
Abstract
Background:
Thyroid cancer is the most common endocrine tumor and generally has relatively good clinical outcomes. However, 15–20% of patients ultimately develop recurrence or disease-related death. The appropriate prognostic factors for thyroid cancer are still elusive. This study evaluated whether the number of circulating tumor cells/circulating epithelial cells (CECs) expressing either epithelial cell adhesion molecule (EpCAM), podoplanin (PDPN), or thyrotropin receptor (TSHR) is related to remission and disease-specific mortality (DSM) of patients with thyroid cancer.
Methods:
Blood samples were collected from patients (n = 128) after thyroidectomy or radioactive iodide therapy. CECs were enriched by lysis of red blood cells and depletion of leukocytes. Subtyping and quantification of the enriched cells were performed with immunofluorescence staining using antibodies against EpCAM, TSHR, and PDPN, respectively. Whether the number of a specific subtype of CECs is related to remission and DSM of patients was determined by univariate and multivariate analyses.
Results:
The EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs counts for patients in the non-remission group (n = 43) were significantly higher when compared to the remission group (n = 85; p < 0.001). Receiver operating characteristic analysis showed that the number of EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs was able to distinguish the status of remission from non-remission. The cutoff point for EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs was 40, 47, and 14 (cells/mL), with the accuracy of the assay equivalent to 80.4%, 76.6%, and 77.3%, respectively. On the other hand, the number of EpCAM+-CECs (p < 0.001), PDPN+-CECs (p = 0.013), and TSHR+-CECs (p < 0.001) for patients in the DSM group (n = 17) was significantly higher when compared to the patients who survived (n = 111). Receiver operating characteristic analysis showed that EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs counts were able to distinguish mortality from survival status. The cutoff point for EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs was 27, 25, and 9 (cells/mL), with the accuracy of the assay equivalent to 69.5%, 67.2%, and 68.5%, respectively.
Conclusions:
CEC testing is a useful tool for analysis of overall survival and remission status of patients with thyroid cancer. Implementation of CEC testing into routine clinical test may be worthy to consider for patient clinical care.
Introduction
T
Testing of serum level thyroglobulin (Tg) and medical imaging analysis are the two major modalities for monitoring disease recurrence in current clinical practice. Tg testing can be limited by the presence of anti-Tg antibodies (anti-TgAb) that interfere with the assay, while radioactive iodine is required for scintigraphic imaging analysis. Searching for new methods for monitoring disease status is warranted. The clinical use of liquid biopsies, including circulating tumor cells (CTCs)/circulating epithelial cells (CECs), circulating tumor DNA, and exosomes, in cancer diagnosis and prognosis has grown exponentially (9). In particular, the capacity of CTCs/CECs to provide biological information to assess the status of the patient underlines its potential as an independent biomarker to improve therapeutic outcomes (10 –12). Angiogenesis usually occurs in solid tumors when the tumor size is >2–3 mm3 (13,14). During angiogenesis, tumor cells of epithelial origin expressing epithelial cell adhesion molecule (EpCAM) may shed into the circulation to form CECs, which could serve as a surrogate marker for the angiogenic activity of a tumor and the degree of metastasis (15 –18). Recent studies from the authors' laboratory and others have revealed the potential applications of CEC testing in the early detection and disease monitoring of patients with thyroid cancer (11,19,20). CEC subtypes expressing different cellular markers have also been demonstrated. For example, CECs expressing podoplanin (PDPN) and thyrotropin receptor (TSHR) have been identified in the peripheral blood of patients with thyroid cancer (21). PDPN expression in cancer cells or cancer-associated fibroblasts is an independent unfavorable prognostic indicator in patients with various cancers (22). The TSHR is mainly expressed in thyroid cells, although cells from other tissues have been demonstrated to express TSHR (23). CECs with PDPN or TSHR expression have been shown to facilitate differentiating disease status of patients with papillary thyroid carcinoma (PTC).
CTCs/CECs characterization has also been shown to serve as a prognostic factor for various types of cancer, including lung, osteoblasts, and germ-cell tumors (22,24,25). However, little is known whether the CEC count in the bloodstream is related to the survival and remission status of patients with thyroid cancer. This issue was addressed in this long-term follow-up study. The potential applications of CEC testing in the clinical care of patients with thyroid cancer are discussed.
Methods
Study subjects
Patients were prospectively enrolled and cytopathologically diagnosed with thyroid cancer. After surgery, they underwent long-term follow-up and treatment at the Chang Gung Memorial Hospital in Linkou. This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (approval IDs 101-3497B, 102-4838C, 102-3433B, and 104-3901B). The enrollment criteria were: (i) aged >18 years, (ii) histopathologically diagnosed with thyroid cancer, (iii) able to comprehend fully and sign an informed consent form, and (iv) able to participate in a long-term follow-up study. Since 2015, 128 patients have been enrolled in the study, with a mean age of 46.1 ± 15.2 years (median 46 years), of whom 96 are women (Table 1).
Values are shown as the mean ± standard deviation or n (%).
Eleven cases were without tumor size.
RAI, radioactive iodine; Tg, thyroglobulin.
Patients underwent thyroidectomy at the authors' center after a diagnosis of thyroid cancer. All patients were staged in accordance with the Union for International Cancer Control tumor-node-metastasis (TNM) criteria (sixth edition) (26). All thyroid cancer tissues were pathologically classified according to the World Health Organization criteria (4). For cases with high or intermediate risk (27), 131I remnant ablation was performed. The dose of 131I ablation was 30–100 mCi (1.1–3.7 GBq) for most patients. In Taiwan, admission for isolation is required for patients receiving >30 mCi of 131I ablation. To balance the needs of patient care and the inconvenience of hospitalization for patients, post-thyroidectomy patients are subject to risk assessment for the aggressiveness of thyroid cancer to determine the administered activity of 131I. Patients who are considered high risk are typically treated with 100 mCi of 131I with admission for isolation, unless the patients refuse. On the other hand, patients who are considered as intermediate risk are recommended to receive 30 mCi for remnant ablation without admission for isolation. A post-therapy whole-body scan (WBS) was performed one week after 131I administration using a dual-head gamma camera (Siemens Medical Solutions USA, Inc., Malvern, PA), equipped with a high-energy collimator. The whole-body image was taken using continuous mode scanning at a speed of 5 cm/min. In addition, thyroid scintigraphy was performed using a pinhole collimator with a 4-mm aperture placed 7 cm above the neck for a total of 50 K counts or 30 min. Levothyroxine (LT4) treatment was initiated to decrease thyrotropin (TSH) levels without inducing clinical thyrotoxicosis. Cases in which the foci of 131I uptake extended beyond the thyroid bed were classified as either persistent disease or metastatic disease. Such patients received increased therapeutic activities of 100–200 mCi (3.7–7.4 GBq). WBS was performed two weeks after administering a higher therapeutic dose of 131I.
Neck ultrasonography was done 6–12 months after the initial thyroidectomy to exclude the possibility of local recurrence. Serum Tg was measured using a highly sensitive Tg access assay (Beckman Coulter, Brea, CA) when patients were on LT4 treatment and was used as an indicator for monitoring the disease status of patients. The blood samples used for CEC testing, serum Tg measurements, and other thyroid-related assays were collected simultaneously in one blood drawing. The serum levels of anti-TgAb were measured using a competitive radioimmunoassay (Biocode Hycel, Liege, Belgium) with an analytical sensitivity of 6 IU/mL. An anti-TgAb level <115 IU/mL was considered as not interfering with serum Tg testing. At the end of 2016, the enrolled patients were categorized into remission and non-remission groups. Non-remission is defined as biochemical and structural evidence for thyroid cancer, even after receiving multimodality treatments.
Cell culture and transfection
OECM-1 and HepG2 cells were cultured in Rosewell Park Memorial Institute 1640 medium supplemented with 10% fetal bovine serum (FBS). 293T cells were cultured in Dulbecco's modified eagle medium (DMEM) supplemented with 10% FBS and were transfected with plasmid DNA using the Lipofectamine 2000 (LF2000) reagent, as described previously (28,29). Briefly, 293T cells were plated at a density of 2 × 106 cells/six-well culture dish. Twenty-four hours after cell plating, the cells were transfected with the pCMV-SPORT6 expression plasmids (6 μg) in the presence of 10 μL LF2000. The culture medium was replaced with fresh DMEM five hours post transfection. Forty-eight hours post infection, the cells were re-suspended by trypsinization for immunofluorescence staining.
Enrichment and isolation of CECs
A negative selection-based PowerMag system was used for CEC enrichment and isolation, as previously described (11,19,20). Fresh blood samples obtained from patients four to six weeks after thyroidectomy or radioactive iodide therapy (131I) were processed through lysis of red blood cells (RBC) and depletion of CD45+ leukocytes using a magnetic chamber. This method has been used to detect EpCAM-positive and EpCAM-negative CECs/CTCs from patients with various cancer types (11,19).
Immunofluorescence staining and CEC characterization
During immunofluorescence staining, the leukocyte-depleted cell filtrates were separated into two aliquots. One of the aliquots was incubated with an anti-TSHR antibody (Abcam, Cambridge, United Kingdom) and DNA staining Hoechst 33342 dye (Invitrogen, Carlsbad, CA) at room temperature for one hour. The other aliquot was incubated with an anti-EpCAM antibody (Abcam) and anti-PDPN antibody (Angiobio, San Diego, CA) in the presence of DNA staining Hoechst 33342 dye at room temperature for one hour. After several washes and centrifugation to remove the supernatants, the cell pellets were re-suspended, and the Alexa Fluor 488-conjugated donkey anti-mouse antibody (for TSHR and EpCAM) and Alexa Fluor 555-conjugated goat anti-rat antibody (for PDPN) were added to the cell suspension. The unbound antibody was removed after incubation in the dark for 30 minutes. The complete cell aliquot was placed on a slide, and the full immunofluorescence images were captured using fluorescence microscopy with an automated slide scanning platform (Zeiss Axiovert 200M) followed by image analysis using the IN Cell Analyzer 1000 Cellular Imaging and Analysis System (GE Healthcare Life Sciences, Pittsburgh, PA). EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs were the Hoechst-positive cells that were positive for EpCAM, TSHR, and PDPN, respectively.
Statistical analysis
Categorical data were compared using Pearson's chi-square test or Fisher's exact test. All data are expressed as the mean ± standard error of the mean. Univariate analysis and multivariate analysis by Cox proportional hazards regression model were performed to determine the significance of various factors (30). A p-value of <0.05 was considered statistically significant. Survival analysis was performed by using the Kaplan–Meier method and was compared using the Breslow and Mantel–Cox tests. Receiver operating characteristic (ROC) curve analysis was used to define the best cutoff value for remission and disease-specific mortality (DSM).
Results
Of the 128 enrolled cases, 67 (52.4%) patients were aged >44 years. A total of 119 (93%) patients were histologically diagnosed with PTC and another nine with follicular, Hürthle cell, and poorly differentiated thyroid carcinomas (Table 1). The mean tumor size was 2.5 ± 1.6 cm, including 35 (27.3%) cases with microcarcinomas (≤1.0 cm). A total of 108 patients underwent total thyroidectomy with or without lymph node dissection. Surgical pathological features illustrated 25 (19.5%) cases with microscopic extension to the perithyroidal tissue and 22 (17.2%) cases with gross extrathyroidal extension. After surgery and thyroid remnant ablation with 131I, 22 (17.2%) cases were diagnosed with distant metastases, and 43 (33.6%) cases were in non-remission status. A total of 42 (32.8%) cases received cumulative 131I activities >200 mCi. In addition, 61 (47.7%) cases had a postoperative Tg level of >10 ng/mL.
Experiments were performed to validate the antibodies that were used for identifying subpopulation of CEC expressing EpCAM, PDPN, or TSHR. First, immunofluorescence staining of white blood cells and cancer cell lines expressing EpCAM (OECM1 cells), PDPN (OECM1 cells), and TSHR (HepG2 cells) were performed by using the respective antibodies (Fig. 1A–D). Second, 293T cells were transfected with control vector or with the expression plasmids encoding EpCAM, PDPN, and TSHR followed by immunofluorescence staining using the respective antibodies (Fig. 2A–C). Both sets of data indicate that the antibodies used in this study specifically recognize EpCAM, PDPN, and TSHR.
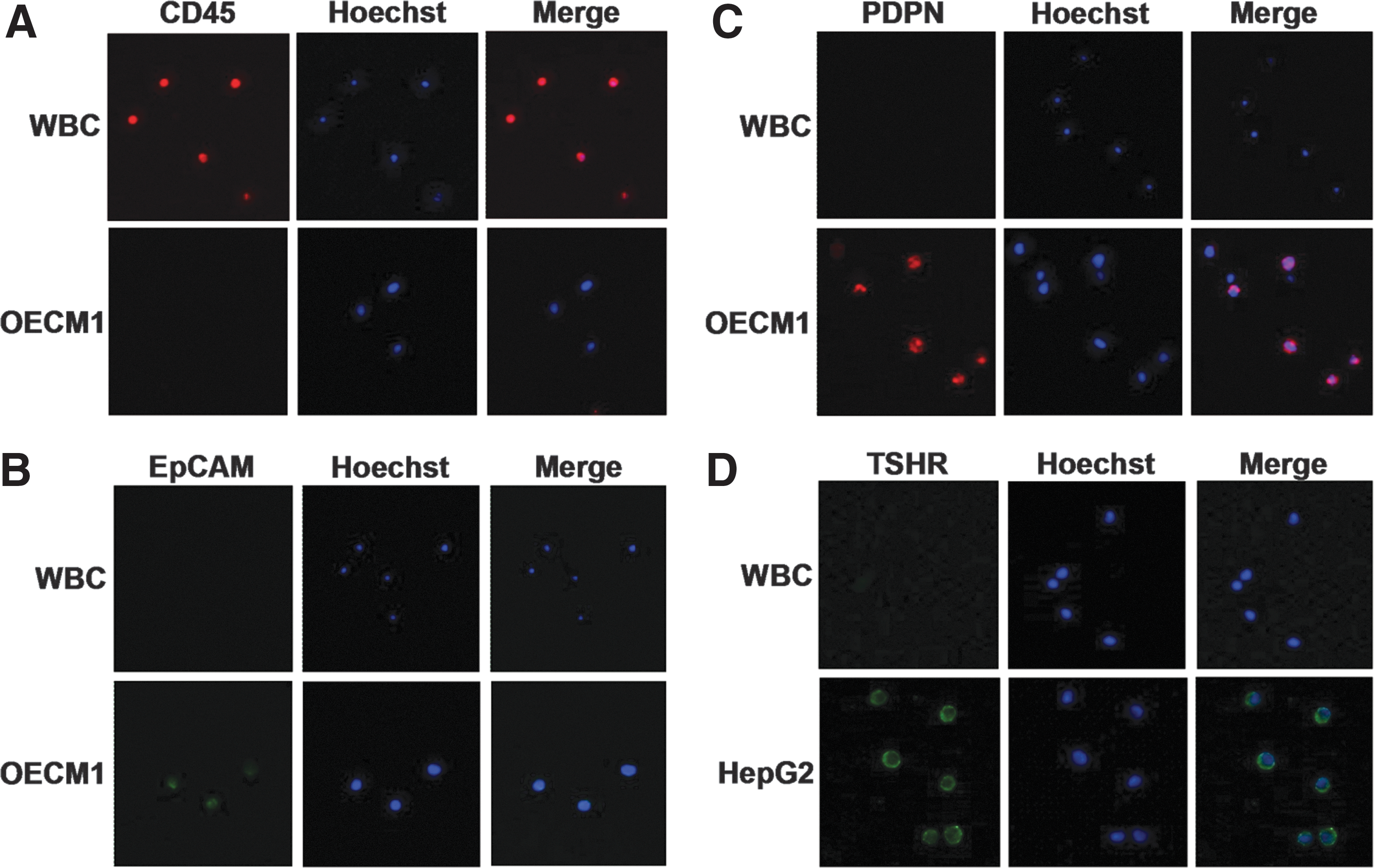
Immunofluorescence staining of leukocytes and cancer cell lines expressing epithelial cell adhesion molecule (EpCAM), podoplanin (PDPN), and thyrotropin receptor (TSHR). (
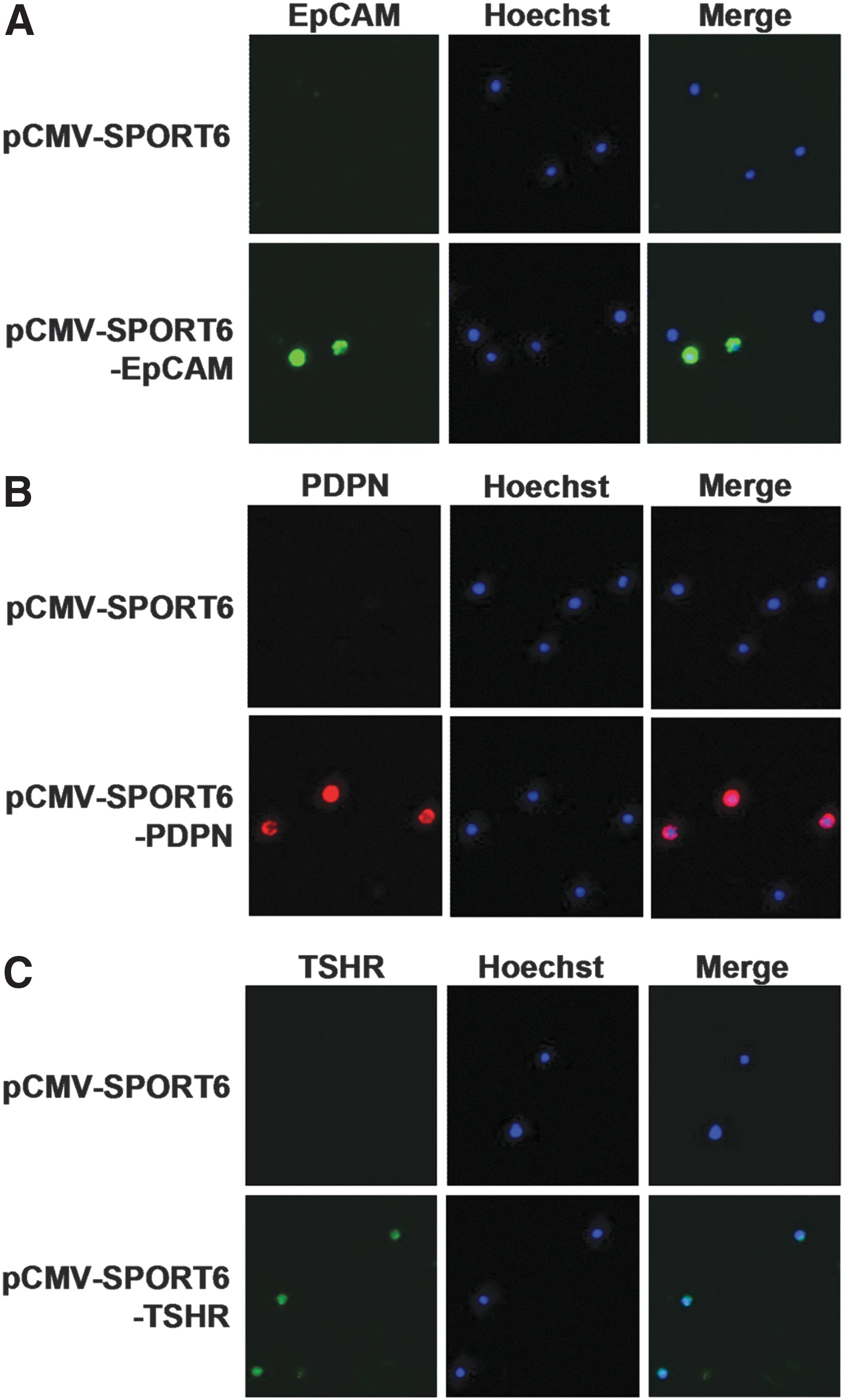
Immunofluorescence staining of HEK293T cells expressing EpCAM, PDPN, and TSHR. (
Fresh blood samples from patients four to six weeks after thyroidectomy or radioactive iodide therapy (131I) were processed through lysis of RBC and depletion of CD45+ leukocytes using the PowerMag system. The enriched cells were analyzed through immunofluorescence staining using the anti-EpCAM, PDPN, and TSHR antibodies (31,32). Hoechst 33342 was used to identify nucleated cells. Fluorescence microscopy analysis was performed to identify the CECs expressing EpCAM, PDPN and TSHR. Representative CECs positive for EpCAM, PDPN, or TSHR are shown in Figure 3A–C.

Isolation and characterization of circulating epithelial cells (CECs) from patients with thyroid cancer. (
At the end of follow-up, patients were categorized into non-remission and remission groups (Table 2). A total of 43 cases comprise the non-remission group, including 17 cases with DSM. Prognostic factor analysis revealed that age, tumor size, tissue with gross extrathyroidal extension, distant metastasis, TNM stages I and IV, Tg level, and CEC count (EpCAM+, TSHR+, and PDPN+) were statistically different between the remission and non-remission groups. In addition, DSM analysis demonstrated that age, tumor size, tissue with gross extrathyroidal extension, distant metastasis, TNM stages I and IV, and CEC count (EpCAM+, PDPN+, and TSHR+) were statistically different between the DSM and survival groups (Table 3). Multivariate analysis illustrated that age, sex, EpCAM+-CECs, PDPN+-CECs, and TSHR+-CECs were statistically different between the survival and DSM groups (Table 4). Furthermore, analysis was performed of patients who had papillary thyroid microcarcinomas (n = 24). No statistical difference was found when the number of CECs was compared between the non-remission (n = 2) and the remission (n = 22) group, and the DSM (n = 2) and the survival (n = 22) group for patients with papillary thyroid microcarcinomas (data not shown). It is likely that the total number of patients with papillary thyroid microcarcinomas is not sufficient for analysis. In particular, only two patients were in the non-remission and DSM groups. Further studies focusing on recruiting more patients with PTC <1 cm is required to address this important issue.
Values are shown as the mean ± standard deviation or n (%).
Eleven cases were without tumor size.
Postoperative 131I accumulative dose.
LN, lymph node; TNM, tumor-node-metastasis; CEC, circulating epithelial cell; EpCAM, epithelial cell adhesion molecule; PDPN, podoplanin; TSHR, thyrotropin receptor.
Values are shown as the mean ± standard deviation or n (%).
Eleven cases were without tumor size.
Postoperative 131I accumulative dose.
Dependent variable: survival vs. mortality.
ROC analysis showed that the number of EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs distinguished the remission from non-remission status with an area under the curve (AUC) equivalent to 0.782 (p < 0.0001), 0.688 (p = 0.0005), and 0.761 (p < 0.0001; Fig. 4A). The cutoff point for EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs was 40, 47, and 14 (cell/mL), with the accuracy of the assay equivalent to 80.4%, 76.6%, and 77.3%, respectively. In addition, ROC analysis showed that the number of EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs distinguished mortality from survival status with an AUC equivalent to 0.760 (p = 0.0006), 0.733 (p = 0.0020), and 0.748 (p = 0.0010), respectively (Fig. 4B). The cutoff point for EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs was 27, 25, and 9 (cell/mL), with the accuracy of the assay equivalent to 69.5%, 67.2%, and 68.5%, respectively. Analysis using cutoff points showed that the number of CECs with the three markers in the DSM group is statistically higher than when compared to the survival group (p < 0.0001; Fig. 5A–C).
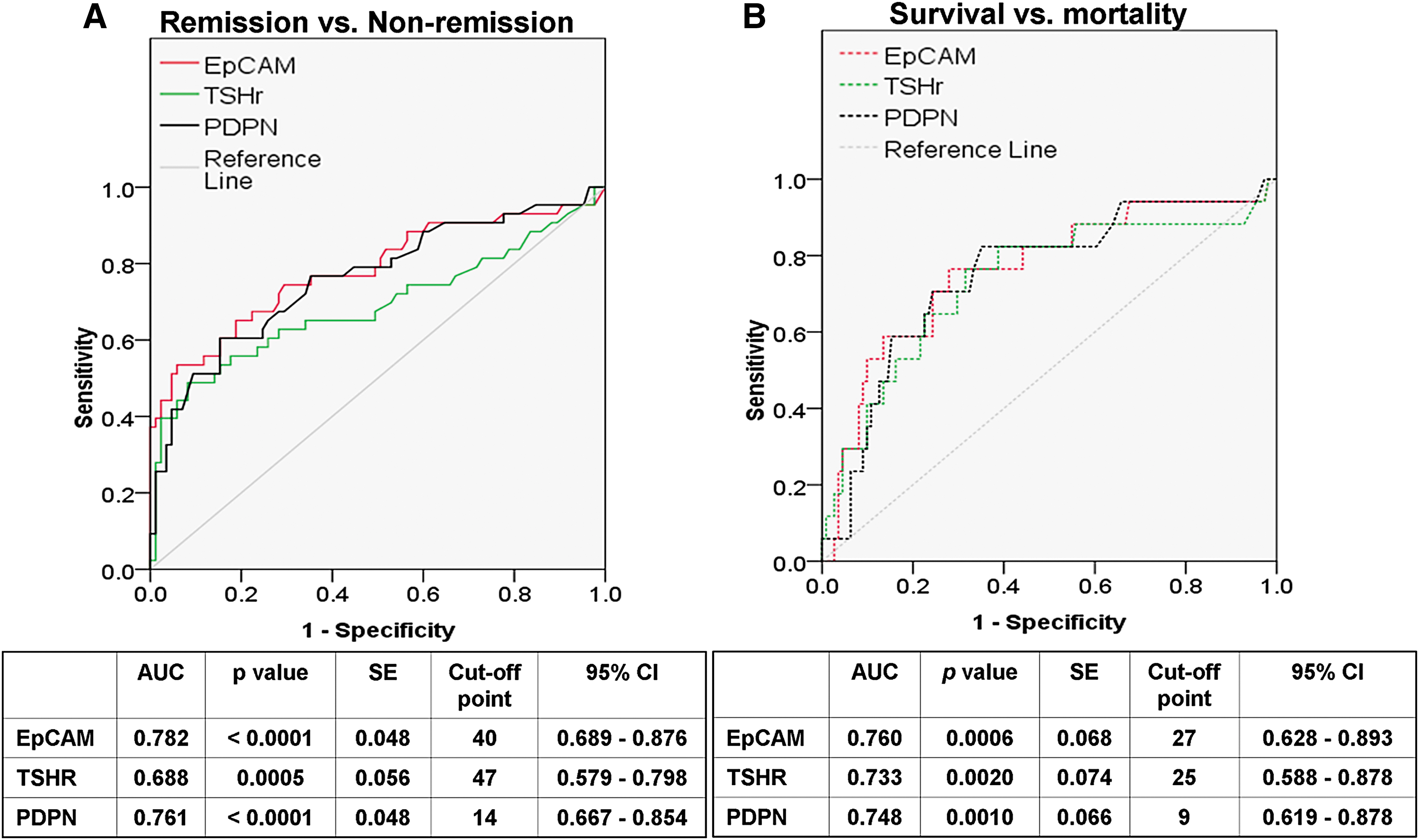
Receiver operating characteristic (ROC) analyses of CEC counts from patients with thyroid cancer. (
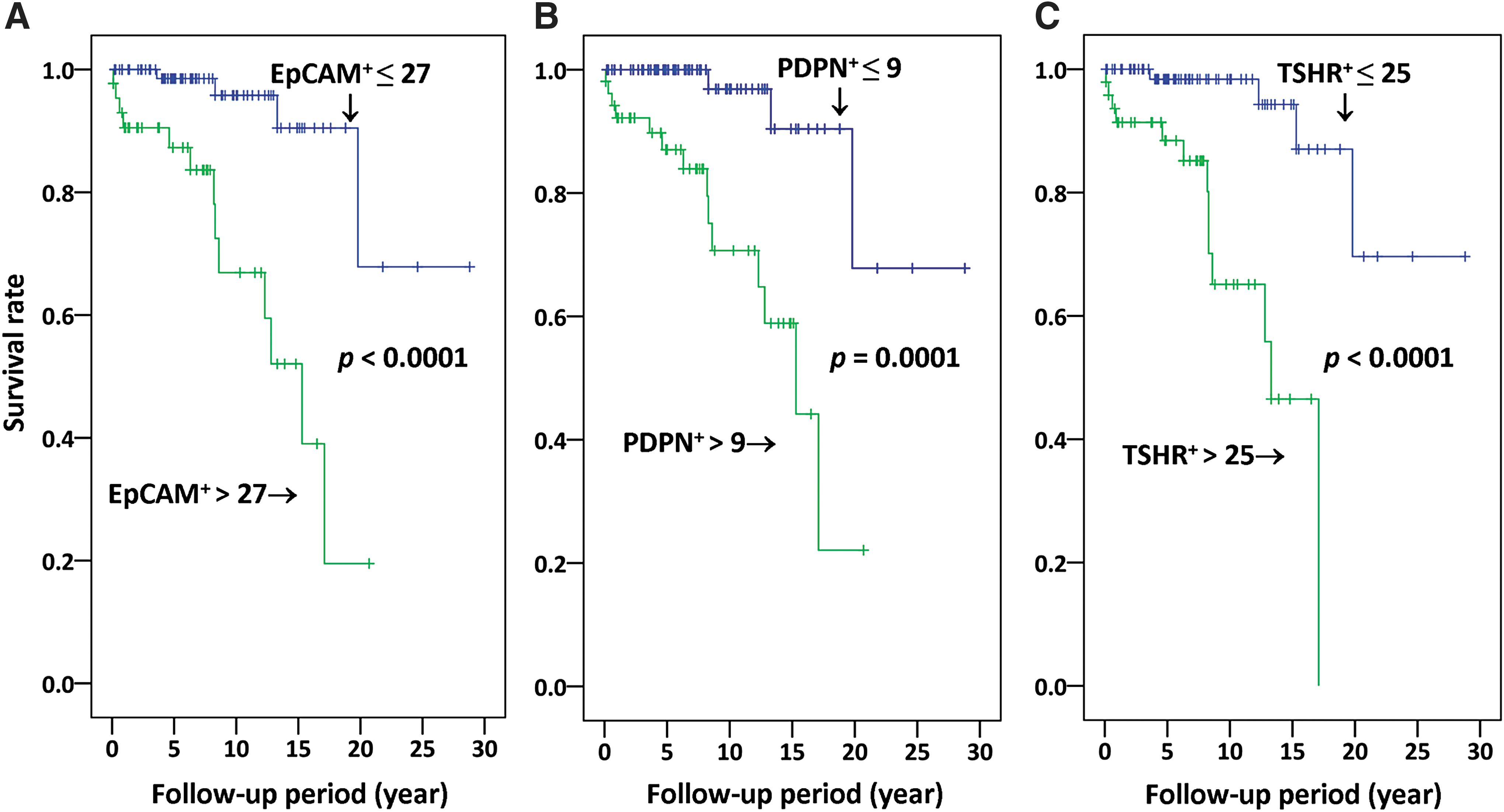
Kaplan–Meier survival curves of patients with thyroid cancer. (
Discussion
The presence of CECs in the bloodstream is considered a prognostic factor for poor survival in different cancer types (33 –35). Patients with well-differentiated thyroid cancer tend to have excellent prognosis after treatment. However, distant metastases may occur and threaten the life of patients (6). To date, the correlation of the number of CECs with overall survival of patients with thyroid cancer is still unknown. This study reports for the first time that the number of EpCAM+-CECs, TSHR+-CECs, and PDPN+-CECs is statistically higher in the non-remission group than in the remission group. The CEC count is also higher in the DSM group than in the survival group. This study highlights that the CEC count may be a prognostic factor for predicting the overall survival of patients with thyroid cancer.
CEC characterization has been shown to facilitate the identification of a patient with early-stage PTC and follow-up of disease status post thyroidectomy (19), define and monitor the therapeutic outcome of patients with PTC (20), and supplement serum Tg testing and medical imaging analysis for distinguishing disease status of patients with PTC (11). This study continues the authors' long-term effort and explores the clinical applications of CEC characterization in the management of patients with thyroid cancer. It is demonstrated that the overall survival of patients with thyroid cancer is closely related to the levels of CECs in the bloodstream.
At present, the prognostic relevance of CECs/CTCs in cancer patients is still controversial. A large cohort study of patients with breast cancer at the time of primary diagnosis and from the prospectively randomized multicenter SUCCESS-A trial (EudraCT2005000490-21) did not demonstrate prognostic values of CTCs, as quantified by an immunocytochemistry method (36). On the other hand, a meta-analysis of patients with triple-negative breast cancer provided strong evidence that CTCs in the peripheral blood is an independent prognostic factor of poor survival outcomes (37). Using the CellSearch system for CTC enrichment and characterization of blood from 18 patients with distantly metastatic medullary thyroid cancer indicated that the presence of five or more CTCs is associated with worse overall survival of patients (18). However, the conclusion is limited by the number of patients enrolled in the study. By analyzing a large cohort of 128 patients with thyroid cancer, the current data provide strong evidence that in addition to age and sex, the number of CECs were statistically different between the remission group and the non-remission group. In addition, patients with a high CEC count above a specific cutoff value usually have a significant shorter overall survival, regardless of whether EpCAM, PDPN, or TSHR is used as the CEC marker. Similar results were observed when CECs with simultaneous expression of EpCAM and PDPN (i.e., EpCAM+PDPN+-CECs) were analyzed (data not shown). CEC testing thereby could be considered as a potential clinical test for monitoring treatment response and prognosis of patients with thyroid cancer.
Different subtypes of CECs are present in the bloodstream. In addition to the common epithelial cell marker EpCAM, CECs expressing PDPN and TSHR were identified in the peripheral blood of patients with thyroid cancer. PDPN is a 38 kDa mucin-type I transmembrane glycoprotein known as a marker of lymphatic endothelial cells (38). In a recent study, PDPN expression was evaluated in patients with PTC and thyroid cancer cell lines derived from papillary (TPC1 and BcPAP) and follicular (FTC133 and CGTH-W-1) thyroid carcinomas using reverse transcription polymerase chain reaction, Western blotting, immunofluorescence staining, and immunohistochemistry (21). Results of this study demonstrated that PDPN mediates the invasiveness of cells derived from PTC, consistent with the current data demonstrating that an increase in the number of CECs expressing PDPN is a prognostic factor for poor survival of patients with thyroid cancer. On the other hand, thyroid follicular cells are the major cell types to express TSHR, although TSHR can also be found in nonthyroidal tissues (23). Although both PDPN and TSHR are not only expressed in thyroid cells, there is a minimal impact on their use as prognostic markers for patients who are diagnosed with thyroid cancer. These markers could also have prognostic value by supplementing other clinical factors or markers such as Tg in clinical surveillance of disease status.
This large prospective study was designed to perform CEC testing after thyroidectomy with or without radioactive iodine therapy (131I). The procedure of thyroidectomy may trigger the release of cancer cells into the peripheral blood (12,39) and cause an increase in the number of CECs. Hence, the time interval between surgery and blood collection for CEC testing must be taken into consideration. In this study, blood sampling was usually performed four to six weeks after surgical intervention in order to minimize its potential effect on the results of CEC testing. This time interval is also appropriate for Tg testing, and both tests can be performed simultaneously with a single blood draw. Combined analysis of CECs and Tg testing may assist in the clinical management of patients with thyroid cancer.
In conclusion, this study, together with previous reports (11,20), demonstrates that CEC testing is a useful tool for detecting residual disease, monitoring treatment response, and predicting overall survival of patients with thyroid cancer. The value of CEC testing needs to be corroborated in larger prospective studies in order to assess its value as a clinical tool that may complement Tg measurements combined with imaging studies.
Footnotes
Acknowledgments
This work was supported by the Chang Gung Memorial Hospital (grant numbers CMRPG3E1901, CMRPD1C0551-3, CMRPD1E0181-3, CMRPD1F0611-2, and BMRP466); the Ministry of Science and Technology (grant numbers 102-2628-B-182-009-MY3, 103-2314-B-182-018-MY3, 105-2320-B-182-030, 105-2320-B-182-029-MY3, 106-2320-B-182-027-MY3, and 106-2314-B-182-042); and the Chang Gung Molecular Medicine Research Center (grant number EMRPD1F0121) to J.-D.L. and C.-P.T.
Author Disclosure Statement
No competing financial interests exist.