
Abstract
Background:
Previous studies have suggested that oncocytic variant papillary thyroid carcinoma (PTC) may be more aggressive, with higher rates of recurrent disease. The aim of this study was to evaluate characteristics and outcomes of patients with oncocytic variant PTC compared to classical PTC.
Methods:
Patients with oncocytic variant PTC were retrospectively identified from 519 patients who underwent thyroidectomy for PTC between January 2009 and August 2015. Data collected included patient demographics, laboratory and pathology findings, imaging studies, treatment, and follow-up. Patients were matched 1:1 by age, sex, and TNM stage with patients who underwent total thyroidectomy for classical PTC during the same time period.
Results:
The cohort included 21 patients, of whom 18 (86%) were female, with a median age of 53 years (range 23–68 years). All patients underwent total thyroidectomy, and 17 (81%) had a central compartment neck dissection (8 [38%] prophylactic). The median tumor size was 2.0 cm (range 0.9–6.5 cm), and four (19%) patients had extrathyroidal extension. There was no significant difference in histopathologic characteristics, including extrathyroidal extension and lymphovascular invasion, between the two groups except for an increased incidence of thyroiditis in oncocytic variant PTC (90.5% vs. 57%; p = 0.01). In oncocytic variant PTC patients who underwent central compartment neck dissection, malignant lymph nodes were found in 12 (57%) patients compared to 13 (62%) classical (p = 0.75). Lateral neck dissection was performed in 5 (24%) oncocytic variant and classical PTC patients, with metastatic lymphadenopathy found in four (a median of four malignant lymph nodes; range 1–6) and five (a median of 2.5 malignant lymph nodes; range 1–9), respectively. Radioactive iodine was administered to 18 (86%) oncocytic variant PTC and 18 (86%) classical PTC patients. At a median follow-up of 51 months (interquartile range 38–61), one oncocytic variant PTC patient had recurrent disease and underwent reoperation at 24 months. In classical PTC patients with a median follow-up time of 77 months (range 56–87 months), two (9.5%) patients had detectable thyroglobulin levels indicating early recurrence, but neither has undergone reoperation.
Conclusions:
Oncocytic variant PTC was present in 5% of PTC patients. Most (95%) patients remain disease-free at four years, similar to classical PTC outcomes, suggesting that oncocytic variant may not represent a more aggressive variant.
Introduction
P
Oncocytic thyroid cells, also referred to as oxyphilic or Hürthle cells, are characterized by abundant eosinophilic cytoplasm and are generally larger than normal follicular epithelial cells (11). Oncocytic changes may be seen in benign thyroid conditions such as autoimmune thyroiditis (primarily Hashimoto's thyroiditis), follicular nodular disease, and in both benign and malignant thyroid neoplasms (9,12,13). The oncocytic variant of PTC is comprised of oncocytic cells with classic nuclear features of PTC such as enlarged, elongated, irregular nuclei, which are also clear, crowded, and overlapping with prominent grooves and pseudoinclusions (9,12 –17). The pure form of oncocytic variant is very rare and must be differentiated from the tall-cell variant of PTC, which also has abundant eosinophilic cytoplasm but is characterized by cells that are two to three times as tall as they are wide (17).
The incidence of oncocytic variant PTC has been reported to be 1–11%, although there are few recent population studies (16,18). Some reports have suggested that oncocytic variant PTC has more aggressive features such as extrathyroidal extension and higher rates of disease recurrence and cause-specific mortality (up to 28% and 17%, respectively, at 10 years) (6 –8,19). However, others have reported that oncocytic variant PTC has similar outcomes to classical PTC when the age of the patients and tumor stage are comparable (7,9,20,21). Due to the low prevalence of oncocytic variant PTC, variations in diagnostic criteria and classification, and limited follow-up, it is not certain whether patients with oncocytic variant PTC should undergo more extensive surgery or be monitored more closely for disease recurrence (6 –8,22). This study evaluated the authors' institutional experience with oncocytic variant PTC and compared these patients to those with classical PTC. The hypothesis was that there would be no significant difference in recurrence rates between groups when stage of disease was similar, and therefore surgical treatment and postoperative surveillance should remain identical.
Methods
This is a retrospective medical record review of a prospectively collected single institution thyroid database of patients who underwent total thyroidectomy and had a final diagnosis of PTC between January 2009 and August 2015. The study was approved by the Institutional Review Board. All patients >18 years of age reported to have had oncocytic variant PTC on final pathology were reviewed; patients who had previous thyroid and/or parathyroid surgery or who had distant metastases at initial presentation were excluded. All specimens were reviewed again by a single pathologist from the group (B.H.) to confirm proper and consistent classification. Based on the World Health Organization (WHO) definition and prior reports, oncocytic variant PTC was defined as a tumor that showed papillae and/or invasive growth; nuclear features of PTC, including enlargement, elongation, clearing, grooves, and scattered pseudoinclusions; and oncocytic findings of abundant, granular eosinophilic cytoplasm in ≥75% of cells (7,9,12,13,17). Patients with oncocytic variant PTC were matched in a 1:1 manner by age, sex, and TNM stage with patients who underwent total thyroidectomy for classical variant PTC treated during the same time period as a comparison group. All classical variant PTC specimens were also reviewed again to confirm proper and consistent classification.
All patients underwent preoperative high-resolution cervical ultrasound (US) of the thyroid and cervical lymph node compartments (levels II–VI) with fine-needle aspiration (FNA) biopsy of thyroid nodules and abnormal lymph nodes per contemporary guidelines of the American Thyroid Association (ATA). All USs were performed by experienced radiologists or endocrinologists (3). The cytology report of thyroid nodule FNA biopsies was classified based on The Bethesda System for Reporting Thyroid Cytopathology (23). Therapeutic central and/or lateral compartment neck dissections were performed for patients with a clinically suspicious or biopsy-proven lymph node metastases; prophylactic central compartment neck dissection was performed for patients with no evidence of metastatic lymphadenopathy on clinical examination or preoperative US at the preference of the surgeon. The final histopathology noted tumor size(s), the presence of extrathyroidal extension, lymphovascular invasion, and central and lateral compartment lymph node metastases, if lymphadenectomy was performed. TNM staging was based on the AJCC seventh edition (24).
Data reviewed included patient demographics, preoperative imaging and diagnostic study results (including preoperative FNA of thyroid nodules and lymph nodes, if performed), extent of surgery including central and lateral compartment neck dissections, pathological review, postoperative complications, postoperative treatment, and follow-up. Complications included permanent hypoparathyroidism and recurrent laryngeal nerve (RLN) injury. Permanent hypoparathyroidism was defined as persistent hypocalcemia six months or more after surgery that required calcium and/or calcitriol supplementation. RLN injury was evaluated by laryngoscopy based on patient reported voice changes postoperatively.
Recommendations for radioactive iodine (RAI) ablation treatment were based on ATA recommendations for risk stratification (25). Patients were followed every 3–12 months with a physical examination, serum thyroglobulin (Tg) and Tg antibody measurement while on thyroid hormone therapy or after thyrotropin (TSH) stimulation (by either thyroid hormone withdrawal or recombinant human TSH administration), and imaging with at least one of the following: neck US, computed tomography (CT), or RAI whole-body scan. Disease status after primary treatment and at follow-up assessments was defined as no evidence of disease if imaging studies showed no measurable disease and if a non-stimulated Tg level was <2 ng/mL or a stimulated Tg level was <10 ng/mL. Patients with a postoperative elevated non-stimulated Tg level >2 ng/mL or a stimulated Tg level >10 ng/mL were considered to have persistent disease. Patients who were without evidence of disease initially and then developed an elevated non-stimulated Tg level >2 ng/mL or a stimulated Tg level >10 ng/mL and/or abnormal neck imaging were classified as having recurrent disease. The primary outcome measure was recurrence. The minimum requirement for follow-up was a Tg level at least six months after surgery (stimulated or unstimulated) and imaging at approximately one year after surgery.
Results
Of the 519 consecutive patients with PTC who met the study criteria, 25 (4.8%) patients had oncocytic variant PTC reported. The final cohort consisted of 21 patients; three patients were excluded from analysis, as there were no follow-up data beyond the initial postoperative visit. On re-review, one patient only had focal areas of oncocytic changes and was thus excluded. Compared to the age-, sex-, and stage-matched cohort of patients with classical variant PTC, there was no difference in body mass index (BMI), tumor size, treatment, or complications between the two groups (Table 1).
Values are n (%) unless otherwise indicated.
AJCC, American Joint Committee on Cancer; BMI, body mass index; CCND, central compartment neck dissection; IQR, interquartile range; MRND, modified radical neck dissection; PTC, papillary thyroid cancer; RLN, recurrent laryngeal nerve; RAI, radioactive iodine.
Of the 21 patients with oncocytic variant PTC, two patients had Bethesda III nodules on preoperative cytology. One patient had planned total thyroidectomy for a multinodular goiter, and one patient had an intraoperative frozen section that identified PTC and therefore underwent total thyroidectomy. One additional patient had Bethesda I findings preoperatively and underwent planned total thyroidectomy for a multinodular goiter. The remaining 18 patients all had PTC identified on preoperative FNA biopsy, with three having suspected oncocytic variant PTC.
Compared to patients with classical PTC, there was no significant difference in histopathologic characteristics of oncocytic variant PTC, including the presence of extrathyroidal extension or lymphovascular invasion, although the presence of thyroiditis was higher in oncocytic specimens (90.5% vs. 57%; p = 0.01; Table 2). The oncocytic variant PTC specimens demonstrated the nuclear features of PTC but were differentiated from the classical PTC group based on their abundant, granular, and eosinophilic cytoplasm (Fig. 1). One case of oncocytic variant PTC showed 75% oncocytic features, while the remaining 20 cases were entirely oncocytic. Within the oncocytic variant PTC group, four (19%) specimens had some focal areas with tall-cell features, but not the ≥30% that is required to be classified as tall-cell variant of PTC (17). The classical PTC specimens all contained papillary architecture and nuclear features of PTC (Fig. 2). There was no significant difference in the prevalence or extent of central neck disease, including the number of patients who had more extensive central neck disease (≥4 lymph nodes involved; 8 [38%] oncocytic PTC patients vs. 5 [24%] classical PTC patients; p = 0.16).
Classic papillary thyroid carcinoma (PTC). Representative photo from a classic PTC. All the classic cases have papillary architecture and show the nuclear features of PTC, including enlargement, elongation, clearing, grooves, and scattered pseudoinclusions (hematoxylin and eosin [H&E] stain; 20 × objective lens). Color images available online at

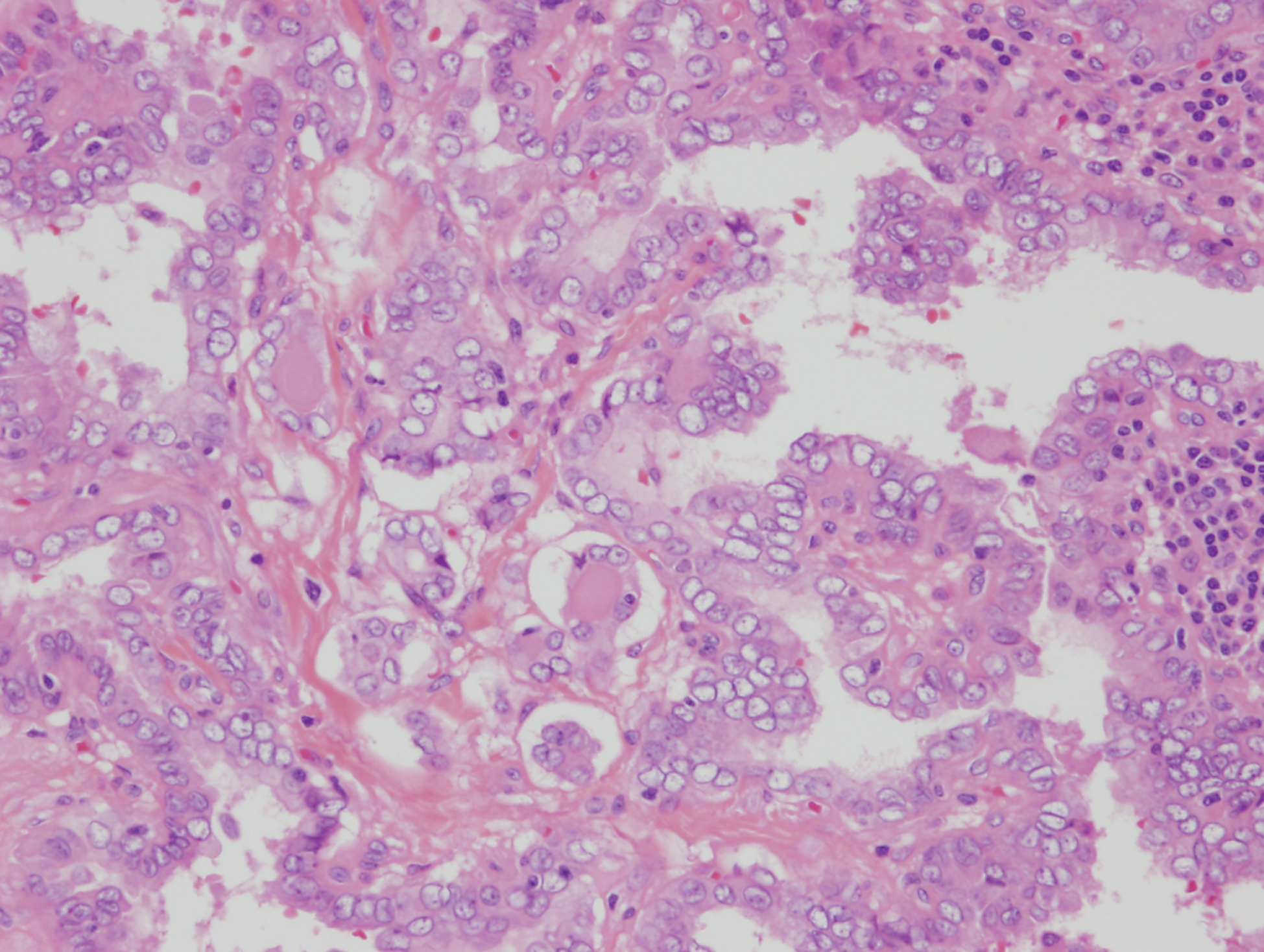
Oncocytic variant of PTC. Representative photo from an oncocytic variant of PTC. All the oncocytic variant cases show the nuclear features of PTC, including enlargement, elongation, clearing, grooves, and scattered pseudoinclusions. The oncocytic variants are differentiated from the classic cases by their abundant, granular, and eosinophilic cytoplasm (H&E stain; 20 × objective lens). Color images available online at
Values are n (%) unless otherwise indicated.
Of 17 patients who had CCND.
Of 20 patients who had CCND.
Of 5 patients who had MRND.
Of 5 patients who had MRND.
Per lateral neck side.
Postoperative treatment and follow-up
RAI was given to 18 (86%) patients with oncocytic PTC (range 32.4–152 mCi) and 18 (86%) classical PTC patients (range 53–108.4 mCi; Table 1). There was no difference in stimulated Tg levels between groups (p = 0.06). Stimulated Tg levels were available for 13 patients with oncocytic variant (median 0.5 ng/mL; range 0.5–10.4 ng/mL) and for 17 classical PTC patients (median 3.7 ng/mL; range 0.5–42.1 ng/mL).
In the oncocytic group, one (5%) patient had structural recurrence, and no patients had persistent disease. The one patient with recurrence in the oncocytic group had initial total thyroidectomy with bilateral therapeutic central neck dissection with findings of left RLN involvement and adherence to the esophageal wall. Initial staging was IVA (T4aN0M0), with focal tall-cell features seen on pathology. The patient received 79 mCi of RAI, with a stimulated Tg level of 2 ng/mL. In the first postoperative year, the non-stimulated Tg level was undetectable. However, both non-stimulated and stimulated Tg levels were markedly elevated at 22 months from the date of operation (22.1 and 80.7 ng/mL, respectively). Imaging (US and CT) showed recurrence in the central neck and left lateral neck, as well as multiple new suspicious bilateral pulmonary nodules. Left central and lateral compartment neck dissection was performed. The patient died one month after reoperation due to cardiorespiratory complications.
For patients with classical PTC, no patient has required reoperation for structural recurrence. Two (9.5%) patients have detectable Tg levels, which indicate residual/early recurrent disease. One patient with stage I disease (T2N1b) treated with RAI (administered activity 102.6 mCi) had non-stimulated Tg levels at 6, 8, 11,19, 24, and 30 months, which were 1.6, 2, 2.1,4.3, 2.8, and 3.6 ng/mL, respectively. Imaging at one and two years has identified no structural abnormalities. The second patient with stage IVA disease (T3N1b) received RAI (administered activity 106.5 mCi). At one year, Tg levels (stimulated and unstimulated) were 8.2 ng/mL and <0.2 ng/mL, respectively. However, at 19 months, the unstimulated Tg level increased to 2.2 ng/mL, and at 53 months, the stimulated Tg level was 21.4 ng/mL. There has been a stable 5 mm hypoeochoic nodule in the thyroid bed, initially detected at 26 months postoperatively, with a total follow-up of 78 months.
Discussion
Oncocytic variant PTC has been recognized by the WHO for nearly three decades. However, management continues to be a challenge due to inconsistencies in thresholds for diagnosis and the poorly defined effects of the oncocytic variant on prognosis. This study demonstrates that when matched with classical PTC of similar stage and age, oncocytic variant PTC does not appear to have worse histopathologic characteristics or confer a significantly worse prognosis.
The identification of oncocytic change in thyroid tumors may lead to confusion and lack of clarity regarding diagnosis and management. Solitary thyroid nodules that are primarily composed of oncocytic cells on FNA may show an average 30% malignancy rate (11). In addition, larger oncocytic lesions (>4 cm) may have an 80% chance of showing malignancy (26). The criteria used for the diagnosis of oncocytic variant PTC include the same nuclear morphological features seen in classical PTC such as irregularly shaped, crowded nuclei, with prominent grooves and pseudoinclusions. The majority of cells should exhibit oncocytic cytoplasm. Although the WHO does not clearly define a threshold for oncocytic findings, most reports use a threshold of ≥75% as in this study (7,9,12,13,16,17).
Previous reports on oncocytic variant PTC have shown conflicting results. Herrera et al. reported on 22 patients with oncocytic variant PTC treated between 1940–1951 and 1970–1989, and they found that the rate of recurrence was significantly higher (>25% at 10 years compared to 11% at 10 years in classical PTC (6). However, treatment methods since those time periods have changed significantly, which makes comparison to more current reports challenging to interpret. Hong et al. recently reviewed the outcomes of 65 patients with oncocytic changes in PTC. However, they included all patients with any component of oncocytic change >10% (19). They found patients with oncocytic changes had a higher BMI and higher recurrence rate. However, this was not stratified according to percentage of oncocytic changes observed. Variations for the threshold of diagnosis may contribute to the varied reports on aggressiveness of disease and prognosis. Other prior reviews have indicated oncocytic variant PTC has a similar prognosis to classical PTC (7,20,27,28). Tumor characteristics in studies have also differed, with some reporting a higher incidence of extrathyroidal extension, which was not identified in the present cohort (7). The rate of multifocal disease has also been variable, with reported rates of 14.7% by Beckner et al. and 24.7% by Gross et al.; 50% of the present cohort had multifocal disease (7,27). In the current review of 21 patients, oncocytic variant PTC did not have more aggressive tumor features, and the risk of recurrence was similar to age-, sex, and stage-matched patients with classical PTC. As referenced in the most recent WHO classification, it is important to differentiate the oncocytic variant from tall-cell variant of PTC, which has an established worse prognosis (17). This may be a potential confounding factor that has led to associations of oncocytic variant PTC with increased aggressiveness and worse prognosis.
The clinical significance of increased evidence of thyroiditis in the current cohort of oncocytic variant PTC is not clear. This finding has also been demonstrated in other studies (8,16). It has been proposed that the oncocytic changes seen may be a secondary response in the tumor cells to the thyroiditis rather than an inherent characteristic of the cancer (7,16). There have been several reports linking Hashimoto's thyroiditis and PTC (29). In several series, these cases are found to occur more often in young women, with less aggressive disease, less frequent nodal metastases, low recurrence rate, and a high survival rate (30 –33). It is not certain whether Hashimoto's thyroiditis is a risk factor for developing PTC, an incidental finding, or part of a response to the tumor (29).
The recurrence rate for both groups is low: 4.5% in oncocytic variant PTC and 9% in classical PTC (p = 0.55). There was only one patient who underwent reoperation for structural recurrence in the oncocytic variant group. The tumor in this patient had tall-cell features on initial and repeat pathology, which may have contributed to increased risk of recurrence. Three other patients who had minimal areas of tall-cell features had no evidence of recurrence at 27, 51, and 66 months of follow-up.
Limitations in this study include the overall small number of patients with oncocytic variant PTC, which is attributed to the relatively low incidence of oncocytic variant PTC (6,7,16,27). Follow-up is relatively short, especially for the patients with oncocytic variant PTC (median 51 months; interquartile range [IQR] 38–61 months) compared to the classical PTC group (median 77 months, IQR 56–87; Table 1). Previous studies have shown that the mean time to recurrence may be up to 69 months, although others have shown that most recurrences occur in the first 30 months (7). Since the identification of oncocytic variant PTC cases for this study was based on initial pathology reports, it is possible that other oncocytic variant cases were not included. However, since the majority of thyroid specimens during this study period were reviewed by a single pathologist, the likelihood of under-reporting is likely to be low. Finally, the potential variability in identifying oncocytic variant PTC among pathologists may affect the generalizability of the study results.
In conclusion, this study adds to the currently available data suggesting that patients with oncocytic variant PTC may not have more aggressive disease and increased risk of recurrence when compared to patients with classical PTC of comparable age and stage of tumor. However, due to the small number of patients that present with oncocytic variant PTC in numerous studies that show conflicting outcomes, it is challenging to make definitive recommendations regarding management. Continued refinement and education on the definition of oncocytic variant PTC would aid in the study of the disease. Management and follow-up of patients should be based on the extent of disease identified and the use of the ATA risk-stratification system to guide surveillance and management (3).
Footnotes
Acknowledgments
This manuscript was presented as a poster at the 85th Annual Meeting of the American Thyroid Association, October 18–23, 2015.
Author Disclosure Statement
No competing financial interests exist.