
Abstract
Background:
Fine-needle biopsy is the international standard for diagnostic evaluation of thyroid nodules. There is a lack of consensus regarding the optimal needle biopsy technique. The implementation of capillary action versus aspiration and the optimal needle gauge remain topics of debate.
Methods:
A systematic review of the Medline, Embase, and Cochrane databases was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Articles evaluating the effects of capillary action versus aspiration and needle gauge on success rates of fine-needle biopsy of the thyroid were assessed for inclusion. The primary outcome of interest was the rate of non-diagnostic cytopathology.
Results:
Twenty-four articles with a collective 4428 nodules were ultimately included in the review. Twenty articles evaluated capillary action versus aspiration, and six evaluated needle gauge. All but two studies were prospective, most of which were blinded trials with or without randomization. Using a random-effects model, capillary action was associated with a statistically significant reduction in the relative risk of non-diagnostic cytopathology (relative risk = 0.57 [confidence interval 0.34–0.92]; p = 0.02). There was a nonsignificant trend in favor of smaller needle gauges.
Conclusion:
Given the statistically significant deceased rate of non-diagnostic cytopathology with capillary action and the potential for increased pain and complications with larger needles without a proven benefit, needle biopsy of routine thyroid nodules should be performed without aspiration and with smaller needle gauges (24–27G).
Introduction
N
Non-aspiration needle biopsy, also known as a capillary action technique, relies on hydrostatic pressure to absorb tissue into the needle bevel. A number of studies have evaluated this technique in comparison to aspiration in the context of thyroid nodules, with varying results. There remains a lack of consensus with respect to capillary action versus aspiration, as well as the optimal needle gauge for thyroid biopsies. In this article, a systematic review and meta-analysis is performed of how these variables affect the diagnostic success of needle biopsy of thyroid nodules.
Methods
This systematic review was performed in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA;
Prospective and retrospective studies were considered. Series of <50 nodules were excluded. Studies that focused on a specific subset of thyroid nodules, such as calcified or hypervascular nodules, were excluded. Series that did not report rates of ND cytopathology were excluded. Studies employing the use of core, stylet, or spinal needles were excluded, as were studies employing the use of additional devices or technologies aside from a standard hollow-bore needle and syringe, with or without a syringe holder. Articles not available in the English language were excluded.
Statistical analysis was performed in the R statistical software environment (The R Foundation, Vienna, Austria) and Microsoft® Excel (Microsoft, Seattle, WA). The Metafor statistical package was used for meta-analysis (6). Relative risk ratios for ND results were generated using studies comparing capillary action to aspiration and those comparing smaller- to larger-gauge needles. A random-effects model was used to generate an estimated average risk ratio for all studies, as well as to perform a linear regression. A template developed by Neyeloff et al. was used to generate pooled weighted rates of ND tests when using capillary action, aspiration, smaller-gauge needles, and larger-gauge needles (7,8).
Results
Included studies
The systematic review schema used to identify eligible articles is shown in Figure 1. Of the 5722 initial hits, 5677 were excluded based on title, abstract, or redundancy. Of the 45 unique full-length manuscripts that were reviewed, nine were discarded for using modified needles or additional devices. Six were excluded for having a sample size of <50. Four articles were excluded for not reporting rates of ND cytopathology. Two foreign language articles were excluded. Twenty-four articles totaling 4428 nodules were ultimately included in the review (9 –32). Twenty studies compared capillary action to aspiration, and six compared needle gauges (Tables 1 and 2). Two studies reported on both variables (14,26).
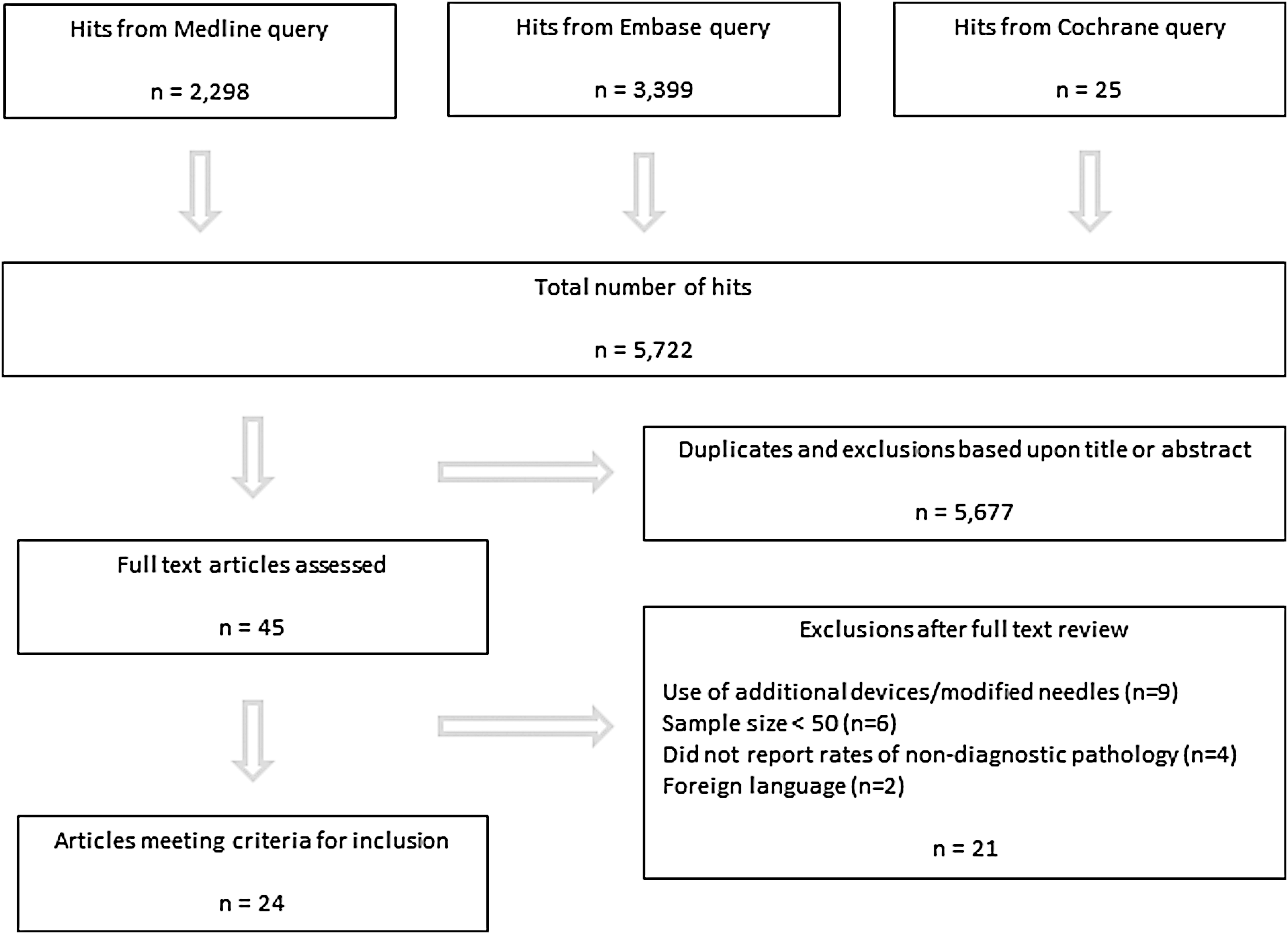
Systematic review flowchart.
N, number of nodules; ND, non-diagnostic.
All but two studies were prospective (92%) (27,32). Of the 24 studies, 16 (67%) employed a prospective design in which the same thyroid nodule was biopsied via two or more different techniques after which the samples were sent to a blinded pathologist (9,10,12,13,15 –17,19 –24,29 –31). The remaining six prospective studies (25%) assigned individual nodules to different biopsy techniques (11,14,18,25,26,28). Some authors chose to perform one technique prior to another for all nodules (i.e., aspiration prior to capillary action), whereas others used randomization to assign some patients to aspiration prior to capillary action and vice versa. Authors typically performed three to four needle passes for each biopsy attempt. Of the 24 studies, eight (33%) confirmed the use of ultrasound guidance for all nodule biopsies (14,16,22,26,28,29,31,32). The majority of the remaining studies employed ultrasound to varying degrees. Three studies (13%) did not use ultrasound at all (13,15,25). Twelve of the included studies came from Asia (50%), five from the Middle East (21%), three from Europe (13%), three from North America (8%), one from Africa (4%), and one from South America (4%; Tables 1 and 2).
Capillary action versus aspiration
Of the 20 studies evaluating capillary action versus aspiration, 3762 individual nodules were reported collectively (9 –28). All of the studies employed the use of standard, hollow-bore needles ranging from 22G to 27G. In sum, 430/3126 capillary action attempts resulted in ND cytopathology (13% [confidence interval (CI) 9.8–16%]; Table 3). For aspiration, 441/2828 attempts resulted in ND cytopathology (16.1% [CI 12.6–18.8%]). Using a random-effects model, capillary action was associated with a statistically significant reduction in the relative risk of ND cytopathology (relative risk [RR] = 0.57 [CI 0.34–0.92]; p = 0.02; Fig. 2). There was moderate heterogeneity between studies (I 2 = 60%).
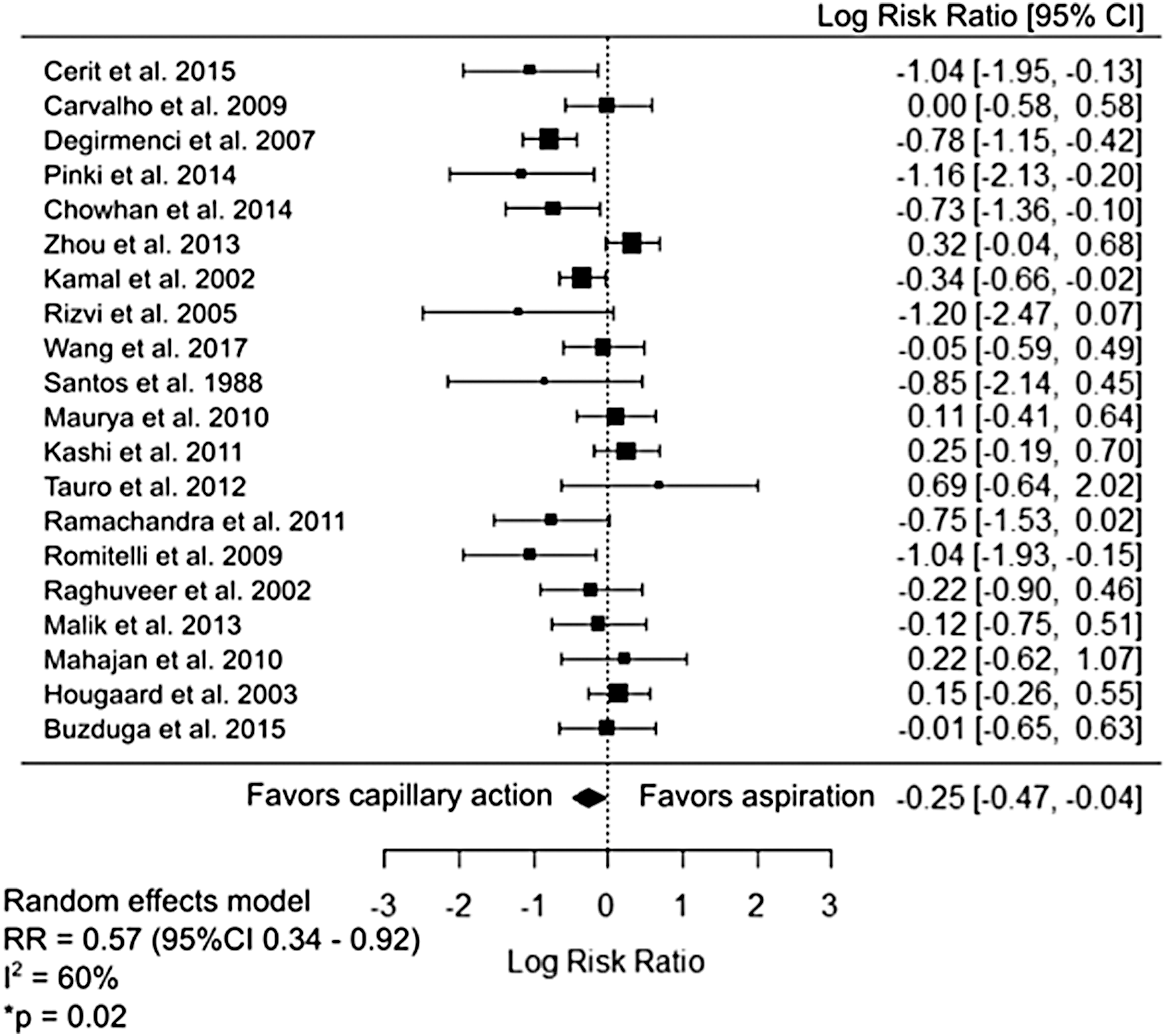
Forest plot of capillary action versus aspiration.
Random-effects model used to calculate pooled rates of non-diagnostic results across studies.
CI, confidence interval.
Smaller versus larger needle gauge
Of the six studies evaluating needle gauge, 1298 individual nodules were reported collectively (14,26,29 –32). Four of the six studies used a 27G for the smaller needle, one used a 25G, and one used a 24G (Table 2). Three studies used a 21G for the larger needle, two used a 22G, and one used a 23G. Aspiration, capillary action, or both techniques were employed for both needle sizes in each study. For the smaller-gauge needles, 110/816 attempts resulted in ND cytopathology (13.7% [CI 8.0–9.5%]; Table 3). For the larger needles, 176/819 attempts resulted in ND cytopathology (19.2% [CI 9.6–28.8%]). Using a random-effects model, there was a nonsignificant trend toward a reduction in the relative risk of ND cytopathology when using smaller needles (RR = 0.60 [CI 0.24–1.50]; p = 0.27; Fig. 3). There was moderate heterogeneity between studies (I 2 = 62%).
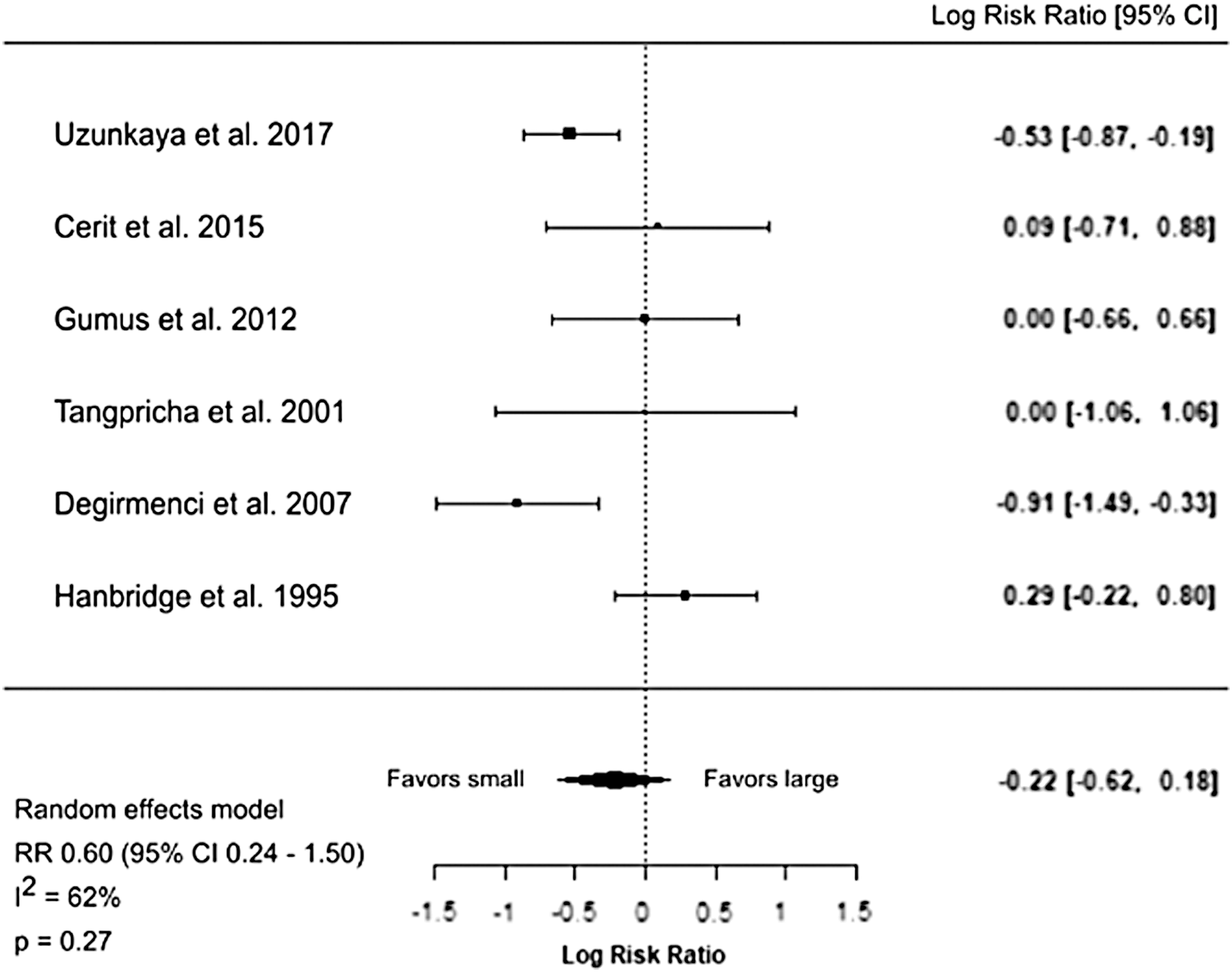
Forest plot of smaller versus larger needle gauge.
Regression analysis evaluating the rates of ND cytopathology for capillary action versus aspiration when controlling for needle gauge
Seventeen studies that reported both needle gauge and capillary action versus aspiration were included for linear regression (9 –13,15 –17,19 –26,28). The effect of needle gauge on the relative risk of ND cytopathology when using capillary action versus aspiration was studied using a random-effects model within the Metafor statistical package. Four of these studies reported using two different needle gauges, and the average between these was used (e.g., 22 and 23 gauge was reported as 22.5 gauge) (10,11,13,20). The estimated model coefficient for needle gauge was −0.08 ([CI −0.29 to 0.13]; p = 0.43), indicating no significant effect of needle gauge on the relative risk of ND cytopathology in this model (Fig. 4).
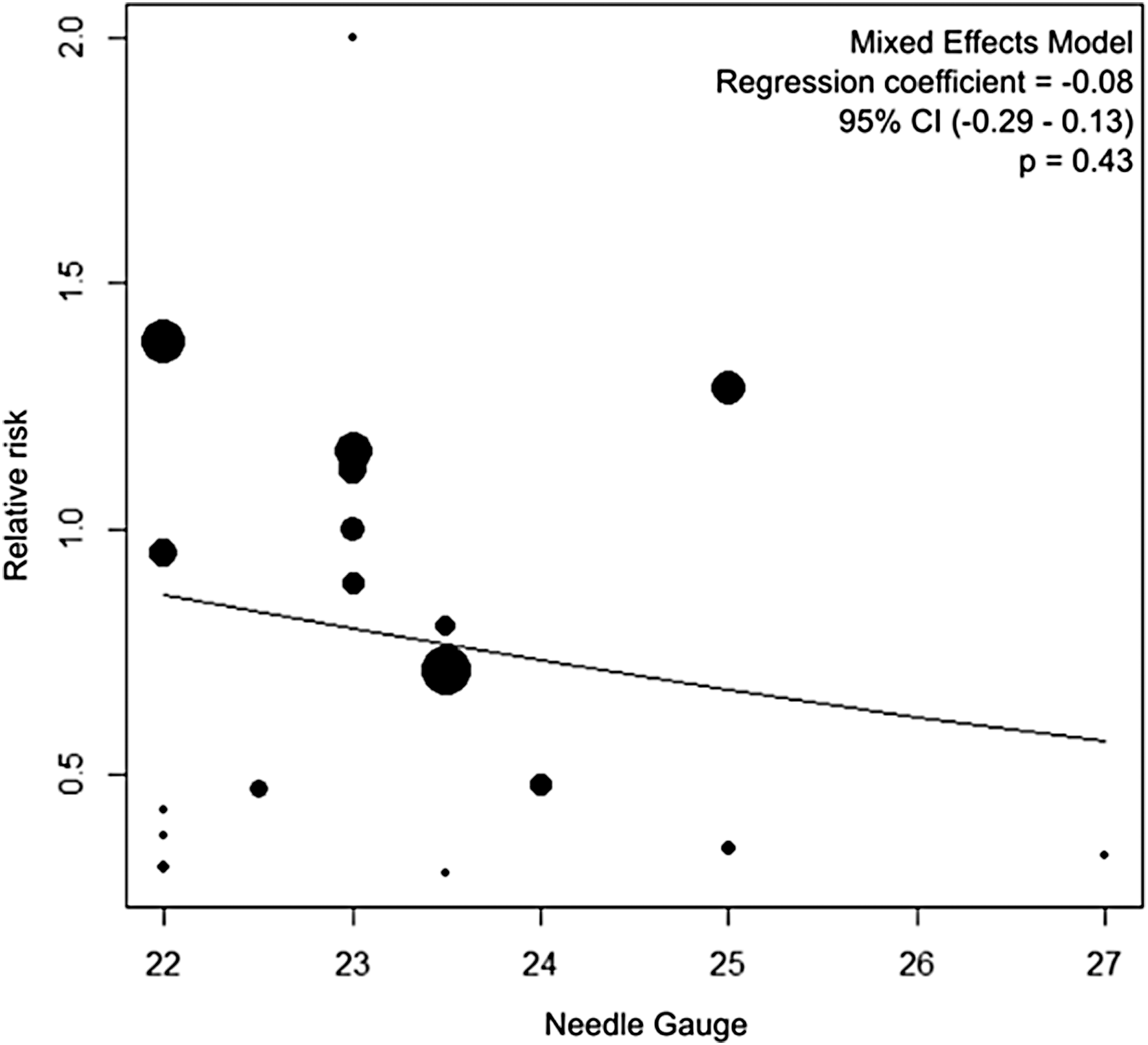
Linear regression of needle gauge and capillary action versus aspiration.
Discussion
The studies included in this review represent a collection of predominantly prospective, blinded trials with a relatively low risk of bias (33). A statistically significant reduction in the rate of ND cytopathology was found using the capillary action technique relative to aspiration (RR = 0.57 [CI 0.34–0.92]; p = 0.02). Most notably described by Santos in 1988, non-aspiration needle biopsy is currently widely utilized (9). With this technique, in contrast to aspiration, thyroid tissue is passively pulled into the needle hollow via hydrostatic forces. This may increase the diagnostic success by avoiding blood contamination, a notorious problem in the interpretation of thyroid cytopathology (3).
The effect of needle gauge on ND thyroid cytopathology has not been evaluated as extensively as capillary action versus aspiration. Larger needle gauges, although theoretically capable of harvesting more tissue volume, do not appear to decrease the rate of ND cytopathology, as evidenced by a nonsignificant trend in favor of smaller needle gauges. Although very uncommon, fine-needle biopsy of the thyroid can result in serious complications such as infections, vocal cord paralysis, and, most notably, hematomas (34 –37). Given the potential for increased pain and complications with no demonstrated benefit, initial biopsy of routine thyroid nodules with larger-gauge needles is not advised.
The force of capillary action is dependent upon several variables, including the fluid density, the gravitational force, and the radius of the cylinder into which a sample is being absorbed (9). To account for a potential interrelationship between needle gauge and the effects of capillary action versus aspiration, a linear regression was performed. A nonsignificant result was obtained, thus indicating no clinically significant interrelationship between these variables within the available data.
This review is limited in a variety of ways. Although most of the included studies were prospective and blinded, the majority were not randomized and, as such, are subject to biases. Between different institutions, varying levels of experience and skill of those obtaining and interpreting the cytopathology may serve as a confounder. In the United States, ultrasound guidance is currently largely standard of care for performing thyroid nodule biopsies. Importantly, of the 24 studies, only eight (33%) confirmed the use of ultrasound guidance for all biopsies (14,16,22,26,28,29,31,32). The lack of consistent use of ultrasound among the included studies may represent a confounder that could also result in increased rates of ND attempts. This review has analyzed the rate of ND cytopathology, arguably the most important outcome when assessing needle biopsies. Nonetheless, there are many other qualitative and quantitative criteria by which fine-needle cytopathology can be analyzed, and it is not possible to comment on these (38). This review included studies evaluating general thyroid nodules, which are a diverse entity that includes benign and malignant pathology with a myriad of anatomic features. It is possible that certain subtypes of nodules are more adequately sampled with aspiration or with larger needles. For nodules with multiple ND biopsies, larger diameter or core needles may be advantageous (39,40). Lastly, there are a variety of negative pressure devices and modified needles that have shown promise as adjunct technologies in needle biopsy of the thyroid. The exclusion criteria precluded these studies from being included in this review (41 –43).
Conclusion
There are a number of prospective studies evaluating the effects of capillary action versus aspiration and needle gauge on the diagnostic success of thyroid biopsies. Given the statistically significant deceased rate of ND cytopathology with capillary action and the potential for increased pain and complications with larger needles without a proven benefit, needle biopsy of routine thyroid nodules should be performed without aspiration and with smaller needle gauges (24–27G).
Footnotes
Acknowledgments
The authors thank Karen Messer, PhD, and Emily Pittman, PhD, of the UC San Diego Biostatistics Department for their assistance with the statistical analysis.
Author Disclosure Statement
No competing financial interests exist.