
Abstract
Amiodarone-induced thyrotoxicosis is a common complication of long-term amiodarone treatment. In a patient with amiodarone-induced lung toxicity and amiodarone-induced thyrotoxicosis type 2 (AIT2), a “white thyroid” was incidentally observed on an unenhanced chest computed tomography (CT) scan. This “white thyroid” resembled a thyroid image on a contrast-enhanced CT scan. Therefore, the thyroid density was prospectively evaluated on unenhanced CT scans in cases of AIT2, in euthyroid patients on amiodarone (AEuth), and in unexposed controls. The aim was to test the hypothesis of a higher thyroid density in AIT2 compared to AEuth. The thyroid density, as measured in Hounsfield Units on unenhanced CT scans, is higher in AIT2 compared to AEuth and much higher than in controls. The causality of this association and its potential diagnostic use require further study.
Introduction
A
The pathogenesis of AIT2 is incompletely understood. Amiodarone is a benzofuranic iodine-rich drug with extensive tissue distribution. Damage to the follicular cells is believed to be due to direct drug and/or iodine exposure, assuming a high intrathyroidal drug concentration (1). Thyroid iodine concentration has not yet been investigated in amiodarone-treated patients.
An incidental observation of a “white thyroid” (Fig. 1A) in a case of AIT2 led to the study of thyroid density as a proxy of thyroid iodine concentration. Indeed, a linear correlation between iodine concentration in thyroid tissue and thyroid computed tomography (CT) scan density has previously been described (4,5).
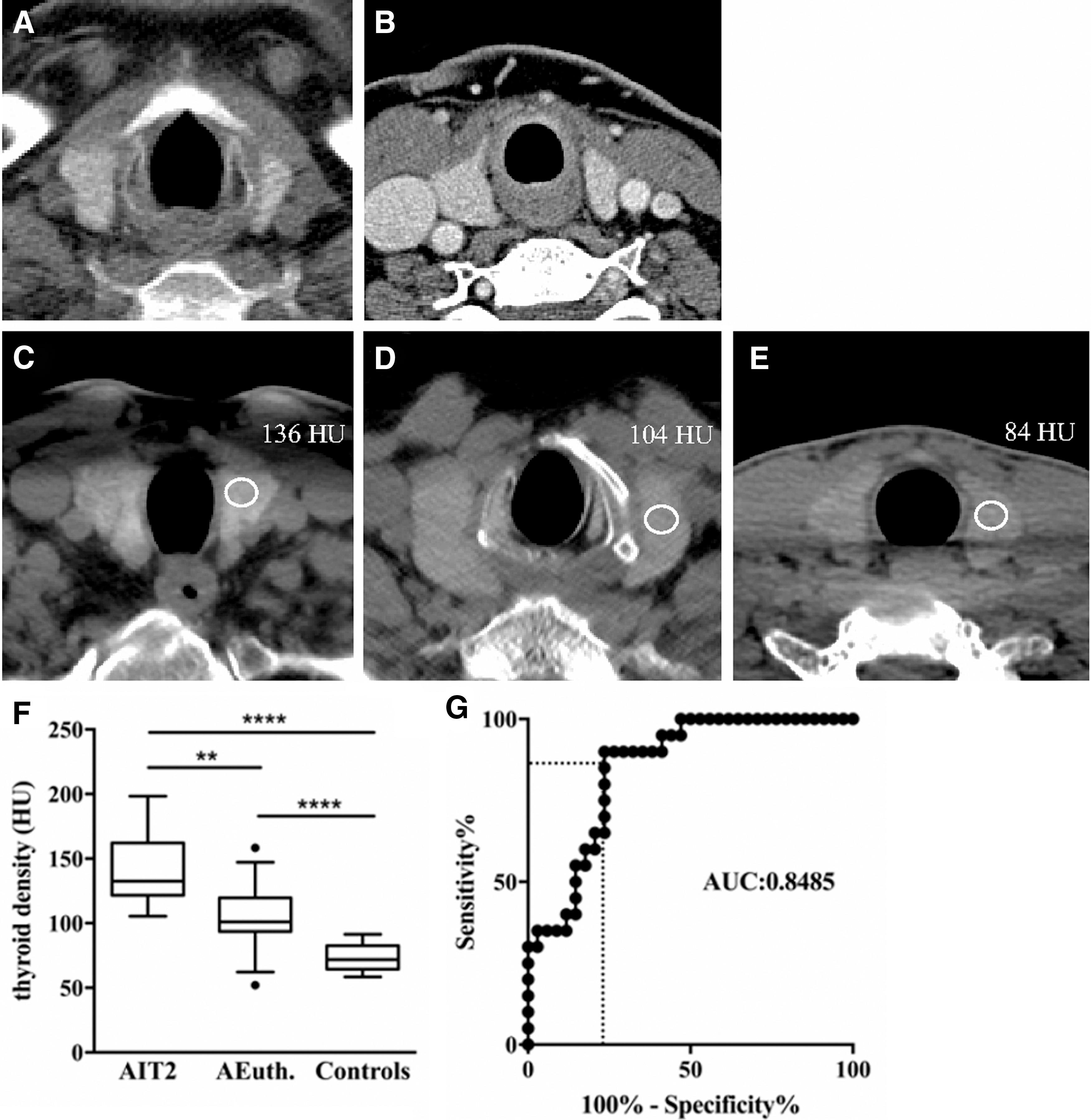
Thyroid computed tomography (CT) in the subject with the “white thyroid” on an unenhanced chest CT scan performed for lung toxicity, identified as an incidental observation in the course of an evaluation of amiodarone-induced thyrotoxicosis type 2 (AIT2; mean thyroid density: 145 Hounsfield Units [HU]). The image resembles a contrast-enhanced thyroid, except for the non-enhanced blood vessels (
It was hypothesized that a higher thyroid density in AIT2 compared to AEuth would be in line with a high amiodarone concentration-induced follicular disruption, the plausible key mechanism of AIT2 (1).
Methods
Consecutive AIT2 and AEuth patients at Sint Jan's Hospital were prospectively included (1/2011-4/2015; IRB permission B049201316794).
The four criteria to be met for AIT2 were: amiodarone treatment for more than three months, thyrotoxicosis (free thyroxine [fT4] >1.5 upper limit of normal and/or elevated free triiodothyronine [fT3], and thyrotropin [TSH] <0.1 mIU/L), a normal-sized homogeneous thyroid with normal/reduced vascularity on CFD-US, and absence of thyroid autoimmunity. The treatment for AIT2 consisted of methylprednisolone, mostly in combination with thiamazole. In refractory cases, additional therapies included perchlorate, cholestyramine, and/or thyroidectomy.
Inclusion criteria for AEuth included amiodarone treatment for more than three months, normal TSH, thyroid palpation, and indication for a CT scan for nonthyroidal clinical reasons.
Exclusion criteria were a prior history of thyroid disease, thyroid peroxidase (TPO) antibodies ≥50 kIU/L or thyroid-stimulating immunoglobulin ≥2 IU/L, and the use of iodine-containing medication or iodine-containing contrast enhanced exams in the preceding three months.
The study procedure consisted of a focused unenhanced neck CT scan obtaining three slices of the thyroid gland with a 64-slice MDCT (DiscoveryCT750HD; General Electric, Milwaukee, WI) at 120 kV. The thyroid density was measured on both sides, and the mean value of the two measurements was taken into account. The median estimated dose length product (DLP) was 204.6 mGy x cm (estimated effective dose 1.36 mSv; DoseWatch 2.0.4).
Normal thyroid densities were obtained from 24 unenhanced cervical spine CT images at 120 kV, excluding subjects with exposure to iodine contrast agents/amiodarone in the preceding six months.
Biochemistry and statistical analysis are provided in the Supplementary Data (Supplementary Data are available online at
Results
In total, 20/22 AIT2 and 34/41 AEuth patients enrolled met the inclusion criteria. Baseline characteristics are depicted in Table 1. In AIT2, the median time to normal thyroid function tests was 28.5 days; in four patients it was ≥90 days. Three subjects, including the subject with the highest thyroid density (198 Hounsfield Units), needed surgery.
Data are given as median and IQR.
AIT2 versus AEuth, **after Dunn's multiple comparison test the difference between AIT2 and AEuth remained significant (p-value <0.01) as well as the difference between AEuth and controls.
AIT2, amiodarone-induced thyrotoxicosis type 2; AEuth, euthyroid patients on amiodarone; BMI, body mass index; fT4, free thyroxine; fT3, free triiodothyronine; TSH, thytrotropin; CT, computed tomography; IQR, interquartile range; NA, not available; NS, not significant.
Overall, a significantly elevated thyroid CT density was found in AIT2 compared to AEuth (Fig. 1). Within study groups, CT densities in males and females were similar and were not correlated with age or body mass index. Within patient groups on long-term amiodarone, there was no correlation of CT density and duration of amiodarone treatment. In AIT2, no correlation was observed between CT density and fT4, fT3, or time to normal thyroid function tests. There was a correlation between thyroid density and number of treatments needed (r = 0.51; p < 0.05).
Discussion
After an incidental observation of a “white thyroid” on an unenhanced chest CT scan in an individual with AIT2, a high and very high thyroid density was confirmed in AEuth and AIT2, respectively. This finding is consistent with an elevated and markedly elevated thyroidal iodine concentration in AEuth and AIT2, respectively, and consistent with histology findings in AIT2. In pathology specimens of AIT2 patients, microscopy showed enlarged follicles besides spots of follicular destruction (6,7). Enlarged follicles, as described in AIT2, increase the ratio of follicular area to the entire tissue, and this ratio has been correlated with thyroidal iodine concentration (8). Histology examination also showed segmental follicular cell alterations containing enlarged lysosomes (6), and such lysosomal inclusion bodies have been implicated in amiodarone-induced skin, liver, and lung toxicity. In skin fragments showing toxicity, dermal macrophages showed more enlarged lysosomes containing iodine, likely within amiodarone/desethylamiodarone (9). Altogether, enhanced lysosomal amiodarone trapping in AIT2 might contribute to the higher thyroid density.
The question arises whether amiodarone accumulation is causally related with thyroid toxicity or just a non-causative hallmark of AIT2, and whether thyroid density could serve as a marker for AIT2. The observation of a higher thyroid density in AIT2 compared to AEuth with similar amiodarone exposure (>3 months; median around 30 months), together with the earlier observation of an early time-dependent rise in thyroid iodine content on amiodarone treatment (10), suggests a nonlinear process with interindividual variability of slope and/or leveling off.
Because of the limitations of this study (cross-sectional, limited study sample, absence of AIT1), a further prospective study is needed with minimal X-ray exposure. Facing the unpredictability of AIT2, thyroid density might enable the population at risk to be better delineated, but the optimal time frame has to be determined. Considering the protracted thyrotoxicosis in a subset of AIT2 patients, the question arises whether the characterization of thyroid density could be useful for predicting the clinical course (3).
In conclusion, AIT2 is characterized by a very high thyroid density in accordance with pathogenic mechanisms implicated in AIT2. A prospective study in subjects in need of long-term amiodarone therapy is needed to confirm this finding and to study high thyroid density as a possible herald and/or hallmark of therapy refractoriness in AIT2.
Footnotes
Acknowledgments
We thank B. Peene for the aid in recruitment of AEuth subjects, M. Langlois for the laboratory analyses, and R. Bouillon for the critical reading of this manuscript and continuous advice.
Author Disclosure Statement
The authors have no related disclosures.