
Abstract

Common management options for Graves' disease (GD) include medical treatment, radioactive iodine (RAI) ablation, or surgery. Thionamides (carbimazole, methimazole, and propylthiouracil) are the first-line medical treatment of GD. Due to potential hepatotoxicity, their use in the setting of underlying hepatic disease can be challenging. For such cases, and if thyroidectomy or RAI cannot be rapidly implemented, alternative medical strategies are not well-established.
We report the case of a 28-year-old Caucasian female diagnosed with type I autoimmune hepatitis (AIH) with severely altered liver function tests (alanine aminotransferase of 1437 IU/L, total bilirubin of 286 μmol/L) and GD. An undetectable thyrotropin (TSH) prompted a targeted history that revealed recent restlessness, rapid heartbeat, and increased stool frequency. Free thyroxine (fT4) and free triiodothyronine (fT3) were increased by more than twofold. Ultrasonography showed a normally sized but heterogeneous thyroid with increased vascularity. Autoantibodies against the thyrotropin receptor (TRAb) were strongly positive, and a diagnosis of GD was made. Due to the AIH, oral prednisone was started at 50 mg/day, with rapid improvement of hepatic function, allowing for progressive tapering after two weeks with concomitant introduction of azathioprine. Given the severe hepatitis, thionamides were withheld in accordance with American Thyroid Association guidelines recommending caution in case of more than fivefold transaminase elevation. Propranolol and low-dose cholestyramine were prescribed for three weeks. A rapid decrease of both fT4 and fT3 was observed as soon as 48 h after glucocorticoid (GC) initiation. After one month of immunosuppressive treatment, liver function tests, fT4, and fT3 were normal. The TRAb titer progressively decreased, becoming negative at six months of treatment (Fig. 1).
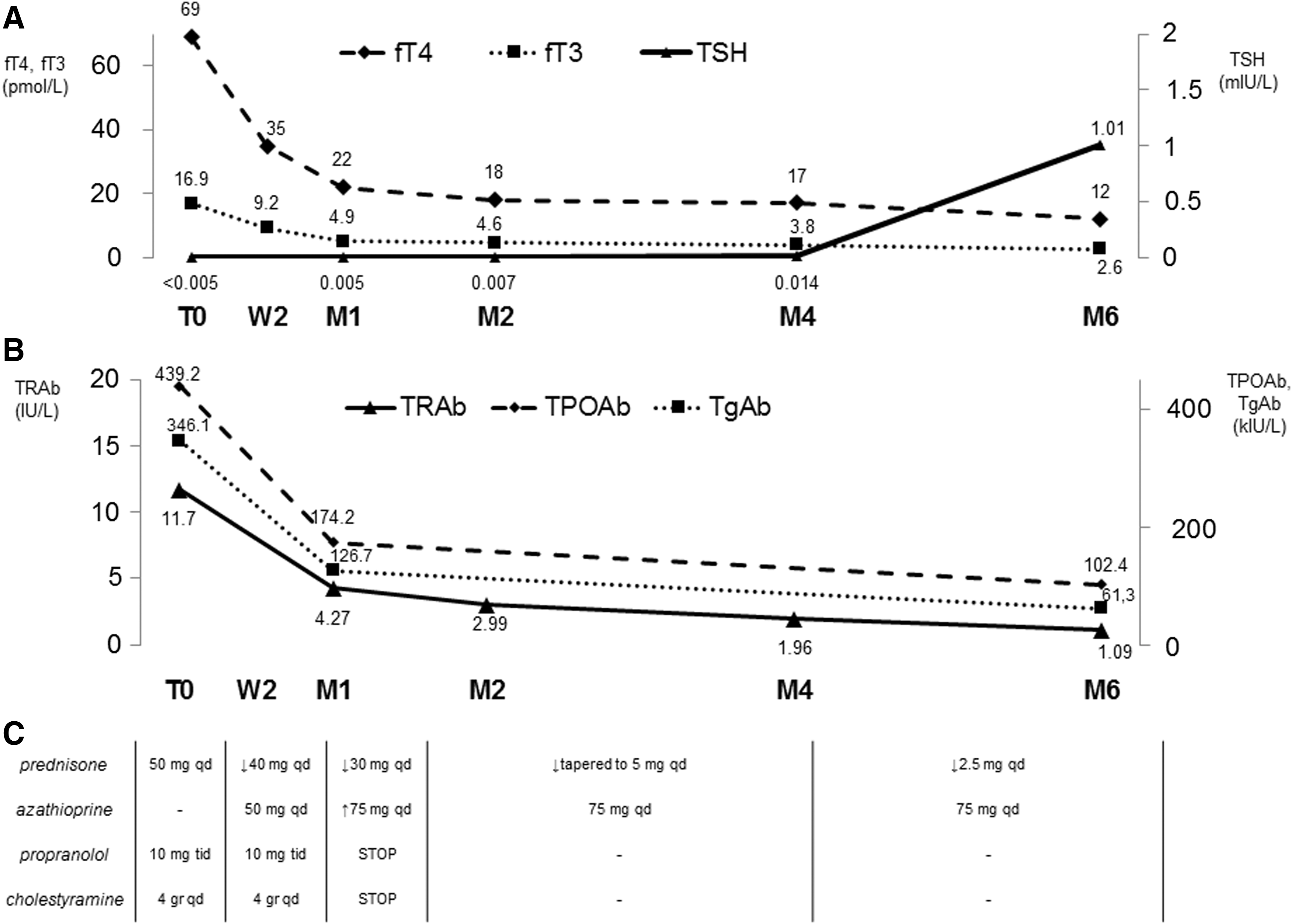
Graphical representation of thyroid function tests (
Somewhat paradoxically, GD is one of the few autoimmune diseases for which GCs are not part of the first-line therapeutic choices, mainly due to fear of complications from long-term administration. Nevertheless, GCs are routinely used in the management of thyroid storm and have proven effective in combination with carbimazole for resistant thyrotoxicosis.
Improvement of Graves' thyrotoxicosis with GCs was first reported in 1965 by Werner et al. who treated five GD patients with 100 mg/day of prednisone (1). In contrast to our case, some patients in that study had received prior treatment with propylthiouracil. In another study of GD patients (2), the rapid decrease of both T4 and T3 levels by short-term dexamethasone suggested that the benefit associated with GC therapy is mediated not only by inhibiting the conversion of T4 to T3 in peripheral tissues, but also by reducing thyroid hormone secretion. The present case suggests GC-mediated reduction of TRAb as a potential contributing mechanism. An alteration of the TRAb function and/or type is another possibility, which we were unable to explore because a TRAb bioassay was not performed. Data on the link between GCs and TRAb are scarce. Adding an intrathyroidal dexamethasone injection to methimazole significantly reduced TRAb levels in newly diagnosed GD patients in one study (3). Conversely, Kahaly et al. (4) detected a significant decrease of TRAb in patients with Graves' orbitopathy treated by intravenous but not oral GC for 12 weeks. Interestingly, baseline TRAb levels were higher in the latter study, possibly suggesting that oral GC might be less effective when the autoimmune load is higher. Other potential explanations for the notable response of TRAb in our case might be the slower tapering, longer treatment, and/or the addition of azathioprine.
We chose not to offer immediate definitive treatment to our patient. The risk of immediate total thyroidectomy was estimated to be too high in a context of acute hepatitis, while RAI was considered a suboptimal choice, given the risk for transient worsening of hyperthyroidism and the possible delayed beneficial effect.
In the absence of an iodine/pertechnetate uptake and scintigraphy, a painless thyroiditis with subsequent normalization of thyroid function cannot be formally excluded. Nevertheless, the ultrasonographic findings and the frankly positive TRAb, measured by a third-generation assay, render this diagnosis much less likely. Lastly, spontaneous remission may occur, such as in patients with alemtuzumab-induced GD. However, the very rapid pace of improvement of thyroid function as soon as 48 h after GC initiation argues against spontaneous remission.
In conclusion, this case highlights a potential role for GCs in selected GD patients with contraindications to thionamides who are not eligible for immediate definitive treatment. The onset of GC action in our patient appeared to be rapid, likely due to several distinct mechanisms, including suppression of T4 conversion to T3 and reduction of TRAb-mediated thyrocyte stimulation. Our observations warrant confirmation in the setting of a clinical trial. Treatment with non-GC immunosuppressants could also be explored.
Footnotes
Acknowledgments
This work was supported by a Leenaards Foundation Fellowship for Academic Promotion in Clinical Medicine to G.P.S.
Author Disclosure Statement
No competing financial interests exist.