compensate for differences in diagnostic, therapeutic, and TNM staging procedures, a common situation during the first two years, especially if not all procedures are performed in the same institution. Nevertheless, patients with a higher risk of recurrence may have inadvertently been enrolled; this could partially explain the high recurrence rate in this study. The 2015 ATA guidelines (18) state that patients with at least one involved lymph node >3 cm should be stratified as high risk. The present cohort included patients treated between January 2009 and December 2013. So, risk stratification and management decisions were made according to the 2009 ATA guidelines (1). Some of the newer recommendations, such as the size of metastatic deposits, did not consistently appear in histopathology reports before 2016. Therefore, some N1 patients with nodal macrometastases (≥3 cm) might have been downstratified, and some N1 patients with five or fewer micrometastases (<0.2 cm) might have been upstratified as intermediate risk. To reduce heterogeneity, the entire spectrum of intermediate-risk patients was purposely not included—only those with greater extent of disease (between T2N1 and T3N1b). Patients with TgAb levels <60 ng/mL were included in the response to treatment analysis (6), and this might have induced some falsely undetectable serum Tg levels (14). Loss of some patients during follow-up could not be controlled because they were referred to other institutions by their health insurance companies. Possible confounding biases were controlled for by the multivariate logistic regression and Cox regression analyses in accordance with the available literature. The final proposed models were adjusted to the data that were obtained, as seen in the analyses of the diagnostics and validations performed for each model. Since the final sample size was smaller than expected, a type II error may have occurred, as shown by the amplitude of the models' confidence intervals. Consequently, variables such as pre-ablation stimulated Tg >10 ng/mL that did not reach statistical significance in the Cox regression model might have proved significant in a larger sample size. Some of intermediate-risk variables, such as aggressive histological variants, vascular invasion, and extranodal extension, could not be analyzed due to their infrequent occurrence.
In conclusion, the observed early recurrence rate of 7.4% is uncharacteristically high for a population of patients who had an excellent response to initial treatment. The significant association found between recurrent disease and lateral neck lymph node metastasis, lateral neck RAI uptake in post therapy whole-body scan, and pre-ablation Tg levels >10 ng/mL may indicate that the so-called early recurrences may in fact be due to unrecognized occult residual, regional, or micrometastatic disease that enlarges to reach the threshold of clinical detection (12,13).
Footnotes
Acknowledgments
We thank Dr. Alfredo Romero and Dr. Felipe Fierro for their collaboration in the definition of specific variables and other important concepts. This study was funded with resources provided by the Instituto Nacional de Cancerología.
Author Disclosure Statement
No competing financial interests exist.