
Abstract
Background:
Dysregulation of the phosphatidylinositol 3-kinase (PI3K) pathway is frequent in advanced follicular (FTC) and poorly differentiated thyroid (PDTC) carcinomas and has been implicated in oncogenesis and tumor progression. This study investigated the efficacy and safety of buparlisib, a pan-PI3K inhibitor in radioiodine refractory FTC and PDTC.
Methods:
The primary endpoint of this open-label, multicenter, phase 2 pilot study was progression-free survival (PFS) at 6 months. The sample size was determined considering that a PFS ≤50% at 6 months would denote an absence of benefits (null hypothesis). Secondary endpoints were objective response rate, PFS at 12 months, overall survival at 6 and 12 months, and safety based on the frequency and severity of adverse events (AEs).
Results:
Forty-three patients (19M/24 F; median age: 67 years) with metastatic, radioiodine refractory, progressive disease received buparlisib, 100 mg, daily. Histology was PDTC in 25 (58%), FTC in 17 (40%), and Hürthle cell carcinoma in 1 (2%). RAS mutation was found in 44% (12/27) and activation of the PI3K pathway in 35% (8/23) of tested tumors. The probability of PFS was 41.7% [95% confidence interval (CI) 7.7–55.5] at 6 months and 20.9% [CI 0–35.7] at 12 months, lower than the 50% expected PFS. At 6 months, 25.6% patients had stable disease, 48.8% were progressive and 25.6% had stopped treatment due to AE. The response to therapy was not influenced by age, sex, histology, or genetic alterations. The overall survivals at 6 and 12 months were 85.9% [CI 76–97] and 78.7 % [CI 67–92], respectively. The mean tumor growth rate decreased from 3.78 mm/month [CI 2.61–4.95] before treatment to 0.8 mm/month [CI −0.2–1.88] during treatment (p < 0.02). Severe grade 3–4 AEs occurred in 27 patients (63%), including hepatitis (25%), hyperglycemia (21%), mood disorders (12%), and skin toxicity (12%), with favorable outcome after temporary or permanent treatment discontinuation or dose reduction.
Conclusions:
Buparlisib did not result in significant efficacy in advanced FTC and PDTC. However, the decrease in tumor growth rate may suggest incomplete inhibition of oncogenic pathways and/or escape mechanisms. This should lead to evaluate combined therapy associating inhibitors of both the PI3K and mitogen-activated protein kinase pathways.
Introduction
T
Patients and Methods
Patients
Eligible patients were adult patients (≥18 years of age) with advanced radioiodine refractory, progressive, histologically confirmed FTC, PDTC, or Hürthle cell carcinoma. Patients were considered radioiodine refractory (i) when radioiodine uptake was absent in at least one target lesion on a post-therapeutic whole-body scan, (ii) when a target lesion was still persistent after a cumulative radioiodine activity of at least 600 mCi, or (iii) when the disease kept progressing 12 months after radioiodine treatment.
Eligible patients had a measurable disease and a documented progression (+20%) over the past 12 months as per the Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 (23). They may have received one or two previous lines of therapy with tyrosine kinase inhibitors but had to be off treatment for at least four weeks. The Eastern Cooperative Oncology Group performance status had to be less than three.
Patients previously treated with a PI3K inhibitor or currently receiving an approved or investigational antineoplastic drug, as well as patients who received wide field radiotherapy less than four weeks or limited field radiation for palliation less than two weeks prior to starting the trial were excluded from the trial. A history of cardiac dysfunction or a medication with a known risk of inducing prolonged QT interval or Torsades de Pointes were exclusion criteria as well as poorly controlled diabetes mellitus (HbA1c greater than 8%) and mood disorders.
Study design
The study was an open-label, one arm, multicenter, phase 2 study designed to evaluate the efficacy and long-term safety of buparlisib (BKM120) at a starting dosage of 100 mg per day. The study was approved by an independent ethics committee and registered on
Radiological assessments (per RECIST v1.1) were performed at 8-week intervals (±7 days) during the 6 first months, then every 3 months until month 12. CT scans were centrally reviewed (V.L.).
Histopathology of all the cases was reviewed by a specialist in thyroid pathology (M.D.), and classified according to the 2017 World Health Organization classification (24).
Laboratory tests were performed throughout the study period, and included thyrotropin, free thyroxine, free triiodothyronine, thyroglobulin determinations, hematology, and biochemistry. Safety was monitored by physical examination, electrocardiogram, cardiac imaging, and assessment of patient-rated questionnaires (Patient Health Questionnaire [9 Questions] and Generalized Anxiety Disorder Scale 7). Serious and nonserious adverse events (AEs) were monitored throughout the study, described per the Medical Dictionary for Regulatory Activities, v17.0, and graded per Common Terminology Criteria for Adverse Events (CTCAE) v4.03.
Tumor tissue from archival primary tumors was available in 32/43 patients. Twenty-eight were of sufficient quality for genotyping of TERT, BRAF, NRAS, and HRAS, which was performed as previously described (25). The mutational status of the PI3K pathway genes were assessed with Next Generation Sequencing (NGS) using an AmpliSeq® custom “cancer genes panel” on a PGM® instrument.
Endpoints
The primary objective of the study was the individual PFS at six months after the initiation of the treatment.
Secondary endpoints criteria were the objective response rate (defined as the proportion of patients with stable disease or partial tumoral response [per RECIST 1.1]) at 6 months and 12 months, the PFS at 12 months, the overall survival (defined as the time from treatment initiation to death from any cause) at 6 and 12 months, tumor size evolution, and safety based on the frequency and severity of AEs per CTCAE v4.03.
Additionally, the relationships between tumor genetic alterations and drug efficacy were studied.
Statistical analysis
The sample size of the study was determined considering that a PFS lower or equal to 50% at 6 months would denote an absence of benefits (null hypothesis). For an expected efficacy corresponding to a PFS of 70% at 6 months (alternative hypothesis) (5 –9), an alpha risk of 5% (unilateral test), the inclusion of 42 patients will allow to reject the hypothesis that PFS is under or equal to 50 % (null hypothesis) with a power of 84%.
Patient characteristics were described and compared between the three groups: patients with stable disease, patients with progressive disease, and censored patients (those who discontinued the treatment because of AEs). The comparisons used Fisher exact test for categorical variables and the Kruskal–Wallis test for quantitative variables.
The PFS curve was estimated using a nonparametric maximum likelihood estimator and taking into account interval-censored data (26). The 95% confidence intervals of PFS at 6 and 12 months were constructed using a modified bootstrap method with 200 replicates.
Overall survival at 6 months and 12 months (with their 95% confidence intervals) were estimated using the Kaplan—Meier method.
Differences between the minimum target-lesion size during treatment and the size at inclusion were computed for all the patients and represented graphically.
The tumor growth rate (TGR) was used to estimate the increase in size of a target lesion over time. This rate was estimated by dividing the size (sum of the three diameters) by the time and expressed in percentage increase per month (27). The method of analysis of the TGR is presented in the Supplementary Methods (Supplementary Data are available online at
All analyses were performed using R software (
Results
Forty-three patients were included in the study. Their characteristics are given in Supplementary Table S1. They included 19 males and 24 females with a median age of 67 years (range, 39–85 years). The median duration of disease since diagnosis of the primary tumor was 6.2 years (range, 1–28 years). Histology was PDTC in 25 cases (58%), FTC in 17 (40%) and Hürthle cell carcinoma in 1 (2%). Eighty-four percent had lung metastases, 61% had cervical and/or mediastinal lymph-nodes, 33% had bone metastases, and 12% liver metastases. Thirty-five per cent had undergone previous targeted therapy, and 61% received external radiation beam therapy.
Genetic alterations were identified in 23 out of the 28 tested tumors (82%). None had a BRAF mutation but 43% harbored a RAS mutation. Using NGS on 23 tumors, we found that the PI3K pathway was activated in 8 (35%), of whom 4 concomitantly had a RAS mutation. TERT was activated by somatic promoter mutation in 15 out of 27 tumors (57%) and associated with a RAS mutation in 8 cases (Supplementary Table S1).
As shown in Figure 1, the probability of PFS at 6 months was estimated to be 41.7% [95% confidence interval (CI) 7.7–55.5] and at 12 months 20.9% [CI 0–35.7]. The expected PFS at 50% at 6 months was therefore not reached. The overall survival was 85.9% [CI 76–97] at 6 months and 78.7 % [CI 67–92] at 12 months.

Disease-free survival at 6 and 12 months.
At 6 months, 11 patients (25.6%) had stable disease, 21 (48.8%) were progressive and 11 (25.6%) had stopped treatment for AE. At 12 months, 4 (9.3%) patients had stable disease, 26 patients (60.5%) had progressive disease, and treatment was discontinued in the other 13 (30.2%) for AE. Supplementary Table S2 shows that the response to therapy was not influenced by sex, age, histology, location of metastases, or previous therapies.
Waterfall plots of best responses are shown in Figure 2 for the 38 patients with at least one available evaluation during treatment. Two patients exhibited a 38 % and 50 % reduction in target lesions at 2 and 4 months but had concomitant progression of nontarget lesions.
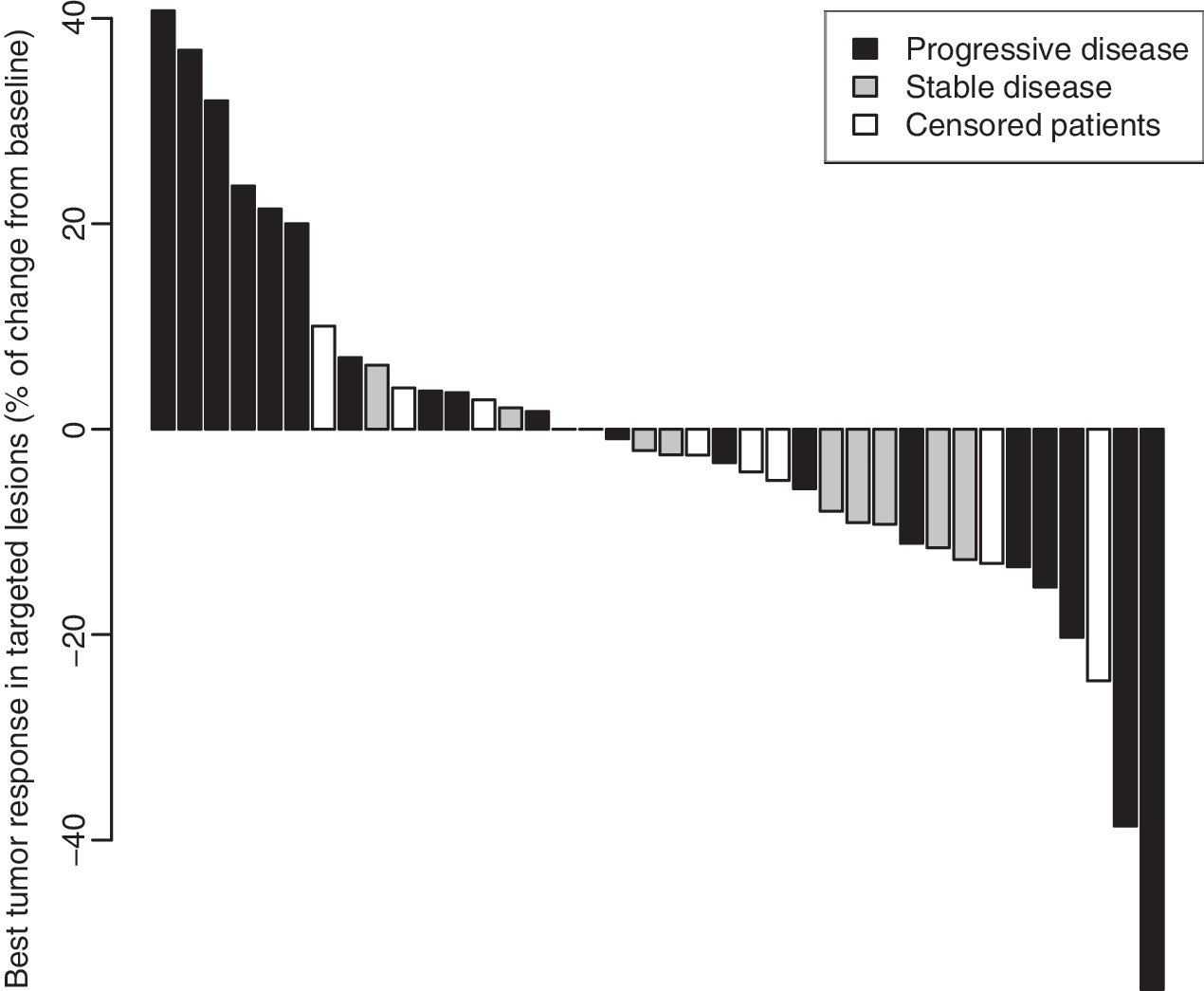
Waterfall plots of best tumor response in target lesions (% of change vs. baseline).
Individual responses in stable, progressive or censored patients (premature discontinuation of treatment for AE) are summarized in Supplementary Figure S1 and detailed in Supplementary Figures S2–S6 The mean TGR decreased from 3.78 mm/month before treatment to 0.8 mm/month during treatment (p < 0.02).
Tumor progression occurred in 50% (4/8) of patients with an activation of the PI3K pathway at NGS, in 50% (6/12) of patients with a RAS mutation and in 53% (8/15) of patients with a TERT mutation. Patients with stable disease at 6 months were RAS negative in 75%, without activation of the PI3 kinase pathway in 85%, and of TERT wild type in 75%.
As shown in Supplementary Table S3, AEs were recorded in 41 patients (95%) during the study. Twenty-seven patients (63%) presented at least one grade 3–4 AE related to treatment. The most frequent one was hepatitis occurring in 11 (25%) patients (9 grade 3 and 2 grade 4). All patients recovered without sequalae after definitive (n = 3) or transient (n = 8) treatment discontinuation. Hyperglycemia and/or diabetes occurred in 21% (9 patients, all grade 3), with complete recovery in 7 patients. Skin toxicity and mood disturbances were both reported in 5 patients (12%). No related drug AE was fatal. Seventeen patients deceased during the study from disease progression. The median delay to treatment discontinuation for AE was 4.2 months (0.4–10.0). The buparlisib dose had to be reduced in 58% of patients to improve tolerance. The risk of AE was not influenced by sex, age, previous treatment, histological type but was increased in patients with long disease duration (Supplemental Table S2).
Discussion
To our knowledge, this study is the first one to assess the effect of an oral pan-class I PI3K inhibitor in patients with thyroid cancer. We focused on poorly differentiated and follicular thyroid cancer because in these tumors there is a frequent activation of the PI3kinase pathway through mutations of RAS, epigenetic inactivation of PTEN, or activating mutations of PIK3CA and AKT1 (10 –16). Accordingly, genetic analyses that could be performed in two-third of patients, showed an activation of the PI3kinase pathway in 35% of cases and RAS mutations in 44%. Mutations of TERT were present in more than half of the patients.
We used buparlisib, a selective pan PI3K inhibitor tested in experimental studies and with encouraging results in some clinical trials (19 –22). Despite the strong rationale that supports this study, the objective of a 50% PFS at 6 months was not reached. The proportion of patients evaluable for the main objective was low, however, since 25% of patients discontinued treatment for AE. Previous studies with buparlisib have shown a safety profile consistent with that observed in the present study with frequent occurrence of hyperglycemia, hepatitis, mood disorders and skin toxicities (19 –22,29–30). Fortunately, all patients with drug induced toxicity recovered after permanent or temporary treatment discontinuation or dose reduction.
None of the patients had a partial response according to RECIST criteria (23). It has been suggested that RECIST criteria may be not be sufficiently sensitive to evaluate subtle responses to targeted therapies in metastatic carcinomas. The tumor growth rate (TGR), which incorporates the time between evaluations, allows for a quantitative characterization of drug activity and has been shown independently associated with prognosis (28). Patients included in this study had highly progressive disease at inclusion with a TGR of 3.8 mm/month. TGR significantly slowed down during treatment. This may suggest incomplete inhibition of the PI3kinase pathway or the existence of other mechanisms promoting tumor growth (31), but the design of this single arm study does not allow a definite conclusion.
In accordance with our study, disappointing results have been obtained, recently, with buparlisib in patients with non-small cell lung cancer and breast cancer although an activation of the PI3kinase pathway was present in all patients (29–30). This underlines the difficulties in developing effective predictive biomarkers to be used in clinical trials and practice (31). One question is whether identification of somatic mutations in the primary tumor is representative of the mutational status of metastases (13 –16), and recent evidence suggests that other defects may occur during tumor progression (11 –13).
Whatever the involved mechanism of this low response rate may be, targeting multiple pathways simultaneously may improve anti-tumor efficacy and promising clinical results have been reported, recently, with the combination of MEK and BRAF inhibitors (17,32 –35).
In conclusion, targeted PI3Kinase inhibition by buparlisib did not result in a significant anti-tumoral effect in thyroid cancer. However, slowing down the tumor growth rate may suggest incomplete PI3K inhibition and/or the existence of other mechanisms that lead to tumor growth and this may suggest the potential interest of combined therapy associating with MEK or BRAF inhibitor with PI3K/AKT inhibitors
Footnotes
Aknowledgements
This work was supported by Novartis Pharmaceuticals Corporation (no grant number applies). We thank Mrs. Irene Zublena and Dr. Valerie Plattner from the Delegation à la Recherche Clinique et l'Innovation des Hospices Civils de Lyon, Mrs. Emeline Blanc and Marina Ndong from the Pharmaco-Vigilance Unit (Hospices Civils de Lyon) for their help in the realization of the trial as well as Jean Iwaz (Hospices Civils de Lyon) for the revision of the final version of the manuscript.
Author Disclosure Statement
F.B.C. has received honoraria, consulting fees and research funding from Novartis and Bayer. P.N. has received research funding from Novartis, Bayer and Eisai. J.W. has received honoraria from Eisai. C.D.C. has received honorarium from Bayer, Novartis and Esai. S.L. has received consulting fees from Bayer and research Grant from Novartis. A.T. received honoraria, speakers fees, and research funding from Novartis. C.dlF. received research funding from Bayer and Novartis and consulting fees from Eisai and Bayer. M.S. has received honoraria, consulting fees and research funding from Bayer, and Eisai. E.D., F.I., J.L., M.K., M.C.E., D.B., C.B., H.L., A.D., M.R., V.L., M.D.P. have no competing financial interests.