
Abstract
Background:
Tyrosine kinase inhibitor (TKI)-induced thyroid dysfunction is recognized as a common adverse effect of treatment, but the importance of incident hypothyroidism during TKI therapy remains unclear. This study analyzed the prognostic significance of hypothyroidism during TKI therapy in cancer patients.
Methods:
This was a retrospective cohort study of adult patients with advanced nonthyroidal cancer treated with TKI and available thyroid function testing at three affiliated academic hospitals from 2000 to 2017. Patients with preexisting thyroid disease were excluded. Demographic, clinical, and cancer treatment data were collected. Thyroid status with TKI treatment was determined from thyroid function testing and initiation of thyroid medication, and classified as euthyroid (thyrotropin [TSH] normal), subclinical hypothyroidism (SCH; TSH 5–10 mIU/L, or higher TSH if free thyroxine normal), or overt hypothyroidism (OH; TSH >10 mIU/L, low free thyroxine, or requiring replacement). Multivariate models were used to evaluate the effect of TKI-related hypothyroidism on overall survival (OS).
Results:
Of 1120 initial patients, 538 remained after exclusion criteria. SCH occurred in 72 (13%) and OH in 144 (27%) patients with TKI therapy. Patients with hypothyroidism had significantly longer OS, with median OS in euthyroid patients of 685 days [confidence interval (CI) 523–851] compared to 1005 days [CI 634–1528] in SCH and 1643 days [CI 1215–1991] in OH patients (p < 0.0001). After adjustment for age, sex, race/ethnicity, cancer type, cancer stage, ECOG performance status, and checkpoint inhibitor therapy, OH remained significantly associated with OS (hazard ratio = 0.561; p < 0.0001), whereas SCH did not (hazard ratio = 0.796; p = 0.165). Analysis of hypothyroid patients (SCH and OH) with TSH >5 and <10 mIU/L stratified by hormone replacement status showed improved survival associated with hormone replacement.
Conclusions:
New hypothyroidism in cancer patients treated with TKI is associated with significantly improved OS, should not necessitate TKI dose reduction or discontinuation, and may provide independent prognostic information.
Introduction
T
Several observational studies have even suggested clinical improvement in patients who develop hypothyroidism while on TKI. In a retrospective study of 65 patients with renal cell carcinoma (RCC), hypothyroidism occurred in 25% of patients treated with TKI and was associated with significantly longer progression-free survival (PFS) and overall survival (OS) (3). Several other small studies in patients with RCC treated with sunitinib or sorafenib similarly demonstrated that hypothyroidism was correlated with greater treatment response rate and longer PFS and OS (4 –7). Whether these results are generalizable to other cancer types or to other TKI is unclear. Most existing data come from clinical trials of cancer therapy, which frequently include patients with preexisting thyroid disease and evaluate treatment with only a single TKI (1). In clinical practice, cancer patients are often treated with serial TKI and other cancer therapies over the course of their illness. The present study evaluated the association between new thyroid dysfunction and survival in the largest cohort to date of euthyroid TKI-treated patients with nonthyroidal cancer. Furthermore, patient survival by degree of thyroid dysfunction and treatment with thyroid hormone replacement was compared. In this study, a significant fraction of patients were treated with multiple TKI and other cancer therapies, more closely representing current clinical practice.
Methods
Patients and data collection
This was a retrospective cohort study of adult patients with advanced nonthyroidal cancer treated with common TKI and available thyroid function testing (TFT) at three Harvard Medical School–affiliated academic hospitals (Brigham and Women's Hospital, Dana Farber Cancer Institute, and Massachusetts General Hospital, Boston, MA), receiving first TKI treatment between August 2000 and August 2013. The Research Patient Data Registry enabled identification of patients with a cancer diagnosis, treatment with one of six common TKI (axitinib, pazopanib, regorafenib, sorafenib, sunitinib, or vandetanib), and any TFTs, originally described in Hamnvik et al. (8). This cohort of 1120 patients was further refined for the present study by exclusion of patients with thyroid cancer or nonmalignant tumors, as well as those with preexisting thyroid conditions (Table 1). Institutional Review Board approval was obtained (Partners Protocol 2014P001974). Patient electronic medical records were reviewed for all data and follow-up through May 2017. Data collected included patient demographics, cancer diagnosis, stage (American Joint Committee on Cancer criteria where applicable), Eastern Cooperative Oncology Group (ECOG) status, non-TKI therapy (including chemotherapy, VEGFR and checkpoint inhibitors), and date of death or last follow-up. The initial collection of patients was done by identifying patients treated with one of six common TKI, a cancer diagnosis, and TFTs, as described above. As is commonly seen clinically, many of these cancer patients were treated with other cancer therapies, including some TKI. Data on these other TKI and classes of therapy were gathered and are reported in this article. TKI in this study were not limited to those with known associations with hypothyroidism in order to allow newer TKI agents and those with possible associations that have not yet been identified to be included. Multiple mechanisms of TKI-related thyroid dysfunction have been postulated, and this remains an area of ongoing research. Additionally, TKI were not limited to those with VEGFR targets. In this retrospective study, the frequency with which different TKI were used was influenced by historical clinical practice and available TKI, including evolving clinical indications for TKI during the study period. TKI treatment data included each TKI name and dates received during the study period (approximated as the first of the month if not otherwise specified). Patients who underwent bone-marrow transplantation were excluded.
Categories are not mutually exclusive.
AML, acute myelogenous leukemia.
The thyroid function data collected included history of thyroid disease, treatment with thyroid hormone or antithyroid drugs, serum thyrotropin (TSH) and free thyroxine (fT4) levels, date of first thyroid abnormality, and highest serum TSH (before replacement) with TKI therapy. Thyroid peroxidase antibody (TPOAb) results were collected but were available in <1% of patients. Patients with preexisting thyroid dysfunction, including abnormal TFTs, a preexisting diagnosis of thyroid disease or use of thyroid medication, thyroid cancer, or prior thyroid resection, were excluded. Thyroid status with TKI treatment was determined from TFT and initiation of thyroid medication.
During treatment, patients were classified as euthyroid (TSH normal), subclinical hypothyroidism (SCH; TSH >5 and <10 mIU/L, or higher TSH if fT4 normal), or overt hypothyroidism (OH; TSH >10 mIU/L and low fT4 if available, or requiring thyroid hormone replacement). Incident hypothyroidism was defined as a persistent change from euthyroid to SCH or OH while on TKI or within six months of TKI therapy because of the nonstandard timing of TFT in this retrospective setting. Patients without TFT during and after therapy (i.e., TSH level) or in whom thyroid status before and during treatment could not reliably be determined were excluded. Additional details are provided in the Supplementary Methods (Supplementary Data are available online at
Statistical analysis
Baseline patient characteristics, including demographic and clinical variables, were assessed, and summary statistics were obtained, including mean and standard deviation for continuous normally distributed variables. Median and interquartile range (IQR) were used for continuous non-normally distributed variables, and number and percentage were used for categorical variables. The cumulative TKI exposure, median TKI treatment, number of non-TKI cancer treatments, and checkpoint inhibitor therapy were also evaluated in each group of patients (euthyroid vs. SCH vs. OH). For these two summary statistics, Student's t-test or the Mann–Whitney U-test for continuous variables and Pearson's chi-square test or Fisher's exact test for categorical variables were used.
OS was estimated using the Kaplan–Meier method. OS was defined from the onset of first TKI therapy until death or censor. Survival curves were compared between euthyroid and hypothyroid (SCH + OH) patients using a large-sample chi-square test (log-rank test). Baseline hazard function for OS was assessed using the Cox proportional hazard model after checking for the assumption of proportionality. Each baseline parameter was studied in a univariate model, and significant variables were included in the multivariate model. Sensitivity analyses performed comparing OS limited to only those patients who developed hypothyroidism within the first six months and the first year of treatment confirmed the primary analysis (data not shown). So, overall data were utilized for the final analyses. Hazard ratio (HR) and a two-sided p-value of <0.05 were used to indicate statistical significance. Analyses were performed using SAS v9.3 (SAS Institute, Cary, NC) and GraphPad Prism (GraphPad Software, Inc., La Jolla, CA). Figures were created using GraphPad Prism and Adobe Photoshop (Adobe Systems, San Jose, CA).
Results
From 1120 initial patients, 538 remained after applying the exclusion criteria. Hypothyroidism occurred in 215 (40%) patients with TKI therapy, including 71 (13.2%) with SCH and 144 (26.8%) with OH. Two (0.3%) patients only had follow-up TFT showing hyperthyroidism without additional available testing and were not included in analyses of hypothyroid groups, leaving 536 patients for the final analysis. Comparison of demographic factors and tumor type among euthyroid, SCH, and OH groups is shown in Table 2. The median age of patients who remained euthyroid was 60 years compared to 65.3 and 59.3 years in those who developed SCH or OH, respectively (p < 0.0001; age of SCH patients was significantly different from euthyroid and OH patients by pairwise comparisons). Women were more likely to become hypothyroid than men (94/178 [52.8%] vs. 121/358 [33.7%]; p < 0.0002). The incidence of hypothyroidism varied among cancer types in the study cohort (p < 0.0001), including a greater proportion of patients with RCC and gastrointestinal stromal tumors (GIST) in the OH group. There was no difference among euthyroid, SCH, and OH groups with relation to race/ethnicity, baseline AJCC Stage, or ECOG status.
Stage refers to the initial American Joint Commission on Cancer staging where applicable; ECOG PS refers to the Eastern Cooperative Oncology Group performance status.
Euthyroid vs. SCH.
SCH vs. OH.
Euthyroid vs. OH.
RCC, renal cell carcinoma; GIST, gastrointestinal stromal tumor; CNS, central nervous system; ND, no data; SCH, subclinical hypothyroidism; OH, overt hypothyroidism.
The median time from study entry to identification of thyroid dysfunction was 196 days (IQR 64–833 days) for SCH and 252 days (IQR 69.5–688.5 days) for OH patients. The median peak TSH in SCH patients was 6.5 mIU/L (IQR 5.9–7.7 mIU/L) compared to 12.9 mIU/L (IQR 10–22.7 mIU/L) in OH patients (peak prior to hormone replacement; p < 0.0001). Of patients who developed OH by the classification, 105/144 (72.9%) had TSH >10 mIU/L and 132/144 (91.7%) received thyroid hormone replacement initiated at the discretion of the treating physicians. For patients with TSH <10 mIU/L who received thyroid hormone replacement, TSH elevation was most often accompanied by nonspecific symptoms, including fatigue, depression, or declining functional status.
Patients in the study received 26 different TKI, with exposure reported as the total number of different TKI received and the number of days during which TKI treatment was received (Tables 3 and 4). In the overall cohort, 252/536 (47%) patients received more than one TKI during cancer treatment. For euthyroid patients, the median TKI exposure was 215 days (IQR 95–658 days), and the median TKI exposure preceding thyroid dysfunction was 195 days (IQR 63–586 days) in SCH patients and 202.5 days (IQR 61–518.5 days) in OH patients (p = 0.46).
Non-TKI cancer treatment received shown is more detail in Table 5.
Checkpoint inhibitors included anti-cytotoxic T-lymphocyte associated protein 4 (CTLA-4) or anti-programmed cell death protein 1 (PD-1) antibody therapy.
Euthyroid vs. SCH.
SCH vs. OH.
Euthyroid vs. OH.
Treatment with other classes of cancer therapy was compared across groups (Tables 3 and 5). The number of non-TKI cancer treatments received was not significantly different between euthyroid, SCH, and OH groups (p = 0.23). Patients with SCH or OH were more likely to have received checkpoint inhibitor therapy (e.g., nivolumab or ipilimumab) during the entire study period (p = 0.0004), but the proportion of patients who received checkpoint inhibitor therapy prior to thyroid abnormalities was similar between euthyroid patients (10/321), SCH (3/71), and OH (5/144) patients (p = 0.96). There was a trend (p = 0.09) toward more chemotherapy (e.g., alkylating agents, microtubule inhibitors, topoisomerase inhibitors, DNA replication inhibitors) in euthyroid compared with SCH or OH patients. Euthyroid patients received significantly more chemotherapy treatments compared to SCH + OH patients together (p = 0.04). The proportion of patients treated with mammalian target of rapamycin (mTOR) inhibitors (e.g., everolimus or temsirolimus), non-TKI VEGFR inhibitors (i.e., bevacizumab or ramucirumab), heat shock protein inhibitors, interleukin-2 or interferon, hormone therapy (e.g., sandostatin), phosphatidylinositol-4,5-bisphosphate 3-kinase inhibitors, and other therapies (e.g., cetuximab or rituximab) was not significantly different between euthyroid, SCH, and OH groups.
mTOR, mammalian target of rapamycin; VEGF, vascular endothelial growth factor; HSP, heat shock protein; IL, interleukin; PI3K, phosphatidylinositol-4,5-bisphosphate 3-kinase; other, treatments included anti-human epidermal growth receptor 2, cetuximab, rituximab, radium, anti-CD-137 antibody, kevetrin, figitumumab, metosanid, and anti-ENPP3 antibody.
OS benefit in patients who develop TKI-associated hypothyroidism
Analysis of OS by product limit survival estimates (Fig. 1) showed significantly longer median OS in patients with hypothyroidism (SCH or OH) compared to euthyroid patients, with a median OS of 1500 days (IQR 1109–1718 days) and 685 days [confidence interval 523–851], respectively (p < 0.0001). When stratified by degree of hypothyroidism, the difference remained significant among all groups, with a median OS of 1005 days (IQR 634–1528 days) in SCH patients and 1643 days (IQR 1215–1991 days) in OH patients (p < 0.0001).
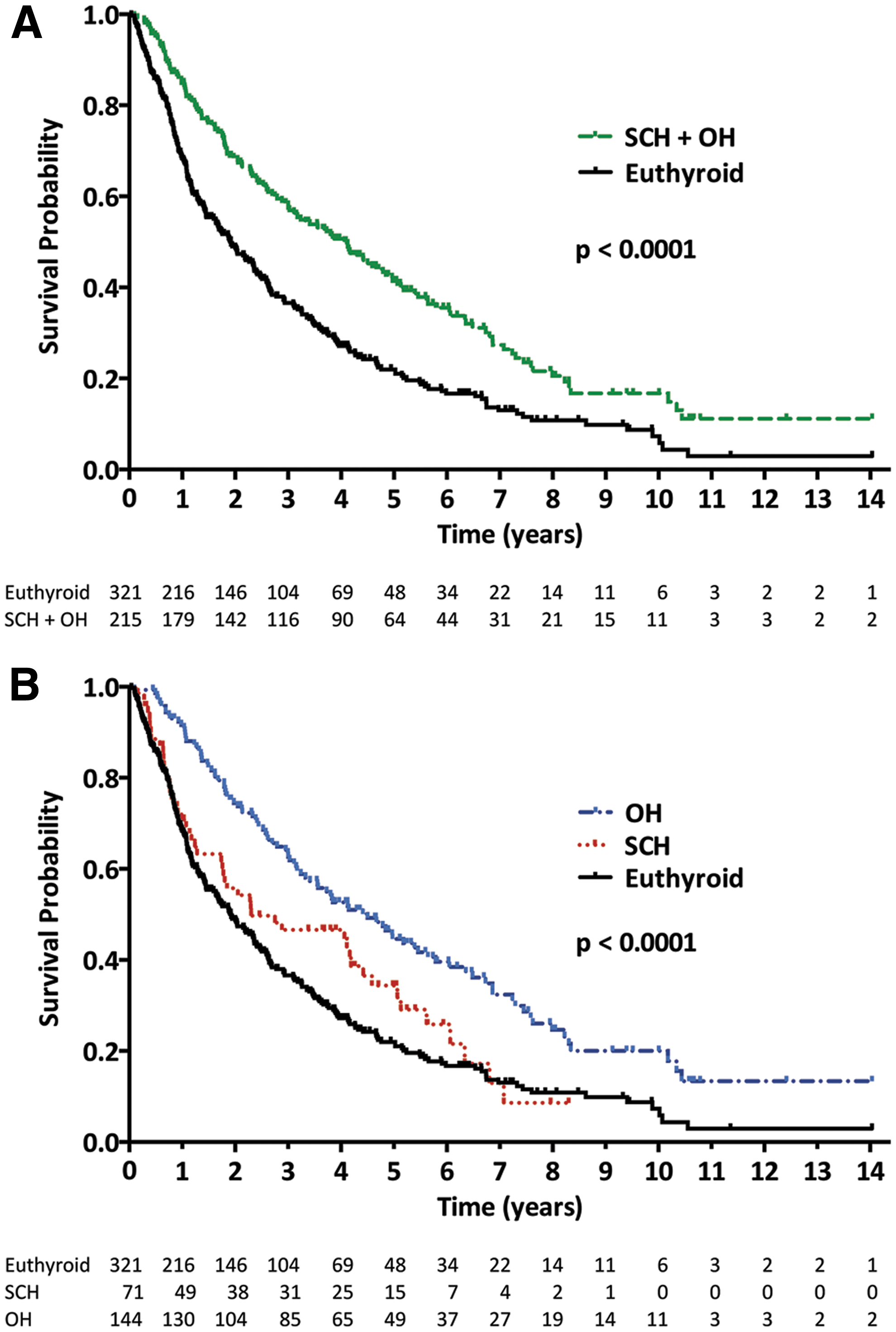
Overall survival (OS) in nonthyroidal cancer patients treated with tyrosine kinase inhibitors (TKI) is significantly greater in those who develop hypothyroidism. OS curves are showed as product limit survival estimates, with number of patients at risk. (
Using the Cox proportional hazards model, age, sex, race/ethnicity, cancer type, cancer stage, ECOG performance status, checkpoint inhibitor therapy, non-TKI VEGFR inhibitor therapy, and thyroid status were evaluated as clinical predictors of OS in the study population, as shown in Table 6. Development of OH was associated with longer OS (HR = 0.523; p < 0.0001), while SCH only showed a trend toward longer OS (HR = 0.754; p = 0.078). Increasing age (HR = 1.016; p = 0.0005) and Hispanic race/ethnicity (HR = 1.978 compared to white race/ethnicity; p = 0.034) were both associated with worse OS, while checkpoint inhibitor treatment and lower baseline ECOG performance status were associated with better OS. Compared to RCC as the reference cancer type, patients with GIST had longer OS, and those with hepatocellular carcinoma, sarcoma, and other carcinomas had significantly shorter OS. Sex and non-TKI VEGFR inhibitor treatment were not significantly associated with OS. Cancer stage also was not significantly associated with OS in this cohort, likely reflecting the predominance of advanced stage disease (96.3% of patients in the cohort had stage III/IV disease, with no significant difference among groups).
Cancer stage = American Joint Commission on Cancer, where applicable. Checkpoint inhibitors included anti-cytotoxic T-lymphocyte Associated protein 4 (CTLA-4) or anti-programmed cell death protein 1 (PD-1) antibody therapy. VEGFR inhibitors included bevacizumab and ramucirumab.
HR, hazard ratio; CI, confidence interval.
A multivariate analysis for variables associated with OS inclusive of the clinical parameters significant in the univariate analysis demonstrated that OH was independently associated with OS (HR = 0.561; p < 0.001), whereas SCH was not (HR = 0.796; p = 0.165). Increasing patient age was independently associated with shorter OS (HR 1.019; p < 0.0001). Factors independently associated with longer OS include low ECOG score (HR >1 with p < 0.0001 for all ECOG performance status > 0), and checkpoint inhibitor therapy (HR = 0.412; p < 0.0015). Compared to RCC, GIST was associated with longer OS (HR = 0.549; p = 0.0009), while sarcoma and other carcinomas were associated with shorter OS (HR = 2.196, p < 0.0001, and HR = 1.764, p = 0.017).
Thyroid hormone replacement and OS in patients with TSH >5 and <10 mIU/L
While current recommendations support thyroid hormone replacement for OH and selected cases of SCH (1,9), untreated hypothyroidism with elevated TSH has been proposed as a beneficial state in cancer patients (10). Analysis of hypothyroid patients (SCH and OH) with TSH >5 and <10 mIU/L showed that those treated with hormone replacement did not have a worse OS (Fig. 2). Additional analysis of OS stratified by TSH level (SCH and OH combined) showed no significant difference between patients with TSH >10 or TSH <10 mIU/L (p = 0.78).
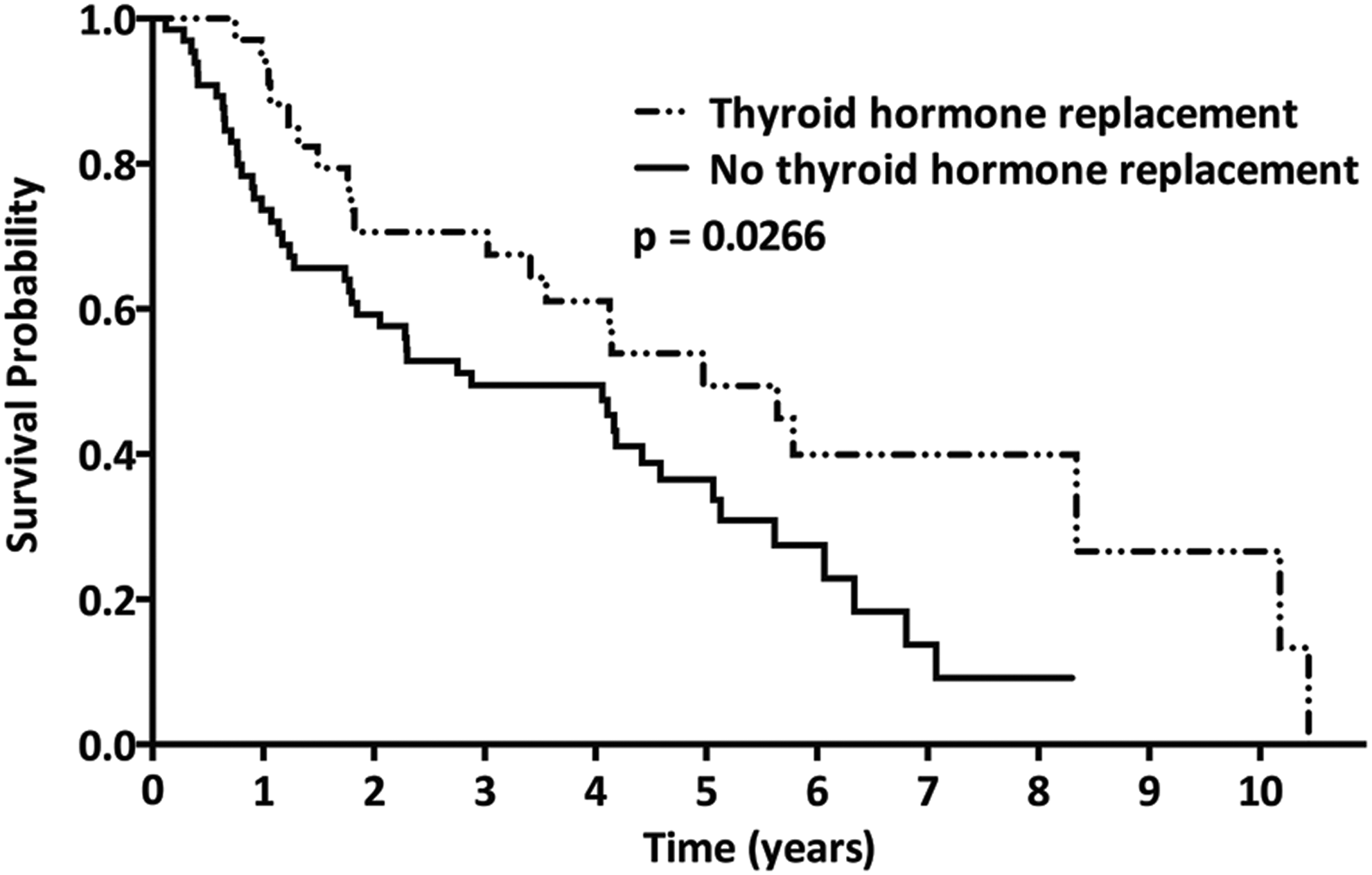
OS in hypothyroid patients with thyrotropin (TSH) >5 and <10 mIU/L who did and did not receive thyroid hormone replacement. Survival curves shown for patient with TSH >5 and <10 mIU/L during TKI treatment. For patients in this TSH range, those who received thyroid hormone therapy (dot-dot-dash line) had significantly greater OS compared to those who did not receive thyroid hormone replacement (solid line; median 1815 days vs. 1052 days; p = 0.0266).
Discussion
This study presents an analysis of TKI-related thyroid dysfunction and its relation to survival in what is, to the authors' knowledge, the largest cohort to date of initially euthyroid patients treated for nonthyroidal cancers. The data demonstrate an improvement in OS among TKI-treated patients who develop OH compared to those who remain euthyroid, and OH remained independently associated with OS after adjustment for relevant demographic, cancer diagnosis, and treatment parameters.
These data extend findings from prior smaller studies suggesting better clinical outcomes in patients who develop TKI-related thyroid dysfunction (3 –6). In a retrospective review of four clinical trials pooling 197 patients who received at least one TKI, patients who developed hypothyroidism were more likely than euthyroid patients to have clinical benefit, defined as complete response, partial response, or stable disease for four months, after adjustment for age, tumor type, and sex (odds ratio = 2.9 [CI 1.3–6.5]) (7). This study excluded patients with preexisting thyroid disease, but was limited by few details regarding TKI drugs received or degree of thyroid abnormality. Currently, a survival benefit is similarly demonstrated in patients developing hypothyroidism in a larger cohort with longer follow-up and incorporating differences in TKI and non-TKI cancer treatments between hypothyroid and euthyroid patients.
No data were found to suggest a benefit in withholding levothyroxine hormone replacement within TKI-treated patients who develop hypothyroidism, as has been suggested in previous reports (10). Thyroid hormone replacement in patients with mild thyroid elevations (TSH >5 and <10 mIU/L) was not associated with a worse survival, suggesting that this may be safely done in TKI-treated cancer patients when hypothyroidism occurs. This is in agreement with the report by Riesenbeck et al. (5) showing longer PFS with hypothyroidism and no influence from levothyroxine hormone replacement. The current retrospective study, initiation of thyroid hormone replacement was determined by the treating clinician and occurred at variable TSH elevations and symptom thresholds. It is possible that this mild degree of hypothyroidism in untreated patients was insufficient to demonstrate a survival benefit for the hypothyroid state.
Potential mechanisms behind the association between TKI-related hypothyroidism and survival in cancer patients are unknown. Successful inhibition of certain tyrosine-kinase pathways may adversely affect thyroid and malignant cells similarly. Peak or average drug concentrations may lead to thyroid damage and have important implications for antineoplastic effectiveness of TKI. Immune-mediated thyroiditis is another proposed mechanism by which TKI-related thyroid dysfunction occurs (1,11 –13). A pattern of thyroiditis—thyrotoxicosis followed by hypothyroidism—has been observed in some cases of TKI-associated thyroid dysfunction, and this biphasic pattern was observed in 18 (12.5%) patients with TKI-related hypothyroidism, though the nonstandard timing of TFT assessment in this retrospective study precludes knowing the precise frequency of this pattern. The greater incidence of TKI-related hypothyroidism with female sex, a well-established risk factor for autoimmune thyroid disease, and the lack of correlation with cumulative TKI exposure also support a role for autoimmunity (14).
Immunotherapies activate the immune system to attack cancer cells and can cause autoimmune reactions as a collateral effect of successful reversal of tumor-mediated immune tolerance (15). Such immune-related adverse events (irAEs) have been shown to correlate with improved clinical response to immunotherapy (16 –18). Thyroiditis is one of the most common irAEs seen with cancer immunotherapy and has been proposed as one mechanism by which TKI may cause hypothyroidism (1,6,19). In a prospective study of 27 patients with advanced cancer, Pani et al. demonstrated new TPOAb positivity in 25% of TKI-treated patients and longer PFS in this subset (11,12). Improved survival concurrent with the development of thyroid dysfunction in TKI-treated cancer patients supports a possible relationship between the induction of thyroid autoimmunity during therapy and a systemic immune response to cancer.
There are several limitations to the current study. As a retrospective cohort analysis, findings are associative and cannot demonstrate causality. Thyroid monitoring and treatment were not pre-specified and were at the discretion of the treating physician, representing a potential source of selection bias and preventing identification of the exact timing and degree of thyroid dysfunction. Exclusion of patients without TFTs performed is a source of possible selection bias. Though analysis demonstrated no significant differences in baseline characteristics to suggest that excluded patients were preferentially more likely to have a poorer prognosis, there remains the possibility that there was an association between unmeasured thyroid status and survival in excluded patients. The possibility that TKI type or exposure confounds the relationship between hypothyroidism and survival cannot be excluded and may require more detailed prospective analysis. It is acknowledged that in this retrospective study, the frequency with which different TKI were used was influenced by historical clinical practice and available TKI. The survival benefit was shown as OS rather than cancer-specific treatment response or survival because while the vast majority of subject deaths could be attributed to the underlying cancer by review of the medical record, acute causes of death, such as sepsis or respiratory failure, could not always be distinguished from cancer progression leading to use of OS as the primary outcome. This study provides a novel evaluation of the relative frequencies of multiple classes of cancer treatment (e.g., chemotherapy or mTOR inhibitors) and the number of unique treatments received, but the great variety of treatments employed precluded a systematic analysis of specific exposure to each non-TKI therapy. It is notable that despite their longer survival, hypothyroid patients received no more and perhaps less chemotherapy than euthyroid patients (Table 5), suggesting that more non-TKI cancer therapy was not a significant driver of their longer OS.
The strengths of this study are the large cohort size of euthyroid patients, preventing confounding by previous thyroid dysfunction, and the analysis and adjustment for important clinical and treatment variables not well assessed in previous studies. In conclusion, these findings suggest that new thyroid dysfunction with TKI therapy may predict good prognosis and should not necessitate TKI dose reduction or discontinuation. To understand this association further, additional prospective and mechanistic studies of TKI-related hypothyroidism are warranted.
Footnotes
Author Disclosure Statement
None of the authors has any relevant disclosures for this work.