
Abstract
Background:
In older patients, thyroid nodules are frequently detected and referred for evaluation, though usually prove to be benign disease or low-risk cancer. Therefore, management should be guided not solely by malignancy risk, but also by the relative risks of any intervention. Unfortunately, few such data are available for patients ≥70 years old.
Methods:
All consecutive patients ≥70 years old assessed by ultrasound (US) and fine-needle aspiration (FNA) between 1995 and 2015 were analyzed. Clinical, US, and histologic data, including patient comorbidities and outcomes, were obtained. Imaging and cytology results from initial evaluation were reviewed to detect significant-risk thyroid cancer (SRTC), which was defined as anaplastic, medullary, or poorly differentiated carcinoma, or the presence of distant metastases. Overall survival analyses were then performed to assist with risk-to-benefit assessment.
Results:
A total of 1129 patients ≥70 years old with 2527 nodules ≥1 cm were evaluated. FNA was safe in all, and cytology proved benign in 67.3% of patients. However, FNA led to surgery in 208 patients, of whom 93 (44.7%) had benign histopathology. Among all patients who underwent FNA, only 17 (1.5%) SRTC were identified, all of which were preoperatively identifiable by imaging and/or cytology. These SRTC were responsible for all (n = 10; 0.9%) thyroid cancer deaths. Among all other patients (n = 1112), 160 deaths (14.4%) were confirmed during a median follow-up of four years. None of these were thyroid cancer related. Survival analysis for these 1112 patients demonstrated that a separate non-thyroidal malignancy or coronary artery disease at the time of nodule evaluation was associated with increased mortality compared to those without these diagnoses (hazard ratio = 2.32 [confidence interval 1.66–3.26]; p < 0.01), confirming these are important variables to identify prior to thyroid nodule evaluation.
Conclusions:
For patients ≥70 years old, US and FNA are safe and prove helpful in identifying SRTC and benign cytology. However, the surgical management of patients ≥70 years old presenting without high-risk findings should be tempered, especially when comorbid illness is identified.
Introduction
T
Over recent decades, the incidence of thyroid nodules and cancer has dramatically increased (7,8), largely attributed to greater detection of incidental lesions (9). Not surprisingly, the majority of these thyroid cancers are small, low-risk carcinomas (8). The observation that thyroid cancer mortality has remained stable during this time suggests that the diagnosis of many thyroid cancers was likely irrelevant, as they would not have become clinically evident (10). Furthermore, surgical interventions are often a source of morbidity that must be balanced with their potential benefits.
Advancing patient age is an important consideration in the evaluation and management of nodular disease. In younger patients, intervention is often justified by the hypothetical avoidance of future cancer progression or metastatic disease, especially when the risk of surgery is low. However, older patients have fewer life-years ahead of them, and frequently have comorbid diseases that increase surgical risks. Current guidelines broadly suggest a more conservative approach to thyroid nodule evaluation and thyroid cancer treatment in older patients (2,11,12), but few data are available to guide providers with the complex assessment of specific risk versus benefit decisions in the older population. Thus, the purpose of this study was to address this gap and facilitate a more informed and personalized discussion between patients ≥70 years old and their healthcare providers.
Since 1995, the Brigham and Women's Hospital Thyroid Nodule Clinic has been the major referral center for all patients requiring nodule evaluation in the healthcare population. Per guideline recommendations relevant to the time, most patients with nodules ≥1 cm in diameter were recommended for ultrasound-guided fine-needle aspiration (UG-FNA). Using these prospectively collected data, an analysis was performed of all patients ≥70 years old seeking care for a thyroid nodule. In doing so, these data provide the first available insight into the quantitative benefits, risks, and potential harm of thyroid nodule evaluation in older individuals.
Methods
The records were reviewed from a prospectively collected database of consecutive patients cared for at the Brigham and Women's Hospital Thyroid Nodule Clinic between 1995 and 2015, identifying euthyroid patients ≥70 years old who underwent UG-FNA of a thyroid nodule ≥1 cm in largest dimension. All demographic, clinical, sonographic, cytologic, and pathologic data were obtained from the medical record. Institutional Review Board approval was granted for this study.
Clinical care of all patients included neck US evaluating the thyroid and cervical lymph nodes performed by a radiologist with expertise in thyroid sonography, using a 10–18 MHz transducer. Nodule location, solid or cystic parenchyma (<25%, 25–50%, 50–75%, or >75% cystic), and size in three dimensions was measured. UG-FNA biopsy was performed by a thyroidologist under ultrasound guidance, using a 25–27 gauge needle and typically employing at least three aspirates per nodule. All aspirates were processed using a liquid-based cytology preparation (Hologic Corp., Marlborough, MA), and aspiration material was evaluated by a pathologist experienced in thyroid cytology. Although the period of study partially predates The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC), cytologic classification employed the same criteria and terminology later adopted by the TBSRTC (1,13). Thyroid FNA cytology was reported as: non-diagnostic, negative for malignant cells (benign), atypia of undetermined significance (AUS), suspicious for follicular or Hürthle cell neoplasm (SFN), suspicious for malignancy (SUSP), or malignant. For patients with more than one nodule evaluated by UG-FNA, the primary cytology was defined as the cytologic result that carried the highest risk of malignancy. In cases where thyroid surgery was performed, the final diagnosis was based upon histopathology. Cancer stage was categorized using the American Joint Committee on Cancer's tumor-node-metastasis (TNM) system applicable at that time.
Significant-risk thyroid cancers (SRTC) were histopathologically defined as: anaplastic thyroid carcinoma (ATC), poorly differentiated thyroid carcinoma (PDTC), or medullary thyroid carcinoma (MTC), or follicular thyroid carcinoma (FTC), Hürthle cell carcinoma (HCC), or papillary thyroid carcinoma (PTC) with distant metastatic disease. Preoperative evidence suggestive of SRTC was defined as: cytology positive for a SRTC histology type (i.e., ATC or MTC) and/or review of imaging reports indicating gross invasion, lymph node metastases, or distant metastases present preoperatively.
Additional medical conditions present at the time of thyroid nodule assessment were reviewed. The presence of coronary artery disease (CAD) was defined as a preexisting diagnosis of CAD in the medical record, or history of myocardial infarction, coronary artery stenting, or bypass surgery. The presence of a separate non-thyroidal malignancy was determined by diagnosis in the medical record. Serious complications from UG-FNA were defined as clinical injury to the carotid artery, jugular vein, esophagus, or trachea, as well as pain or hematoma requiring urgent reevaluation of the patient. Serious complications of thyroidectomy were defined as re-operation for hematoma, bilateral recurrent laryngeal nerve (RLN) injury, persistent (>6 months) unilateral RLN injury, postoperative hypocalcemia requiring reevaluation, or persistent (>6 months) hypoparathyroidism. The date of last clinical follow-up or the date and cause of death were extracted from the electronic medical record to assess the overall survival (OS) of patients. The presence and type of medical comorbidities and the number of medications taken at the time of initial nodule evaluation were recorded.
Statistical analysis
Summary statistics are provided as mean ± standard deviation for normally distributed continuous variables, median with range for non-normal continuous variables, or number and percentage for categorical variables. For comparisons of continuous and categorical variables, the two-sample Student's t-test and Pearson's chi-square test were used, respectively. OS was estimated using the Kaplan–Meier method, and comparison of survival curves was made using a large-sample chi-square test (log-rank test). OS in patients with CAD or non-thyroidal cancer was compared to patients without these comorbidities, excluding SRTC patients, and these survival curves were subsequently further stratified by specific comorbidity. Risk of all-cause mortality was assessed using Cox proportional hazard regression analysis, including baseline predictors such as age, sex, and comorbidity with hazard ratio (HR) and confidence intervals (CIs) presented. All analyses were performed with SPSS for Windows v16.0 (SPSS, Inc., Chicago, IL) or SAS v9.3 (SAS Institute, Cary, NC). Statistical significance was defined as a two-tailed p-value of <0.05 for all analyses. Figures were produced using GraphPad Prism (Graphpad Software, Inc., La Jolla, CA) and Adobe Photoshop (Adobe Systems, Inc., San Jose, CA).
Results
Between 1995 and 2015, 1129 consecutive patients ≥70 years old were evaluated by UG-FNA for a thyroid nodule ≥1 cm in greatest dimension. As shown in Table 1, 872 (77.2%) were women, and the median age was 75 years (range 70–95 years). The median nodule size was 1.7 cm (range 1.0–12.5 cm), and 656 patients (58.1%) had two or more nodules each ≥1 cm (multinodular). Thyroid nodule evaluation led to a diagnosis of malignancy in 132/1129 (11.7%) patients.
Includes 208 patients that underwent thyroid surgery and 17 patients with cytology positive for malignancy that did not undergo surgery. See text for details.
SD, standard deviation; CAD, coronary artery disease; MNG, multinodular goiter.
The primary cytologic diagnoses are presented in Table 2 and show that of the 1129 patients, cytology was non-diagnostic in 72 (6.4%), benign in 760 (67.3%), AUS in 95 (8.4%), SFN in 90 (8.0%), SUSP in 62 (5.5%), and malignant in 50 (4.4%). The percentage of patients undergoing surgery and the rate of malignancy in each cytologic category are shown in Table 2. While surgery was typically recommended for SUSP or malignant cytology, thyroid surgery was not performed in all patients. For 14 patients with suspicious cytology, surgery was deferred because of another active malignancy, serious medical conditions, or advanced age. In patients with malignant cytology, 10 with advanced thyroid cancer did not undergo surgery because of the extent of their disease, and seven patients had intrathyroidal metastases from a non-thyroidal malignancy for which surgical resection was not indicated. There were 30 patients with benign cytology who underwent thyroid surgery. The indications were hyperparathyroidism (n = 5), compressive symptoms (n = 10), nodule >4 cm without symptoms (n = 11), and increasing nodule size (n = 3). One patient underwent nodule removal during resection of a squamous cell cancer.
Percentage of malignancy = malignancies diagnosed divided by total number in each cytologic category.
Includes 17 patients with malignancy positive by cytology only. These results were positive for intrathyroidal metastasis of a non-thyroidal malignancy (n = 7), anaplastic thyroid cancer (n = 4), medullary thyroid cancer (n = 1), and papillary thyroid cancer (n = 5).
Of these 1129 patients ≥70 years old undergoing thyroid FNA, 208 (18.4%) underwent thyroid surgery. Of these, histology was benign in 93 (44.7%) and malignant in 115 (55.3%). Including the additional 17 patients with biopsy-proven thyroid cancer who did not have surgery because of disease extent or other significant health limitations, there were 104 (78.8%) PTC, five (3.8%) FTC, two (1.5%) HCC, one (0.8%) MTC, four (3.0%) PDTC, and nine (6.8%) ATC detected in this cohort (Table 1). Intrathyroidal metastasis from a non-thyroidal cancer was diagnosed by cytology in seven patients (0.6% of all patients).
Seventeen (13.6%) of the 125 thyroid cancers in this older cohort were defined as having SRTC based on histology of ATC, MTC, or PDTC or other thyroid cancer histology and the presence of distant metastases. In patients with SRTC, the mean age was 79.3 ± 5.5 years, and a high proportion (n = 7; 41.2%) were male. Importantly, in all 17 SRTC patients, preoperative assessment suggested SRTC (Table 3). Thyroid cancer mortality was confirmed in 10/17 (58.8%) SRTC patients during a median follow-up of only five months (interquartile range 2–28.5 months).
Definition of significant-risk thyroid cancer (SRTC) = ATC, PDTC, or MTC, or FTC, HCC, or PTC with distant metastatic disease.
Criteria for preoperative evaluation suggestive of SRTC = cytologic result showing a SRTC-defining histology (e.g., ATC, MTC) and/or imaging results showing gross tumor invasion, lymph node metastases, or distant metastases.
At time of FNA.
By sonographic assessment.
On preoperative imaging evaluation.
Thyroidectomy not performed.
From lymph node biopsy.
From lung biopsy.
US, ultrasound; NA, not applicable; HE, hypoechoic; FDG, flurodeoxyglucose; MC, microcalcifications; ATC, anaplastic thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; MTC, medullary thyroid carcinoma; HCC, Hürthle cell carcinoma; PTC, papillary thyroid carcinoma; SUSP, suspicious for malignancy (Bethesda V).
For the remaining 108 thyroid cancer patients, histology demonstrated that 87 lesions (80.6%) were completely intrathyroidal, 12 (11.1%) had minimal microscopic extrathyroidal extension, six (5.6%) had minimal microscopic extrathyroidal extension combined with lymph node metastases, two (1.9%) had local lymph node metastases, and one (0.9%) had gross extrathyroidal extension with local lymph node metastasis. Lymph node metastases were classified as central neck (N1a) in five patients and lateral neck (N1b) in three patients. In contrast to patients with SRTC, no deaths related to thyroid cancer were identified in these 108 patients over the duration of follow-up of 72 months (range 1–228 months).
The potential risks of thyroid nodule evaluation in the entire cohort were evaluated by quantification of procedural complications. Only one patient was identified with a complication (symptomatic hematoma) after UG-FNA, but ultimately required no additional treatment. Of 208 patients treated surgically, three (1%) significant complications were identified, including one case of permanent hypoparathyroidism, one case of transient hypoparathyroidism requiring emergency evaluation for hypocalcemia, and one case of unilateral RLN injury.
Next, the overall future survival (OS) in this cohort was investigated, starting at the time of initial thyroid nodule evaluation. Of the 1112 patients ≥70 years old without SRTC, no deaths related to thyroid cancer were identified during a median follow-up of 48 months (range 1–240 months), though 160 (14.4%) patients died over this period from causes unrelated to thyroid cancer. Analysis showed that separate non-thyroidal malignancy or CAD noted at the time of thyroid nodule evaluation was strongly associated with future mortality during follow-up, confirming such findings are important to identify during patient evaluation. The OS of the 508 patients identified with CAD or a non-thyroidal malignancy were compared to the 604 patients without these comorbidities. Patients with CAD or non-thyroidal malignancy were older (76.3 ± 5.0 years vs. 75.2 ± 4.3 years; p < 0.01) and more likely to be male (141/251 [56.2%] vs. 367/861 [42.6%]; p < 0.01). The product limit survival estimates for Kaplan–Meier curve analysis of OS (Fig. 1A) showed significantly shorter OS in the patients with these comorbidities (log-rank test p < 0.0001). In a multivariate Cox proportional hazard regression (Table 4), the presence of CAD or non-thyroidal malignancy was independently associated with worse OS (HR = 2.32 [CI 1.66–3.26]; p < 0.01). When patients were stratified into those with separate malignancy, CAD, both conditions, or those without either of these comorbidities, Kaplan–Meier curve analysis showed significant differences is OS (log-rank test p < 0.0001; Fig. 1B) and multivariate Cox proportional hazard regression analysis showed increasing hazard of death after adjustment for age and sex (Table 5). Together, these data demonstrate the importance of identifying separate non-thyroidal malignancy or CAD at the time of initial thyroid nodule evaluation.
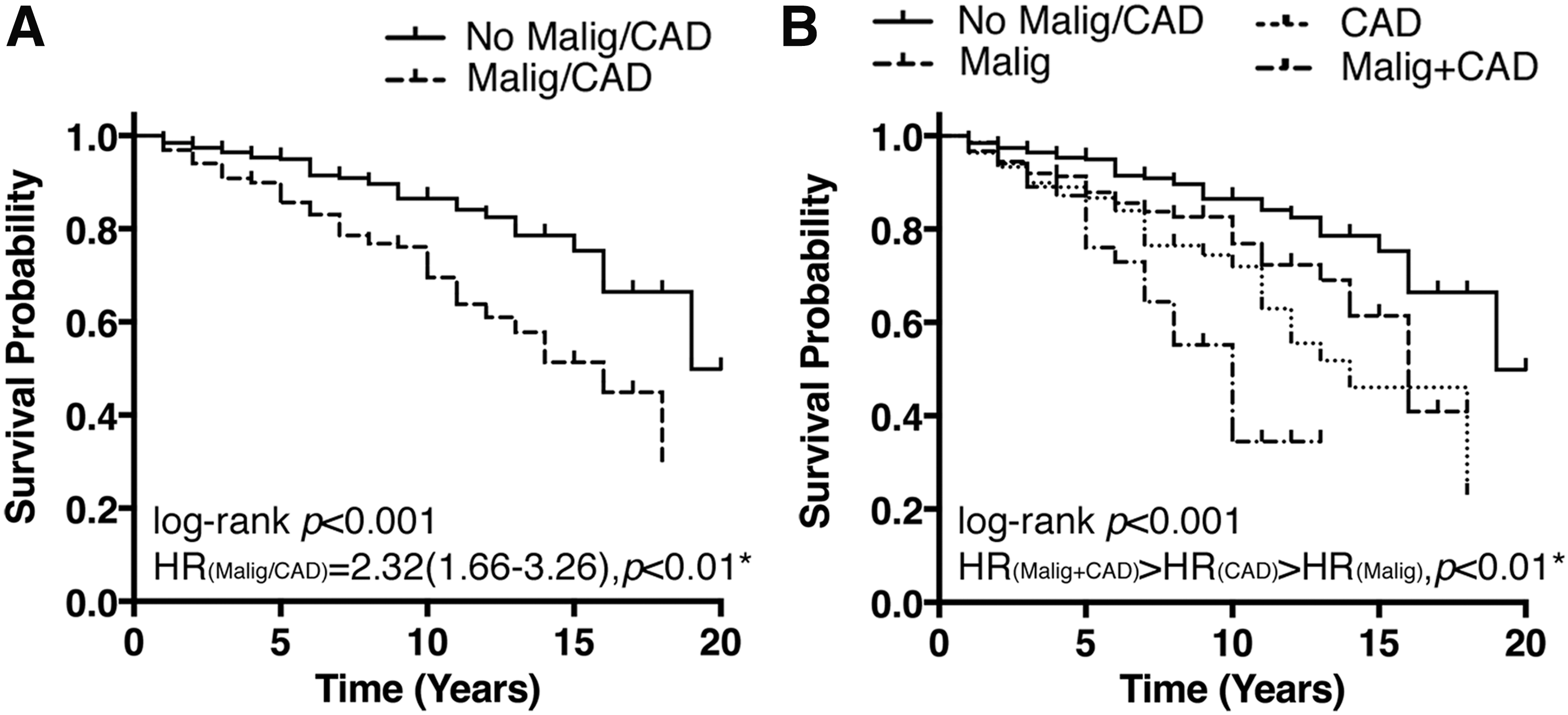
Impact of separate non-thyroidal malignancy or coronary artery disease (CAD) at the time of thyroid nodule evaluation on overall survival (OS) in patients ≥70 years old. Kaplan–Meier curves for OS for the entire patient cohort, excluding those with significant risk thyroid cancer. (
HR, hazard ratio; CI, confidence interval.
Summarizing the potential benefits and risks associated with thyroid nodule assessment in this cohort ≥70 years old (Table 6), the following were confirmed: 1 out of every 66 patients ≥70 years old was found to harbor a SRTC for which intervention is necessary. However, 1 out of every 13 patients ≥70 years old underwent unnecessary surgery for benign disease. A serious surgical complication occurred in 1 out of every 69 patients ≥70 years old undergoing thyroidectomy. Perhaps most importantly, one out of every seven patients ≥70 years old died during a median follow-up of 48 months (range 1–240 months), and almost all deaths (94%) were attributable to non-thyroidal causes.
Defined as ATC, PDTC, MTC, and FTC, HCC, or PTC with distant metastasis.
Including only thyroidectomies performed for asymptomatic nodular disease.
Discussion
The identification of thyroid nodules and diagnosis of thyroid cancer has been dramatically increasing, especially in older adults. However, the optimal management of these illnesses in this population remains unclear as physicians and patients try to balance the risks and potential benefits of intervention. The data from this prospectively collected, consecutive cohort of 1129 patients ≥70 years old seeking diagnostic evaluation for thyroid nodules provide the first large-scale guidance to assist with this complex decision.
These data confirm the utility of sonographic neck evaluation, and UG-FNA, in patients ≥70 years old when thyroid nodules ≥1 cm are identified. Using this strategy, benign cytology will be identified in approximately two-thirds of patients, which is a highly accurate finding and allows conservative management, alleviating concern among patients and providers. Equally important, initial evaluation in this older cohort identified a SRTC in 1/66 patients. Older individuals with thyroid nodules may have a lower risk of malignancy than younger patients. In a large cohort of consecutive patients undergoing thyroid nodule FNA, malignancy was confirmed in 17.1–22.9% of thyroid nodules in patients aged 20–49 years compared to 12.6% in patients ≥70 years of age (14). However, older patients are at higher risk for aggressive thyroid cancers and thyroid cancer mortality (15). Recently, Lim et al. (16) showed an increased thyroid cancer mortality rate in 77,276 thyroid cancer patients diagnosed during 1974–2013, and a positive annual percent change in incidence-based mortality rate was statistically significant for patients diagnosed after 79 years of age. The present data do show that mortality related to thyroid cancer is a significant concern in this population, confirming the importance of identifying aggressive thyroid cancers, which accounted for all thyroid cancer mortalities.
Prompt recognition of potentially fatal thyroid cancer is necessary to provide optimal management. While survival for these high-risk cancers remains poor (17), palliative management as well as novel emerging treatments (18,19) make timely diagnosis important. It was found that nearly all the aggressive and ultimately fatal thyroid cancers were identifiable preoperatively based on imaging and cytologic assessment, providing the opportunity for urgent intervention in those for whom it is most necessary. The presence of SRTC was suggested by imaging in most SRTC patients, but FNA is likely still necessary to identify specific histologic types (e.g., ATC or MTC) that would predict aggressive tumor behavior and lead to more urgent management.
However, for the majority of patients without SRTC, these data suggest that the traditional approach involving diagnostic or therapeutic surgery must be carefully considered or reduced among patients ≥70 years old. In support of this, the present data confirm that 1/13 who underwent surgery had benign disease. Many of these patients had indeterminate cytology, for which diagnostic thyroidectomy was considered necessary to detect and potentially treat thyroid cancer. Six additional patients had thyroidectomy for a thyroid nodule with repeatedly non-diagnostic cytology, though none of these were revealed to have thyroid cancer. Importantly, there were also no thyroid cancer deaths over a median of 48 months (range 1–240 months) observed in any patients who did not harbor a SRTC.
Given the indolent course of most thyroid carcinomas, it is important to consider patient longevity when initiating the evaluation of a newly detected thyroid nodule. Over a median duration of 48 months (range 1–240 months), it was confirmed that 13.5% of this older cohort died during follow-up. In particular, the identification of patients with a separate (non-thyroidal) malignancy and/or CAD proved highly important, as individuals with such comorbidities had a significantly higher risk of all-cause mortality during follow-up compared to those without these diagnoses. These findings suggest that thyroid nodule evaluation in such patients may prove of little long-term benefit (and can be avoided), so long as the initial ultrasound demonstrates no concerning findings.
In summary, these data depict the risks and benefits of thyroid nodule evaluation in patients aged ≥70 years. While one cannot exclude a modest possible benefit to treating all biopsy-confirmed thyroid cancer, the data are consistent with the known indolent course demonstrated by most well-differentiated thyroid cancers. In support, the American Thyroid Association guidelines note that a conservative strategy may be reasonable in such older individuals (2) because the majority of older patients with nodular disease will have benign or relatively indolent thyroid cancer (14,20), and prior studies support a conservative approach in low-risk papillary microcarcinomas (21,22). Though the surgical complications were low in this cohort, as the patients were treated by high-volume thyroid surgeons, the risks of intervention are likely greater in lower-volume settings. Together, these findings support the application of an individualized approach to surgical intervention in older patients without clear evidence of aggressive thyroid cancer.
Limitations of this study are acknowledged. Most but not all thyroid nodules ≥1 cm in the cohort underwent evaluation with UG-FNA. This is because physician discretion likely favored UG-FNA of nodules with more concerning features, with conservative monitoring of lower-risk nodules. This could convey a source of selection bias. If true, however, inclusion of additional nodules that did not undergo UG-FNA would support the findings even further, since such low-risk sonographic nodules would most likely be benign. Not all patients with cytology SUSP underwent surgery potentially to diagnose and treat thyroid cancer, but it is notable that no thyroid cancer deaths were subsequently identified in such patients, consistent with the indolent course observed for most thyroid malignancies. Separately, though patients were evaluated with UG-FNA in this population, the possibility cannot be excluded that outcomes for many patients could have been similar if evaluated with US alone. Histopathologic diagnosis was not confirmed for all nodules, including those with indeterminate cytology, but it is notable that no thyroid cancer deaths were observed in such patients. Finally, determination of survival status was limited by use of the electronic medical records, and some patients were lost to follow-up, but the median follow-up of four years demonstrates a clinically important duration of continued evaluation.
In conclusion, these data confirm that US and UG-FNA assist with the initial risk assessment of thyroid nodules in patients aged ≥70 years by identifying those with benign cytology or by identification of sonographic/cytologic findings suggesting highly aggressive malignant disease. However, the surgical management of patients ≥70 years old presenting with lower-risk thyroid nodules (based on US and/or cytology), including those with indeterminate and non-diagnostic cytology, should be individualized, and a conservative approach favored given the significant potential for morbidity in comparison to more limited therapeutic benefit. This is particularly true for those with significant medical conditions such as CAD or other non-thyroidal malignancies at the time of initial evaluation.
Footnotes
Author Disclosure Statement
All authors above have no relevant disclosures.