
Abstract
Background:
This study aimed to characterize the frequency of self-reported thyroid-related impaired sex life in patients with thyroid diseases, to examine its clinical correlates and relationship with overall quality of life (QOL), and to investigate the effect of treatment.
Patients and Methods:
Two separate patient samples with benign thyroid diseases were investigated: a cross-sectional sample (759 women and 118 men) treated at two Danish university hospital outpatient clinics, in 2007–2008, and a longitudinal sample (358 women and 74 men) undergoing treatment at the abovementioned centers, during 2008–2012, evaluated before and 6 months after therapy. The thyroid-specific QOL questionnaire ThyPRO was used to measure patient-evaluated thyroid-related sex life impairment. Biochemical and clinical variables were analyzed (i.e., age, education, degree of thyroid dysfunction, comorbidity, serum thyrotropin, total thyroxine, and triiodothyronine, as well as thyroperoxidase and thyrotropin receptor antibody concentrations). The SF-36 Health Survey was used to analyze the effect of impaired sex life on overall QOL.
Results:
In the cross-sectional sample, 36% of women and 31% of men reported what they perceived to be thyroid-attributable impaired sex life. Women with autoimmune thyroid diseases reported more impairment than those with non-autoimmune thyroid diseases. In patients with Graves' disease lower levels of educational attainment and in patients with toxic nodular goiter comorbidities were associated with impaired sex life. Overall QOL was lower in patients with thyroid-related sex life impairment. In the longitudinal sample, 42% of women and 33% of men had impaired sex life at baseline, which improved at 6 months follow-up only in women and, when analyzing individual diagnoses separately, statistically significantly among those with autoimmune hypothyroidism. Sexual impairment was associated with low education in patients with toxic nodular goiter and with high plasma triiodothyronine concentrations in patients with Graves' disease. In autoimmune hypothyroidism, a younger age was associated with sex life impairment.
Conclusion:
We found a high frequency of self-reported, thyroid-related sex life impairment in patients with benign thyroid diseases, especially in young women with autoimmune thyroid diseases. Self-perceived impaired sex life persisted in women treated for Graves' disease, suggesting that normalization of thyroid function was not sufficient to restore sexual function.
Introduction
B
Previous studies have focused on the influence of thyroid dysfunction or autoimmunity on sex life, but its impairment in patients with non-toxic nodular goiters has been investigated in only one study including 19 females (9). More women with nodular goiter had sexual dysfunction than those with hyper- or hypothyroidism, or Hashimoto's thyroiditis (9). Also, only a few studies have addressed whether therapy restores sex life in thyroid patients (8,14). Sexual function improved but was not normalized after restoration of thyroid function in females with hypo- and hyperthyroidism (8).
Since the prevalence of thyroid diseases is relatively high and the majority of patients need life-long therapy, the identification of sexual problems and their clinical correlates is relevant. The aims of the present study were to describe the frequency of self-reported, thyroid-related impairment in sex life in two large samples of patients with benign thyroid diseases, to examine the relationship with clinical variables and overall QOL, and to investigate the effect of treatment on the improvement of sexual quality of life in a longitudinal study.
Methods
Patient populations
Data from two separate and previously described patient populations were used. These were multipurpose samples, previously utilized for validation of ThyPRO multi-item scales (not reported here) as well as for descriptive purposes, as in this study.
The cross-sectional sample (n = 877, response rate 69%) comprised patients with thyroid diseases followed at or referred to two university hospital outpatient clinics (Copenhagen University Hospital Rigshospitalet and Odense University Hospital, Denmark), in 2007–2008 (15). This sample comprised patients with newly diagnosed thyroid disease as well as patients controlled for ongoing treatment.
The longitudinal sample (n = 432, response rate 80%) comprised patients undergoing treatment for thyroid diseases at the abovementioned centers in 2008–2012, evaluated prior to and 6 months after treatment (16).
The samples are described in Table 1. Patients were classified into five mutually exclusive diagnostic groups based on their clinical status at the time of diagnosis: nontoxic goiter, toxic nodular goiter, Graves' hyperthyroidism (without orbitopathy), Graves' orbitopathy, and autoimmune hypothyroidism.
Data are in number (percent) if not otherwise specified. In the longitudinal sample, sociodemographic data, including age, are at baseline.
Interquartile range.
Questionnaires
All patients completed the thyroid-related quality of life measure ThyPRO, which evaluates the influence of thyroid disease on physical, mental, and social symptoms, functioning and well-being, including sex life. It consists of 85 items, summarized in 13 multi-item and one single-item scale. Each item is asked with a 4-week recall period and has five response options, ranging from “not at all” to “very much.” The 13 multi-item scales are constructed by summation of relevant items and subsequent transformation to the range 0–100, with higher scores indicating more symptoms and impact on QOL. The single-item Overall QOL impact is also linearly transformed to the range 0–100. The wording of the latter is, “During the past 4 weeks, has your thyroid disease had a negative effect on your quality of life?”. ThyPRO has been extensively validated and is available in multiple languages (2,17
–25) (see Supplementary Data; Supplementary Data is available online at
Sociodemographic data and data on comorbidity were self-reported. In the longitudinal sample, data at baseline are presented. Information about comorbidity was obtained in accordance with the guidelines of the Danish National Institute of Public Health using a list of prespecified chronic conditions, supplemented by an open-ended question on other nonthyroid diseases (27).
Identification and quantification of impaired sex life due to thyroid disease
Impaired sex life due to thyroid disease was identified by item 10a of ThyPRO: “During the past 4 weeks, have you felt your thyroid disease had a negative influence on your sex life?” Patients responding positively to this question, at any level, were categorized as experiencing impaired sex life due to thyroid disease.
Correlates of Impaired Sex Life scores
Relationships between sociodemographic and clinical variables and impaired sex life were evaluated separately in each diagnostic group. This was performed by regressing clinical variables on the ThyPRO Impaired Sex Life scale, using multiple linear regressions. Relationships with age and education were estimated separately. Relationships with clinical variables were controlled for age and education. The framework for interpretation of effects was in accordance with Cohen: small difference, 4–10; moderate difference, 10–16; and large difference, >16 (28).
The following variables were evaluated in the cross-sectional sample: duration of disease, degree of thyroid dysfunction (euthyroid, subclinical. and overt hypo- and hyperthyroidism, respectively) at the time of diagnosis as well as at the time of measurement, being untreated for thyroid disease at time of measurement, self-reported comorbidity (operationalized as no vs. some comorbidity), serum TSH, total thyroxine (T4), total triiodothyronine (T3), and TPO-Ab and TSH receptor autoantibody (TR-Ab) concentrations.
In the longitudinal sample, sociodemographic and clinical variables at baseline were regressed on ThyPRO Impaired Sex Life scores at baseline and at follow-up as well as on changes in Impaired Sex Life scores between baseline and follow-up. Further, clinical variables at follow-up were regressed on Impaired Sex Life scores at follow-up. Thus, prediction of Impaired Sex Life at baseline was attempted predicted by clinical variables at baseline, as was change in Impaired Sex Life score as well as Sex Life score at follow-up; in addition, predictions of Impaired Sex Life scores at follow-up were also attempted using clinical variables at follow-up.
The following variables were analyzed at baseline and follow-up: age, education, degree of thyroid dysfunction (see above), comorbidity, serum-TSH, total T4, total T3, and TPO-Ab concentrations.
Effect of impaired sex life on measures of overall QOL
Impaired sex life (yes/no) was regressed on SF-36 Mental Component Summary and Physical Component Summary scores, as well as on the ThyPRO Overall QOL-impact scale, controlling for age and education. The framework for interpretation of effects was in accordance with Cohen (effect size 0.2–0.5, small; 0.5–0.8, moderate; and >0.8, large): MCS and PCS: small difference 2–5, moderate difference 5–8, large difference >8; ThyPRO Overall QOL-impact scale: small difference 4–10, moderate difference 10–16, large difference >16 (28).
Statistical analyses
Statistical analyses were performed using SAS (29). All analyses were performed separately for each gender and diagnostic group. Due to the low number of men in the samples, prediction of impaired sex life scores and analyses of effect of impaired sex life on overall QOL were only conducted among women.
Gender differences were tested by Fisher's exact test and differences according to diagnostic groups used estimations and tests of predicted population margins. Changes in the frequency from baseline to follow-up were evaluated by McNemar's test. The statistical significance level was set to p < 0.05 and a specific effect was only considered significant, if the F-test of the overall model as well as the type II sum of squares test of the variable was also significant. Prediction of Impaired Sex Life scores by clinical variables was analyzed using multiple linear regression controlling for age and education, as were the tests for differences in overall QOL between patients with and without impaired sex life.
Results
Frequency of impairment in sex life due to thyroid disease
In the cross-sectional sample, a third of patients experienced what they perceived to be impaired sex life (women, 36% [CI 32–40]; men, 31% [CI 22–41]) (Table 2). No gender differences were observed. In men, the diagnostic subgroups were too small for subgroup analyses. In women, patients with non-autoimmune diseases (nontoxic and toxic nodular goiter) had less impairment than patients with autoimmune thyroid disease (Fig. 1). In the longitudinal sample, 42% [CI 37–48)]of women and 33% [CI 22–44] of men reported what they perceived to be impaired sex life at baseline. In women, this proportion declined significantly to 34% [CI 29–40] at six months follow-up, whereas no change was observed in men (Fig. 2). At baseline, a significantly larger proportion (57% [CI 44–70] of women with Graves' hyperthyroidism experienced impaired sex life, compared with women with non-toxic goiter. At follow-up, no statistically significant difference between diagnostic groups was observed (Table 2).
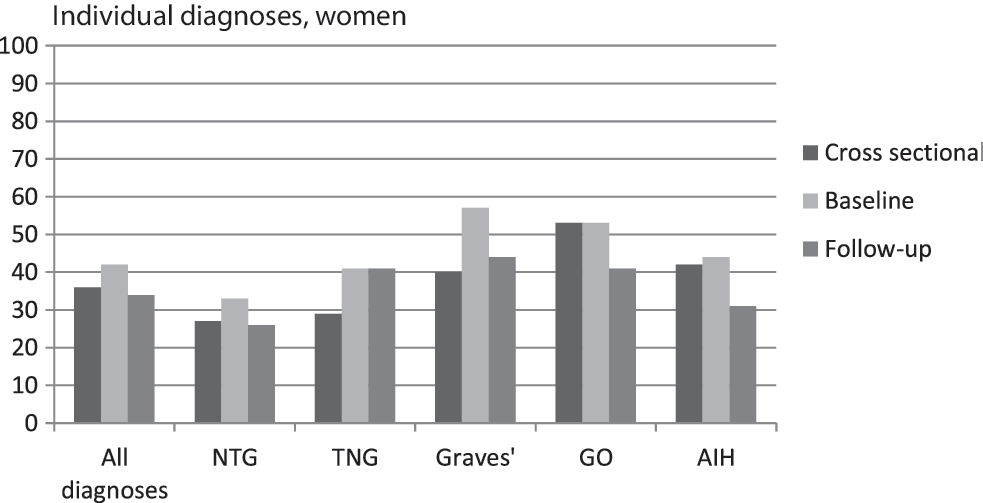
Percentage of female patients reporting a negative influence of thyroid disease on their sex life. AIH autoimmune hypothyroidism; GO Graves' orbitopathy; Graves', Graves' hyperthyroidism; NTG, non-toxic goiter; TNG, toxic nodular goiter.

Percentage of patients reporting a negative influence of thyroid disease on sex life, separately for each gender, irrespective of thyroid diagnosis. In the cross-sectional sample and at the two timepoints in the longitudinal sample. Test of gender differences and of change from baseline to follow-up as indicated (Fisher's exact test and McNemar's test). ns, not significant.
Data are presented as total numbers and percentage, and 95% confidence intervals of the percentages are provided for each group. Number of missing responses n (%) are also presented for each group.
N = nonmissing responses.
Proportion smaller among patients with nodular goiter, compared to autoimmune diagnoses (nontoxic goiter vs. Graves' p = 0.019, GO p < 0.001, AIH p = 0.003; toxic nodular goiter vs. GO p = 0.001, AIH p = 0.029) in cross-sectional sample.
Proportion larger in Graves' hyperthyroidism, compared to non-toxic goiter (p = 0.029), at baseline.
Proportion smaller at 6 months follow-up, compared to baseline (all patients: p = 0.006, autoimmune hypothyroidism p = 0.049).
No gender difference.
GO, Graves' orbitopathy; AIH, autoimmune hypothyroidism.
Prediction of ThyPRO Impaired Sex Life scale scores
In the cross-sectional sample, the Impaired Sex Life scale scores were only related to clinical variables in two instances: in patients with Graves' disease, those with the longest (+5 years) education presented less impact on sex life than those with shorter educations (all with large differences), except for patients currently studying and patients with an apprenticeship education (Table 3). Among patients with toxic nodular goiter, those with comorbidity scored 21 points worse than those without (estimated mean score 31 vs. 10, p = 0.0017).
The group with significantly different scores is in bold, and the groups from which it was different is indicated with superscript letters. Framework for interpretation of effects in accordance with Cohen (28): small difference (effect size 0.2–0.5), 4–10 (marked*); moderate difference (effect size 0.5–0.8), 10–16 (marked **); and large difference (effect size >0.8) >16 (marked ***).
In the longitudinal sample, total T3 was positively associated with Impaired Sex Life scores in patients with Graves' disease at baseline, for each nmol/L increment in total T3 (ref. interval 1.4–2.8 nmol/l) a worsening of the Impaired Sex life score of 6 points (p = 0.0007) was observed. No other associations were found at baseline.
Impaired Sex life scores at follow-up were associated with baseline variables in three instances: (1) in patients with toxic nodular goiter, students and those with long education had impaired sex life scores (large effect sizes). (2) in patients with Graves' disease, plasma T3 was positively associated with Impaired Sex life scores −4 points worsening (p = 0.0032) per 1 nmol/L increment in plasma T3. (3) in patients with autoimmune hypothyroidism, age was negatively associated with Impaired Sex Life scores (i.e., 4 points [corresponding to a small effect size] less negative impact per 10-year increase in age).
No variables were associated with change in Impaired Sex life scores from baseline to follow-up.
When examining the relationships between clinical variables at follow-up on Impaired Sex Life score at follow-up, a positive association between plasma T3 and Impaired Sex Life score was again found in patients with Graves' disease: for every nmol/L increase in T3, Impaired Sex Life score worsened by 18 points (p = 0.0048, large effect size). No other associations were identified.
Effect of impaired sex life on overall QOL measures
Estimated mean levels of the two SF-36 overall QOL-measures (MCS andPCS) and the ThyPRO Overall QOL-impact scale are presented in Table 4. Among all diagnostic groups in the cross-sectional sample, worse SF-36 MCS as well as PCS scores were found in patients who experienced negative thyroid influence on sex life (small to large effect sizes as indicated in Table 4). The same was found for the ThyPRO Overall QOL impact scale (all with large effect sizes).
Data are estimated mean score levels, controlled for age and education. Significantly (p < 0.05) worse scores among patients reporting impaired sex life are in
Scored to norm-mean 50 and standard deviation 10, lower scores with worse QOL.
Scored 0–100, higher scores with more impairment of QOL.
MCS, Short Form-36 (SF-36) Health Survey Mental Component Summary; PCS, Physical Component Summary; QOL, quality of life.
In the longitudinal sample, a baseline association between impairment of sex life and worse SF-36 MCS scores among those with impairment of sex life was found in patients with both nontoxic or toxic nodular goiter (moderate effect sizes), but not in the other groups. Baseline scores on ThyPRO Overall QOL impact (large effect) and the SF-36 Physical Component Summary (small effect) showed similar results, albeit for the latter only in patients with nontoxic goiter.
At follow-up, worse SF-36 Mental Component Summary scores among those who perceived their sex life as impaired were found in patients with both nontoxic (small effect size) or toxic nodular goiter (large effect), as well as in patients with autoimmune hypothyroidism (moderate effect). Similarly, SF-36 Physical Component Summary remained low in patients with nontoxic goiter who reported impaired sex life, and this also applied to patients with Graves' disease (both with moderate effect sizes). In addition, worse ThyPRO Overall QOL-scores were observed among patients with impaired sex life, irrespective of whether they were diagnosed with Graves' disease, or nontoxic or toxic nodular goiter (all with large effect sizes).
Discussion
The purpose of this study was to evaluate sex life in patients with thyroid diseases and to examine both the clinical variables associated with what patients themselves perceived to be thyroid-attributable impaired sex life and any relationships with overall quality of life. To the best of our knowledge, this is the largest study investigating this issue in patients with thyroid disorders.
Prevalence of sex life impairment
Based on information from a large cross-sectional sample of patients with thyroid diseases and a longitudinal sample of patients receiving treatment for thyroid disease who completed the ThyPRO quality of life questionnaire and SF-36, it was noted that a negative influence of thyroid disease on sex life was common: a third of the patients in the cross-sectional sample reported some impact on sex life. In the longitudinal sample, as many as two fifths of patients experienced a negative impact on sex life at baseline. This proportion decreased to one third after treatment, suggesting an effect for thyroid dysfunction on sexual well-being. The observed decrement was statistically significant only in women, but the fact that the prevalence in women (42%) is within the range of the 95% confidence interval for the baseline prevalence in men (22–44%), indicates that this difference may be due to the low number of men in the sample rather than being a true gender difference. The prevalence of sexual problems among females and males has varied in previous studies and has probably reflected both the real differences between populations and between applied measurement instruments, thereby hampering comparisons between studies. Atis et al. analyzed a relatively small sample of hyperthyroid females and, similar to our study, found sexual dysfunction in 60%, in comparison to 32.5% among healthy women (10). In a study of 1494 Danish citizens (aged 18–88 years) it was found that 11% of women and 18% of men were dissatisfied with their sex life, but at the same time 30% of women and 27% of men complained of sexual dysfunction (30). Although the specific reference to impairment due to thyroid disease in the present study hampers direct comparison with these data, the similarity between these two frequencies may be due to patients with thyroid disease attributing unrelated symptoms of sexual dysfunction to their thyroid disease.
Clinical predictors of sex life impairment
Age and menopause are relevant contributors to sexual dysfunction in women (31). In a representative Danish population, libido decreased with age (32). However, comorbidities and lifestyle are fairly strong predictors of deterioration of sex life in the elderly, rather than age per se (33). Inconsistent with the abovementioned observations, we observed that younger women with autoimmune thyroid disease reported a higher impact on sex life compared with older women. This finding might be explained by the fact that the typical symptoms of dysthyroidism are more severe in younger patients (34 –36). This indicates that the thyroid-attributed impaired sex life reported by patients is indeed caused to some extent by the thyroid disease.
Increased comorbidities observed in patients with thyroid diseases (37 –40) might lead to a deterioration in sex life. Although more than half of the patients in the cross-sectional sample and one third in the longitudinal sample reported comorbidities, we found that comorbidities negatively influenced sex life only in patients with toxic nodular goiters.
In the cross-sectional sample, women with autoimmune thyroid disease (Graves' hyperthyroidism, Graves' orbitopathy and Hashimoto's thyroiditis) reported worse impairment of sex life than women with non-autoimmune thyroid disease (nodular goiter and toxic nodular goiter), which hints at an influence of autoimmunity per se. Only three previous studies have evaluated the impact of thyroid autoimmunity independently of thyroid function on sexual functioning in women with Hashimoto's thyroiditis (8,9,12). They found that impaired sex life and decreased libido were associated with chronic autoimmune thyroiditis. Krysiak et al. also reported decreased libido, lubrication, and sexual satisfaction in euthyroid women with Hashimoto's thyroiditis (12). We found that among women with Graves' hyperthyroidism, as many as 57% reported what they perceived to be thyroid-attributable impaired sex life. At 6 months follow-up, this proportion had declined to 44%. We also observed a higher prevalence of what patients perceived to be thyroid-attributable impaired sex life in women with Graves' hyperthyroidism, even after 6 months of treatment, as compared to females with toxic nodular goiter. Higher levels of thyroid hormones in patients with Graves' disease might explain the observed difference at baseline, while the etiology of the difference observed at follow-up is less obvious. Our observations are consistent with previous studies reporting worse QOL in patients with Graves' disease than in patients with toxic nodular goiters, and the persistence of impaired QOL during short- and long-term follow-up 41–43). A possible explanation of our findings might be related to TR-Ab autoantibodies, which are elevated in Graves' patients. Extra-thyroidal TSH receptor expression, together with the transcript needed for thyroid hormone production, has previously been identified in the endometrium, suggesting that it might synthesize thyroxine. Thus, TR-Ab might alter local homeostasis and paracrine interactions, contributing to sexual dysfunction.
Since no variables were associated with changes in Impaired Sex Life scores from baseline to follow-up, no suggestions regarding any etiology or mechanisms of the improvement are provided from this study. Such indications await specific interventional studies.
A relatively consistent finding regarding the relationship between sex life and total T3 was observed among hyperthyroid patients (both toxic nodular goiter and Graves' hyperthyroidism): the higher the plasma T3, the more impact on sex life, both at baseline and at follow-up. Our observations are similar to those of other studies reporting decreased sexual functioning in hyperthyroid men and women (8 –10,44). Oppo et al. found an inverse correlation between free T4 and desire in hyperthyroid females (8). Atis et al. also found an association between sexual dysfunction and free T3 and free T4 levels in hyperthyroid females (10). A decreased concentration of androgens with a concomitant increase in sex hormone binding globulin has been suggested as a possible mechanism (45). In hyperthyroid females, sexual dysfunction may also result from psychiatric or psychological changes caused by the disease (39). Similarly, in men with hyperthyroidism, high frequencies of premature ejaculation have been observed, which improve after normalization of thyroid function (44,46). Low sexual desire, erectile dysfunction, and ejaculation disorders are correlated with serum levels of TSH and thyroid hormones (44). Our finding of low education predicting sexual dysfunction in patients with toxic nodular goiter is in line with previous research (8).
Sex life and overall quality of life
In the cross-sectional sample, we found that patients reporting impaired sex life had worse overall QOL. Undoubtedly, sex life is a relevant aspect of overall quality of life. However, our study does not reveal whether impaired sex life worsens the overall QOL in thyroid patients, or if worse overall QOL impairs sex life in thyroid patients. Similar relationships between limited sexual satisfaction and decreased well-being have been noted in different groups of patients (47,48).
The main limitation of our study is the lack of a control group, which ideally would be a group of patients suffering from a non-thyroidal disease, and with a comparable overall QOL, as assessed by SF-36. Also, we did not use an instrument solely dedicated to sexual dysfunction assessment. However, by applying a thyroid-specific measure of negative impact on sex life, the prevalence of impaired sex life, directly attributed by the patients to their thyroid disease, can be obtained. It is nonetheless important to consider that, within the ThyPRO, the attribution of sex life impairment to thyroid disease is made by the patients themselves. Asking the question in this fashion may bias the results toward patients assuming their sex dysfunction is related to their thyroid disease when it is not. In general, self-awareness of a disease may predispose patients to reporting symptoms that they would otherwise not pay much attention to, or that they might otherwise attribute to aging, stress, etc. Nonetheless, this is indeed a descriptive study, reporting what the patients experience, providing an important insight into a potential clinically unsatisfied need, for example for assessment, counseling or even therapy. Other limitations are the relatively small number of men in the study and the inclusion of only Danish speaking patients, leading to an ethnically rather homogeneous sample. Further, for ethical and data protection reasons, it was not possible to conduct nonresponder analyses. Finally, due to the large number of tests performed, some significant findings may be due to chance. However, the three-level significance requirement of the analysis strategy was preventive of such. Also, the fact that all statistically significant effects were above the 0.2 effect size limit, and indeed two-thirds were classified as large effects (and only two of the 36 significant effects were small), dispels the concerns about false significant findings.
Future studies could apply a sex life impairment measure without attribution to thyroid disease and estimate the impairment attributable to thyroid disease by careful selection of control groups. Future research should also focus on identifying specific aspects of sex life impairment, and the effect of different treatment modalities on sex life improvement. Relevant clinical variables, and possibly further sociodemographic variables, for example cohabitation, employment status, children living at home potentially affecting sexual QOL should be characterized to predict which patients are at risk of sex life impairment. For further improvement of patient care, short versions of questionnaires should be developed and applied in everyday clinical practice to inform physicians about sex life impairment and to assess the effect of the treatment of the thyroid disorder. Furthermore, intervention studies are needed to investigate whether patients with impaired sex life due to thyroid disease will benefit from, for example, psychotherapy.
In conclusion, we have found a high prevalence of patient-attributed, thyroid-related sex life impairment in patients with benign thyroid diseases, especially among young women with autoimmune thyroid diseases. Self-perceived impaired sex life persisted in treated women with Graves' disease suggesting that the normalization of thyroid function is not sufficient to abolish sexual dysfunction. These observations support a multidisciplinary approach to thyroid patients to facilitate communication and improve the quality of their sex life.
Footnotes
Author Disclosure Statement
J.B. is an employee of Optum, which distributes the SF-36. N.S.G., M.R., U.F.R., A.K.R., L.H., M.G., S.J.B., and T.W. have nothing to disclose.