
Abstract
Background:
Milk is a major source of iodine in human nutrition. Because both iodine content and the consumption of milk and dairy vary widely over time and populations, their contribution to iodine intake must be evaluated regularly. A recent national iodine survey found Israel's population to be mildly iodine deficient, possibly due to unmonitored changes in the food content of dietary iodine. Accounting for dairy iodine content can help guide efforts to prevent iodine deficiency.
Objectives:
This study aimed to determine the iodine concentration of dairy products typically consumed in the Israeli diet, and to estimate iodine intake from dairy products among Israeli adults.
Methods:
Iodine was analyzed in 33 selected dairy products that account for 89% of the total population's dairy intake according to the “MABAT” Israeli National Health and Nutrition survey. Based on these data, the distribution of iodine intake from milk, dairy, and dairy-based foods in the adult population was calculated.
Results:
Israeli milk is rich in iodine, with a mean concentration of 22 μg/100 g. However, due to low dairy consumption, the mean iodine intake from milk and dairy was only 34 μg/day (median 23 μg/day; range: 0–337 μg/day) or 22% of the recommended daily allowance. Self-reported intake among poor, male, and Arab subgroups was even lower.
Conclusions:
Because Israeli milk and dairy products are iodine rich, their contribution to the population's iodine intake would increase if they were consumed in greater amounts, particularly by high-risk groups. Dairy's potential contribution to iodine nutrition should be considered in recommendations for dairy consumption and iodine prophylaxis.
Introduction
A
The case of Israel highlights the importance of routinely monitoring a population's iodine intake. Israel is an industrialized state with a developed healthcare system (9), but along with other relatively populous countries, it does not provide iodine prophylaxis (e.g., universal salt iodization) (10), and until recently, the prevailing view was that the country was iodine sufficient due to the proximity of its population to the Mediterranean sea. However, trends for a significant rise in the self-reported use of thyroid treatment medication among Israeli adults (11,12) and for increasing and extensive use of iodine-depleted desalinated sea water suggested otherwise (12). Israel's first national iodine survey was conducted, and it was found that the population is mildly iodine deficient. The median urinary iodine concentration (UIC) was 83 μg/L for school-aged children and 61 μg/L for pregnant women. Sixty-two percent of the UIC samples from children fell below the World Health Organization's adequacy range for children of 100–199 μg/L, and 85% of pregnant women's samples fell below the adequacy range for pregnancy of 150–249 μg/L. At these levels, Israel now ranks in the lowest decile globally in terms of iodine status (13).
In order to develop an effective public-health response to prevent such deficiencies and to clarify the causes for their emergence, it is crucial to identify key sources of dietary iodine, such as milk and dairy products, whose contribution to the population's iodine intake may vary over time (14,15). Milk and dairy are among the most important sources of iodine in the human diet in many developed and developing countries (1,16). For example, they accounted for approximately 60% of iodine intake among Norwegians (15,17) and 40% of the total iodine intake for French children in 2013 (18). In many developing countries, milk consumption and the percentage of dietary energy derived from dairy foods nearly doubled between 1961 and 2007 (19), but this does not mean that iodine intake increased accordingly or that the trend has continued. Because patterns of both milk consumption and iodine content vary widely over time and place, the contribution of milk and dairy products to iodine intake must be reevaluated regularly and locally. Contextual changes, such as recommendations to restrict salt intake or changes in dairy farming, can reduce iodine intake in the population (2,7,15,20). For example, the iodophors typically used in dairies to sterilize teats and sanitize equipment prior to milking can contribute to milk iodine content (21 –23). In the late 1990s, Israeli dairy farmers were advised to use iodophor concentrations of 5000–10,000 ppm for teat disinfection, but by the late 2000s, the recommendation was to use 2000–4000 ppm or to use iodine-free alternatives (24 –26). Theoretically, such gradual changes in farming practice could significantly alter milk iodine content. Thus, in Israel and elsewhere, the long-term consistency of iodine content in milk, dairy, and other foods cannot be taken for granted.
For these reasons, this study was undertaken to estimate the contribution of milk and dairy products to iodine intake in Israel's population. This required information on the iodine content of milk and dairy products and on the level of their consumption by the population. However, data on iodine content for Israeli milk and dairy products are scant and outdated (11). Although dairy production in Israel is high, consumption may be low. While in 2015 local milk production in Israel was estimated at 178 L per capita per year (27), or enough to provide a total of approximately 491 g/day per capita, the equivalent of more than three daily servings (where one serving equals 150 g), production has decreased by approximately 20% since the mid-1990s (27 –29), possibly reflecting reduced consumption. The only available data on the dietary consumption of milk and dairy by a representative Israeli population come from The First Israeli National Health and Nutrition Survey (MABAT survey), which was conducted by the Ministry of Health between 1999 and 2001 (30). These data place per capita milk and dairy intake among Israeli adults at around only 150 g/day per capita, the equivalent of one serving. In view of the population's mild iodine deficiency, this study aimed to determine the current iodine concentration of Israeli milk and dairy products and to estimate their contribution to the populations' iodine intake.
Methods
Population nutrition survey
Data on milk and dairy consumption for the adult Israeli population were obtained from the MABAT survey conducted by Israel's Ministry of Health, with ethical approval as described elsewhere (30). The anonymous MABAT survey data are publically available and do not require ethical approval for further analysis. The MABAT survey took place between 1999 and 2001 among a nationally representative sample of men and women (N = 3426) aged 25–64 years. Itemized food intake, including the brand and quantity of all dairy products consumed, was recorded by trained professionals using a 24-hour recall dietary questionnaire (30). Self-reported use of multivitamin and mineral supplements was recorded. The question on nutrition supplement use was worded as follows: “During the past month, have you taken any nutrition supplements such as: multivitamins, vitamins, minerals, dietary fiber, fish oil, iron, or calcium?” If the answer was positive, each supplement was listed separately, including the name of the supplement, who recommended it (i.e., a physician, dietitian, alternative medicine practitioner, personal initiative, friends, family, commercial company or nature store, non-medical health professional, media, other, or don't remember), and how often it is taken (i.e., less than once a month, 1–3 times per month, 1–2 times per week, 3–4 times per week, 5–7 times per week). Intake of iodine containing supplements was noted by examining the manufacturer's labels for iodine content of the reported supplements.
Participants of the survey provided demographic data, including age, sex, pregnancy status, self-reported income, and belonging to one of the four main population groups in the Israeli society: Arab, Secular Jewish, Religious Jewish, and Ultra-Orthodox Jewish (15%, 63%, 12%, and 10% in the Israeli adult population, respectively) (31). Women aged 25–49 years were classified as being of childbearing age. Participants were classified by the survey as falling below the poverty line based on self-reported income and household size (30).
Dairy product selection and sampling
The dietary intake data from the MABAT survey was analyzed, and 26 dairy products, including liquid milk, were identified, which as a whole accounted for 89% of the population's weighted total dairy intake. These items were selected for analysis of their iodine content in addition to two soy milk beverages (sometimes perceived as a milk alternative) (32) and five new products (three types of Activia yogurt, organic milk, and Golan Heights Dairies milk), which came on the market more recently. In total, 33 products, listed in Table 1, were selected for purchase and analysis.
Product type (source in parentheses), product name, product subtype, fat percentage where relevant, and producer name.
Geographical and seasonal considerations
Dairy production in Israel is centralized and limited to several central dairies and production facilities (Tnuva, n = 2; Strauss, n = 1; Tara, n = 1; Yotvata, n = 1; Tzuriel, n = 1; Golan Heights Dairies, n = 1; and Harduf, n = 1). Geographical sampling of milk from individual farms was unnecessary because these dairies pool raw milk from farms situated throughout Israel, where the herds are predominantly fed in barns without grazing (19). Potential seasonal variability was taken into account by procuring samples of each product during early summer (May 2015) and early winter (December 2015). In both summer and winter, three samples of each item were purchased at one of seven different retail supermarkets and grocery stores, ensuring that each individual sample came from a different production lot. For every product, equal amounts of each seasonal replicate were pooled by volume or weight as appropriate, and then homogenized and stored at −20°C. Frozen, pooled samples were shipped on dry ice to the National Institute of Nutrition and Seafood Research (NIFES), Bergen, Norway, for further analysis.
Analysis of dairy iodine content
Iodine content was determined using inductively coupled plasma mass spectrometry (ICP-MS) after digestion in tetramethylammonium hydroxide (TMAH), as previously described (33). A test sample of 1 mL of milk or 0.1–0.2 g of solid material was added to 5 mL of deionized water and 1 mL of TMAH. Extraction was carried out in a dry oven at 90 ± 3°C for 3 h. After cooling, 1 mg/L of tellurium was added as internal standard to the sample solution and diluted to a final volume of 25 mL with deionized water. Prior to analysis, all samples were filtered through a 0.45 μm syringe filter. Certified reference material was used to measure the accuracy and precision of the method. Iodine content is reported as μg/100 g.
Population iodine intake from milk, dairy products, and dairy-based foods
The distribution and mean of iodine intake from milk and dairy were calculated on the basis of the MABAT survey data. Individual dietary iodine intake from milk, dairy products, and dairy-based foods was calculated for each survey participant by multiplying the amount of each product consumed by the mean iodine content for that product averaged over summer and winter. In addition to evaluating iodine consumed from the 33 analyzed products, iodine intake from 17 frequently consumed dairy-based foods was calculated based on the dairy content of the reported portions consumed. These foods included: cheese bourekas or sambusac (filled pastries), cheese-filled blintzes, cheese ravioli, kanafeh (a Middle Eastern cheese-based dessert), cheesecake, cheese-based pies, pizza, dairy-based omelet, milk-based porridge, malabi (a Middle eastern milk-based dessert), milk-based soup, salep (a Middle Eastern milk-based drink), milk-based semolina porridge, and milk added to coffee and tea.
Using the annual average iodine concentration of analyzed products, the study described the distribution and mean dairy iodine intake for the overall population, and stratified it by sex, pregnancy status, and self-reported societal sector, as listed in the MABAT survey, namely: Arab, Secular Jewish, Religious Jewish, and Ultra-Orthodox Jewish (30). Nonpregnant women aged 25–49 years were classified as being of childbearing age. Participants were further classified as above or below the poverty line according to the MABAT survey criterion, which was based on income in relation to self-reported household size (30). The proportional contribution of iodine provided by a cup of cow's or goat's milk at different ages and life stages was calculated according to the Recommended Daily Allowance (RDA) for iodine (34). One cup was considered as 240 mL (35).
Statistical analysis
Descriptive statistics and analyses were performed with JMP Pro software v13 (SAS Institute, Cary, NC). The distribution of estimated iodine intake from dairy in the overall population and subgroups was tested by Shapiro–Wilk W (normal distribution) and Cramer–von Mises W tests (Weibull distribution). Equality of variance across population subgroups was evaluated by both Levene and Bartlett tests. A nonparametric Kruskal–Wallis (rank sums) test was followed by Wilcoxon's test to compare differences between each pair of subgroups as appropriate. A two-tailed p-value of <0.05 was considered statistically significant.
Results
Iodine content of milk and dairy products
The seasonal and average annual iodine content of the 33 assayed milk and dairy products is given in Table 1. On average, cow's milk contained 22 ± 3 μg of iodine/100 g of milk (M ± SD), with similar values for 3% and 1% fat milk. Tnuva 3% fat milk, which is the most frequently consumed milk in Israel (30), had a concentration of 26 μg of iodine/100 g of milk. In absolute terms, there were only small seasonal variations in the milk produced by the main commercial dairies (Tnuva, Tara, Yotvata, and Golan Heights), ranging from 0 to 11 μg/100 g, with the exception of organic milk produced by the Harduf dairy that varied by 35 μg/100 g between a winter low of 6 μg/100 g and a summer high of 41 μg/100 g. This lack of seasonal variation may reflect dairy practice in Israeli farms. In contrast to North European countries where cows are housed indoors in the snowy months and graze in the summer, the reverse would be true of Israel, where vegetation for grazing flourishes in the rainy winter months but tends to be desiccated by late spring and summer. The majority of farms in Israel house cows indoors all year round, and the pooling of milk by the centralized dairy production may also attenuate variation.
In comparison to cow's milk, goat's milk was much richer in iodine, with an average content of 63 μg/100 g. In contrast, soy beverages (soy milk) had almost no iodine (0–1 μg/100 g). The iodine content of all milk was found to be generally higher than that of cultured or processed dairy products.
Population iodine intake from milk, dairy products, and dairy-based foods
Using the average concentration results of all types of cow's and goat's milk and based on the recommendations of the relevant authorities in Europe and the United States, the proportion of the recommended daily iodine intake provided by a cup of cow's or goat's milk was calculated for children, adolescents, adults, and pregnant or lactating women (Table 2). One cup of cow's milk provides nearly 66% of the RDA of iodine for children, 33% for adults, and 20–25% of the RDA for pregnant and lactating women. A single cup of goat's milk provides almost twice the RDA for children, the full requirement for adults, and approximately half the requirement for pregnant and lactating women.
RDA and UL according to the U.S. National Academy of Sciences Institute of Medicine Dietary Reference Intakes (34).
cup = 240 mL.
RDA, recommended daily allowance; UL, upper limit.
Milk and dairy products were consumed by 80% of MABAT survey participants (n = 2733), and only 6% of all MABAT survey participants reported use of any iodine-containing supplements in the past 30 days (37.5–220 μg per tablet).
Iodine intake from milk, dairy products, and dairy-based foods in the overall adult population was positively skewed (M = 33.7 ± 35.6 μg/day; median 23.1 μg/day; range 0–337 μg/day; interquartile range [IQR] 6.6–50.6 μg/day). This mean represents 22% of the RDA for nonpregnant adults (150 μg/day) and 35% of the estimated average requirement (EAR; 95 μg/day) (34). Only 6% of the population achieved the EAR, and 1.3% achieved the RDA from the consumption of milk, dairy products, and dairy-based foods alone. Neither the U.S. Institute of Medicine upper limit of 1100 μg/day nor the more conservative European Commission upper limit of 600 μg/day for adult iodine intake was exceeded from these foods alone (Fig. 1) (36,37). When the 17 frequently consumed dairy-based foods were excluded from the analysis, the mean iodine intake from milk and dairy products alone was 31.9 μg/day. In other words, including diary-based foods in the calculation only marginally improved the estimated population mean intake by 1.8 μg/day.

Distribution of estimated iodine intake from milk, dairy products, and dairy-based foods (μg/day) among Israeli adults (Israel National Health and Nutrition Survey [MABAT] 1999–2001, N = 3246, ages 25–64 years). Solid line, Weibull fit line; dashed line, recommended daily allowance (RDA) reference line (150 μg/day); dotted line, estimated average requirement (EAR) reference line (95 μg/day).
Table 3 shows the average population iodine intake from milk, dairy products, and dairy-based foods by category of dairy product. On average, drinking cow's milk provides 62.5% of this intake. Yogurt, cultured cow's milk products, and soft white cheeses provide 31.3% of the intake iodine; 6.2% comes from yellow cheese and ice cream, and a negligible fraction from goat's milk.
Estimated by average estimated daily intake according to Israel National Health and Nutrition Survey 1999–2001 (MABAT survey, N = 3246, men and women aged 25–64) (30).
The distribution of iodine intakes from milk, dairy products, and dairy-based foods differed between the different sectors of Israeli society (Fig. 2). The median intake among Israeli Arabs (16.5 μg/day; IQR 0–39.6 μg/day) was significantly lower compared to the medians of all other Jewish groups (Secular Jewish 27.4 μg/day, IQR 10.6–54.0 μg/day; Religious Jewish 23.8 μg/day, IQR 9.2–53.7 μg/day; and Ultra-Orthodox Jewish 33.1 μg/day, IQR 5.4–57.4 μg/day; Wilcoxon pair-wise comparisons, p < 0.0001). The median intake of Ultra-Orthodox Jews was significantly higher than that of either Arabs or Religious Jews (p < 0.0001 and p = 0.003, respectively) and marginally significantly different from that of Secular Jews (p = 0.059).
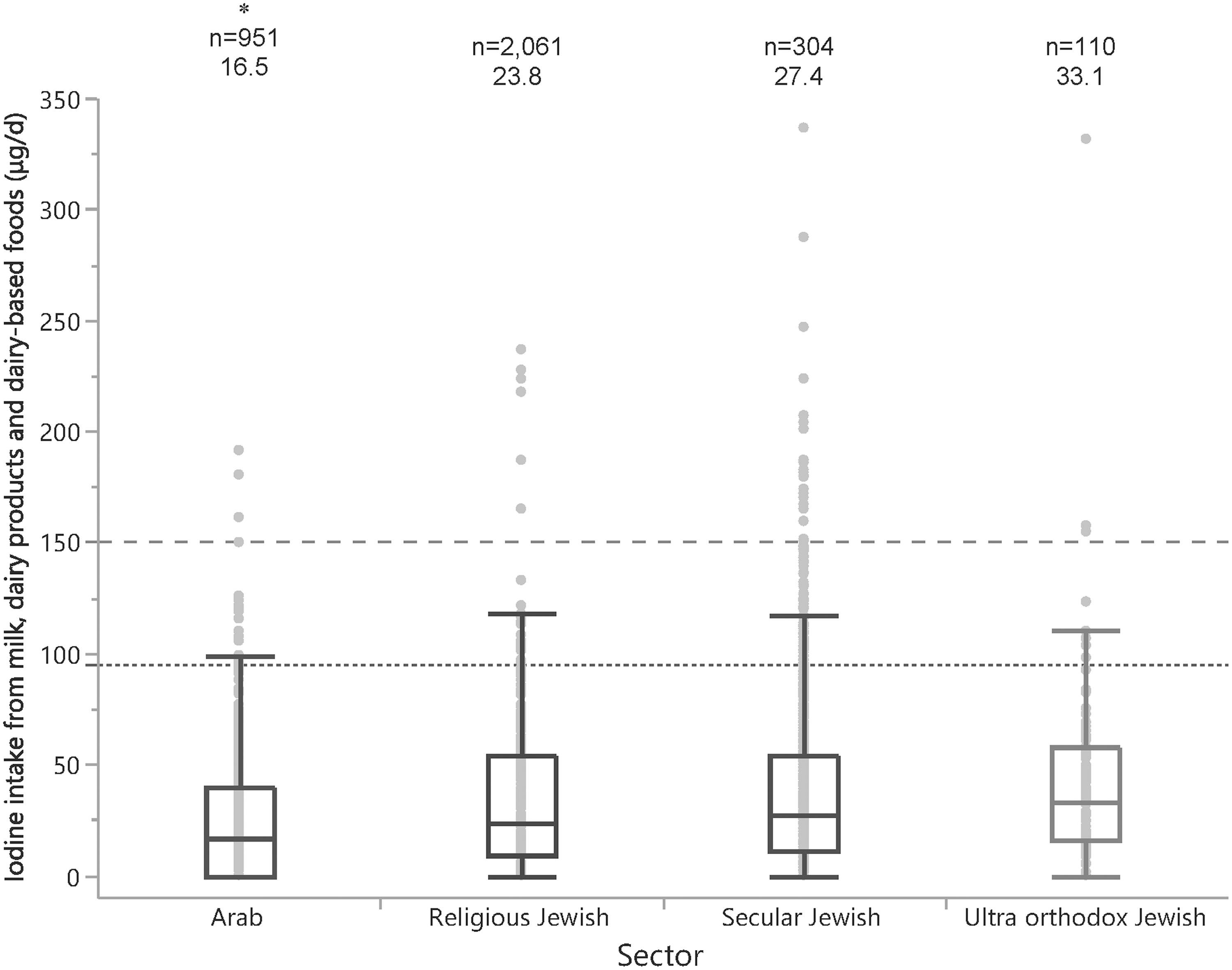
Estimated iodine intake from milk, dairy products, and dairy-based foods (μg/day) by sector among Israeli adults (Israel National Health and Nutrition Survey [MABAT] 1999–2001, ages 25–65 years). Numbers above each box plot denotes group size (number) and median value. *Significantly lower than all other groups (each pair comparison, Wilcoxon method, p < 0.0001). Dashed line, RDA reference line (150 μg/day); dotted line, EAR reference line (95 μg/day).
Iodine intake distributions also differed significantly by sex, childbearing status, and poverty. The median iodine intake from milk, dairy products, and dairy-based foods was 27.5 μg/day for women versus 19.8 μg/day for men, as shown in Figure 3 (Kruskal–Wallis test, p < 0.001). Pregnant women had a marginally significantly higher intake from milk and dairy than nonpregnant women of childbearing age (M = 43.4, median 37.1, range 0–186 vs. M = 23.1, median 33.7, range 0–79 μg/day respectively; p = 0.054). Intakes of pregnant women were the highest reported intakes in this study, as displayed in Figure 3. Consistent with this finding, the frequency of self-reported use of iodine-containing supplements in the past 30 days (37.5–220 μg/tablet) was significantly higher among pregnant women than nonpregnant women of childbearing age (12.8% vs 7.6%, respectively; Fisher's exact test, p < 0.005).
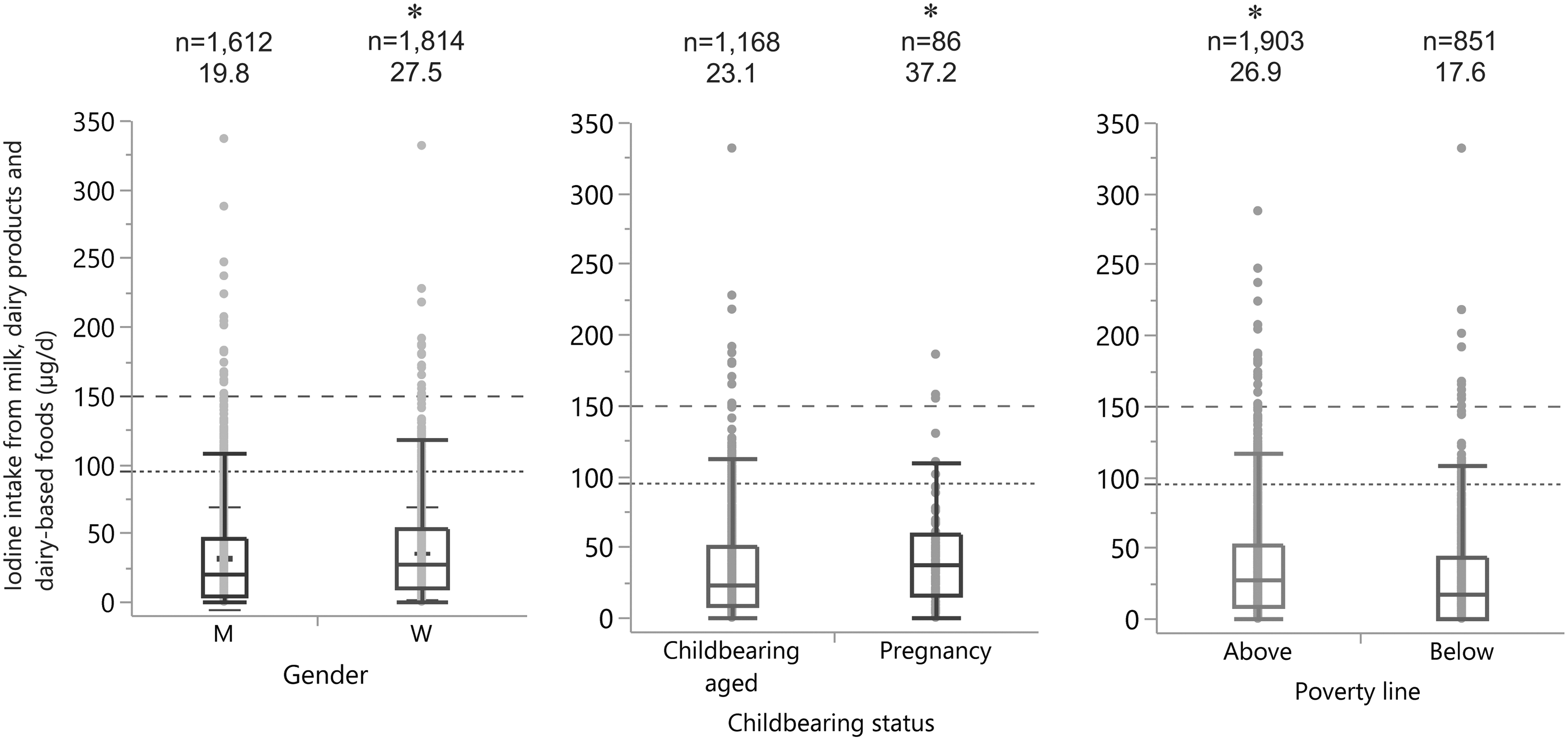
Estimated iodine intake from milk, dairy products, and dairy-based foods (μg/day) by sex, childbearing status, and poverty line among Israeli adults (Israel National Health and Nutrition Survey (MABAT) 1999–2001, ages 25–64 years). Numbers above each box plot denotes group size (number) and median value. *Significantly higher than alternate category (Kruskal–Wallis, p < 0.0001). Numbers above each box plot are group size (number) and median values. Dashed line, RDA reference line (150 μg/day); dotted line, EAR reference line (95 μg/day); M, men; W, women.
Interestingly, iodine intake among those below the poverty line was significantly lower than of those above this line (Fig. 3). Arabs and Ultra-Orthodox Jews were disproportionately overrepresented among the poor. Based on self-reported data, 60.6% of Arabs and 67.7% of Ultra-Orthodox Jews were below the poverty line (chi-square test, Fisher's exact test, p < 0.0001), despite the fact that they only make up approximately 20% and 10% of the general population, respectively. However, self-reported income was unavailable (not reported) for a total of 19.6% of the cohort. The rate of non-reporting differed by sector, with 7.5% unavailable income data for Arabs, 10.3% for Secular Jews, 1.5% for Religious Jews, and 0.3% for Ultra-orthodox Jews.
Discussion
This is the first study to determine iodine content in Israeli milk and dairy products. The study delineates the contribution of milk, dairy products, and dairy-based foods to iodine intake in the Israeli population at large, and reveals significant differences in intake among different sectors of society. Moreover, the high variability in milk iodine content from different countries underscores the importance of maintaining accurate and current local data in every country.
The iodine content in Israeli cow's milk was found to be high enough that drinking two cups per day for children, three for adults, and four for pregnant women would achieve the RDA. For goat's milk, the values are so high that two cups per day for children would exceed the upper limit (Table 2). These values are somewhat higher than those reported for other countries where similar data were obtained by the same technique (ICP-MS). Both Norwegian cow's milk (all types) and cow's yogurt are reported to have lower iodine concentrations than comparable Israeli products (15 vs. 22 μg/100 g and 8 vs. 15 μg/100 g, respectively) (38). Data from New Zealand show lower iodine content in comparison to Israel for standard milk (9 vs. 22 μg/100 g), yogurt (9 vs. 15 μg/100 g), and white cottage cheese (10 vs.13 μg/100 g) (39). Milk from Hong Kong is similarly lower in iodine than Israeli milk (9 vs. 22 μg/100 g) (40. However, slightly lower iodine was found in milk from Israel than in values reported for the United Kingdom (22 vs. 25–41 μg/100 g) (41 –43). Interestingly, the iodine content for the 3% fat milk in the present study was the same as that reported for Israeli milk in the late 1980s (26 μg/100 g) (40).
Substantial variability in intake is shown to reflect high variability in consumption of milk, dairy products, and dairy-based foods in Israel's population at large. Despite a mean dairy intake of 161 g/day overall, the skewed distribution of iodine intake on the left of the distribution shows that a large proportion of the population consumes little milk and dairy (Table 3), while a long tail of higher consumption to the right of the distribution indicates that dairy provides a substantial proportion of the recommended intake for a minority of individuals (Fig. 1). While pregnant women had a relatively higher mean intake than the overall population (43.4 vs. 33.7 μg/day, respectively), these intakes represent only 20% and 22% of the RDA for pregnant and lactating women, respectively. Despite this apparent shortfall in iodine intake from milk, dairy products, and dairy-based foods, adequate iodine intake may be ensured for pregnant women by the use of both an iodine-containing supplement (150 μg/day), as recommended for pregnant women, and iodized salt elsewhere (13,44).
On average, survey participants falling below the poverty line also have a relatively low iodine intake. This is likely because the consumption of milk and dairy, as well as meat and fresh produce, is directly proportional to socioeconomic status (45). Given that substantial proportions among Israel's poor are Arabs and Ultra-Orthodox Jews, low iodine intake from dairy would have been predicted in both population groups. The unexpected finding of the highest iodine intake from dairy being among Ultra-Orthodox Jews is in contrast to the substantial relative poverty of this segment of the population. This suggests that dietary patterns in other vulnerable sectors of society might be improved through public-health and policy measures directed toward encouraging better dietary choices.
The question of how socioeconomic status relates to iodine intake warrants further attention. Socioeconomic status has been inconsistently associated with iodine intake in the literature, depending on social context and salt iodization policy (46 –48). The data suggest that it may be a significant factor in countries such as Israel with large socioeconomic gaps (high GINI indexes) and without salt iodization (47). Because insufficient dietary iodine intake in utero is associated with poor intellectual achievement (5,6), insufficiency among lower socioeconomic strata could hinder upward mobility and compound societal gaps. The detected association between iodine intake and socioeconomic status must be addressed by nutrition policy in Israel and possibly in other countries that do not iodize salt and where dietary patterns determine intake.
While this study shows that in 2016, milk and dairy products were potentially good sources of iodine for the Israeli diet, the dietary patterns captured by the MABAT survey suggest that consumption patterns of milk, dairy, and dairy-based foods among Israeli adults do not ensure adequate iodine intake. Studies using similar sample sizes and dietary estimation methods in other developed countries have revealed higher total iodine intake from dairy products. For example, the mean intakes of iodine from milk and dairy products alone (without dairy-based foods) among 12,153 Australians (whose diet was evaluated by a 24-hour recall) and 2672 Norwegian adults (whose diet was evaluated by food frequency questionnaires) were higher than found among Israeli adults in this study (41 μg/day and 88 μg/day vs. 32 μg/day, respectively) (38,45,49). This suggests that increased consumption of dairy products could boost iodine intake among Israeli adults.
The exceedingly low iodine in Israeli soy-based milk substitutes is an important finding. Several recent studies conducted elsewhere have identified widely divergent iodine values in soy-based beverages (50 –52), and case reports suggest that their consumption may be associated with the risk of hypothyroidism in users of low-iodine substitutes or thyrotoxicosis in users of high-iodine substitutes (53,54). The iodine content of milk substitutes must be considered in providing dietary guidance for sizable populations of vegans or allergic individuals who avoid milk and dairy in Israel and elsewhere. Further research is needed to understand how these products affect iodine status among their users, and to raise awareness of iodine in addition to calcium as a consideration for the manufacture and use of milk substitutes.
This study has several limitations. The 24-hour recall questionnaire to estimate dietary intake is an indirect tool that captures short-term iodine intake and may not reflect the intrapersonal day-to-day variation in dietary iodine intake (55). However, the MABAT survey sample size is large enough to average out the daily variation in iodine intake across the overall population. While the products included in this study represent 89% of the milk and dairy consumption reported by the survey population, the remaining 11% was consumed in small amounts (8–10 g/day on average). Based on the milk iodine content, it is estimated that these foods provide only 1–2 μg of additional iodine per day, so the estimated iodine intake from dairy products may be slightly lower (3–6%) than the true intake. Most importantly, regular monitoring is essential so that policy is responsive to current data regarding the sources of iodine and its intake in the population. Data from the MABAT survey (1999–2001) (30) were the most current available, but the caveat that habitual dairy intake across the population may have changed since 2001 is underscored. It will be important to reevaluate the estimates when more current data become available, not only for adults but also for children and older people, and with specific reference to age-dependent intake patterns, pregnant women, the prevalence of those who avoid dairy such as vegans, and other vulnerable segments of the population.
Further work is also needed to assess other potential sources of iodine in the Israeli diet, as these are uncertain. Only 3% of salt produced in Israel is iodized, and salt imports are negligible (10). Data on consumption are unavailable. However, the household coverage is almost certainly less than the 3% rate of local iodized salt production (10). On average, the population consumes less than a portion a day of fish and seafood (30), which can be estimated to contribute less than half the amount of iodine provided by milk and dairy to total iodine intake. Other potential sources such as eggs and meat are unlikely to make up the difference. Moreover, the extensive use of desalinated water in Israel has diminished the amount of iodine that is directly available (12), and also indirectly available through animal feed and crop irrigation in iodine poor soil (56). The recent national iodine survey found a median urinary iodine concentration of 83 μg/L in school-age children and 61 μg/L in pregnant women. In other words, present habitual dietary patterns do not ensure the iodine sufficiency of Israel's population (13).
In conclusion, Israeli milk and dairy products are iodine rich. The calculated iodine intake from milk, dairy products, and dairy-containing foods, based on a nationally representative population sample, indicates that increased consumption of milk and dairy products could contribute significantly to adequate iodine intake in the Israeli population. Nevertheless, given the increased use of iodine-depleted desalinated water and the absence of mandatory salt iodization in Israel, it is unlikely that the majority of Israelis will achieve iodine sufficiency. These findings support dietary recommendations regarding iodine intake from milk and dairy products and the regular review of public-health policy for universal salt iodization and/or iodine supplementation in high-risk groups. Both are essential to ensure iodine sufficiency for a society that confronts sectorial socioeconomic barriers to adequate diet and must regularly monitor changes in the water and food supply. Only by regularly monitoring food iodine content and intake can public-health authorities respond to changes in access, availability, and quality of the food supply not only in Israel but elsewhere around the world.
Footnotes
Acknowledgments
We are indebted to Dr. Lia Supino from Maccabi Healthcare Services for assistance with data handling. This study was supported by grant no. 3-0000-11150 from the Israeli Ministry of Health Chief Scientist Office, which administers the scientific grant review process and allocation of funds provided in trust by the Israeli Dairy Board. Partial support was also provided by Israeli Ministry of Health Chief Scientist Office grant no. 3-00000-12821 and by the European Union's Horizon 2020 research and innovation programme under “EUThyroid” (grant no. 634453).
Author Disclosure Statement
The funding parties had no involvement with the study. No competing financial interests exist.
References
 ). Israel Cattle Breeder's Association Newsletter [Hebrew].
). Israel Cattle Breeder's Association Newsletter [Hebrew].  54-58:(4)255;1995. Available at:
54-58:(4)255;1995. Available at: 
 )
) 
 . Available at:
. Available at:  ).
).