
Abstract
Background:
Intraoperative neural monitoring (IONM) has gained widespread acceptance as an adjunct to the gold standard of visual identification of the recurrent laryngeal nerve (RLN) during thyroid surgery. Currently, laryngeal electromyography (EMG) recording during IONM is almost always performed using endotracheal tube (ETT) surface electrodes placed adjacent to vocal folds originating from the inner surface of the thyroid cartilage (TC). Therefore, it was hypothesized that surface recording electrodes placed on the outer surface of the TC should enable access to the EMG response of the vocal folds during IONM. The aim of this experimental study was to evaluate the feasibility of the transcartilage approach for laryngeal EMG recording during IONM.
Methods:
A porcine model (12 pigs and 24 RLN sides) with well established applicability in IONM research was used for the experiments. Both ETT electrodes adjacent to vocal folds and adhesive pre-gelled electrodes on the TC were used for EMG recording during IONM. Electrically evoked EMG signals detected by both electrode types were recorded and analyzed. EMG changes during tracheal displacement and RLN traction injury were compared.
Results:
Both the ETT and TC recording electrodes recorded typical laryngeal EMG waveforms evoked by a 1 mA stimulus current applied on both sides of the RLNs and vagus nerves (VNs). Under RLN stimulation, the mean EMG amplitudes recorded with the ETT and TC electrodes were 973 ± 79 μV and 695 ± 150 μV, respectively. Under VN stimulation, the mean amplitudes were 841 ± 163 μV and 607 ± 162 μV, respectively. When upward displacement of the trachea was experimentally induced, the TC electrodes showed less variation in recorded EMG signals compared to ETT electrodes. When RLN traction stress was experimentally induced, both the ETT and TC electrodes accurately recorded the typical EMG pattern of progressively degrading amplitude and gradual recovery after release of traction.
Conclusions:
This study confirms the feasibility of using transcartilage surface electrodes for recording laryngeal EMG signals evoked during IONM in an animal model. However, before practical application of this approach in clinical thyroid surgery, further studies are needed to improve electrode designs by optimizing their shapes and sizes, and increasing their adhesive stability and sensitivity.
Introduction
A
Currently, monitoring systems that use endotracheal tube (ETT) surface electrodes are the most widely used commercially available monitoring systems (3). These ETT-based systems record electromyographic (EMG) data from the vocal folds (i.e., thyroarytenoid or vocalis muscles). During IONM, a handheld stimulation probe is used to evoke the laryngeal EMG response by depolarizing the RLN or vagus nerve (VN). The EMG response is typically quantified by both the amplitude and latency of the signal obtained during RLN or VN stimulation. The EMG amplitude may correlate with the number of depolarized muscle fibers, which then affects RLN function. Latency is related to the time of the conducted action potential and response (12 –14). The main limitation of ETT-based systems is that a high-quality recording requires constant contact between the electrodes and vocal folds during surgery (3,13,15 –18). A malpositioned or displaced ETT can cause false IONM signals (8,11,13,15 –17,19), resulting in the need for intraoperative verification or readjustment of the ETT position, which can be complicated and time-consuming.
Since the vocal fold originates from the inner surface of the thyroid cartilage (TC; Fig. 1A), it was hypothesized that surface recording electrodes placed on the outer surface of the TC should obtain recordings of the EMG response of the vocal fold. It was also hypothesized that compared to ETT electrodes, the TC electrodes would obtain less affected EMG signals during tracheal movement and would detect similar adverse signals caused by RLN injury. Thus, this study evaluates a novel transcartilage approach in which noninvasive adhesive surface electrodes were attached to the outer surface of the TC (Fig. 1A and B) for recording EMG signals during IONM. Experiments were performed to evaluate the feasibility of the proposed approach and to compare its signal stability and accuracy with that of conventional ETT-based systems (Fig. 1C and D).
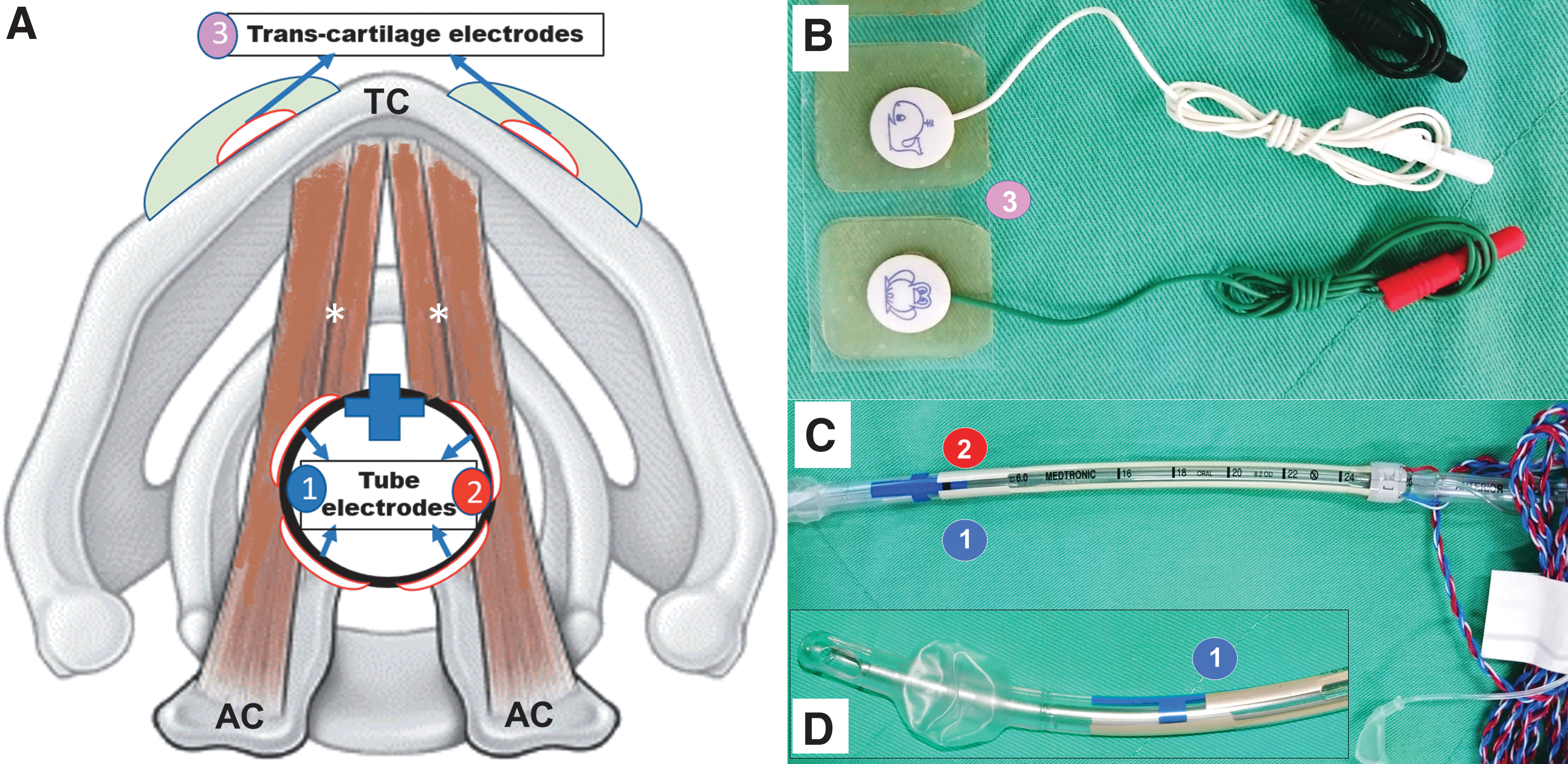
Anatomic relationship between the larynx and the surface recording electrodes used for intraoperative neuromonitoring in thyroid surgery. (
Methods
Experimental animals, anesthesia, and ETT surface electrodes
Twelve male pigs (age 3–4 months; weight 20–25 kg) obtained from the Laboratory Animal Center of Kaohsiung Medical University, Taiwan, were studied. The study protocol was approved by the Institutional Animal Care and Use Committee of Kaohsiung Medical University. All experiments were performed according to institutional guidelines that comply with national and international regulations for animal experiments, including the 3R principles (replacement, reduction, and refinement). The porcine model used for the experiments in this study is well established in RLN and IONM research, and the EMG parameters (amplitude, latency, and threshold) of the model are consistent with human data (12,20 –22).
Each animal was premedicated with intramuscular azaperone (4 mg/kg) 30 min before the experiment. With the animal in a prone position, general anesthesia was induced by inhalation of 2–4% sevoflurane in oxygen administered from a plastic bottle. A bolus of propofol 1 mg/kg was administered intravenously with a 24-gauge peripheral intravenous catheter placed on the ear. The pig was then intubated with an EMG ETT (TriVantage EMG tube, size 6 ID; Medtronic, Jacksonville, FL; Fig. 1C). The proper EMG tube position was verified and confirmed by the anesthesiologist. After positional stabilization of the tube, the pig was placed in the supine position with the neck extended (Fig. 2A). Anesthesia was maintained with 1–3% sevoflurane in oxygen. The lungs were ventilated in volume-control mode at a tidal volume of 8–12 mL/kg, and the respiratory rate was set to 12–14 breaths/min. Body temperature was maintained with a circulating water mattress maintained at 40°C.
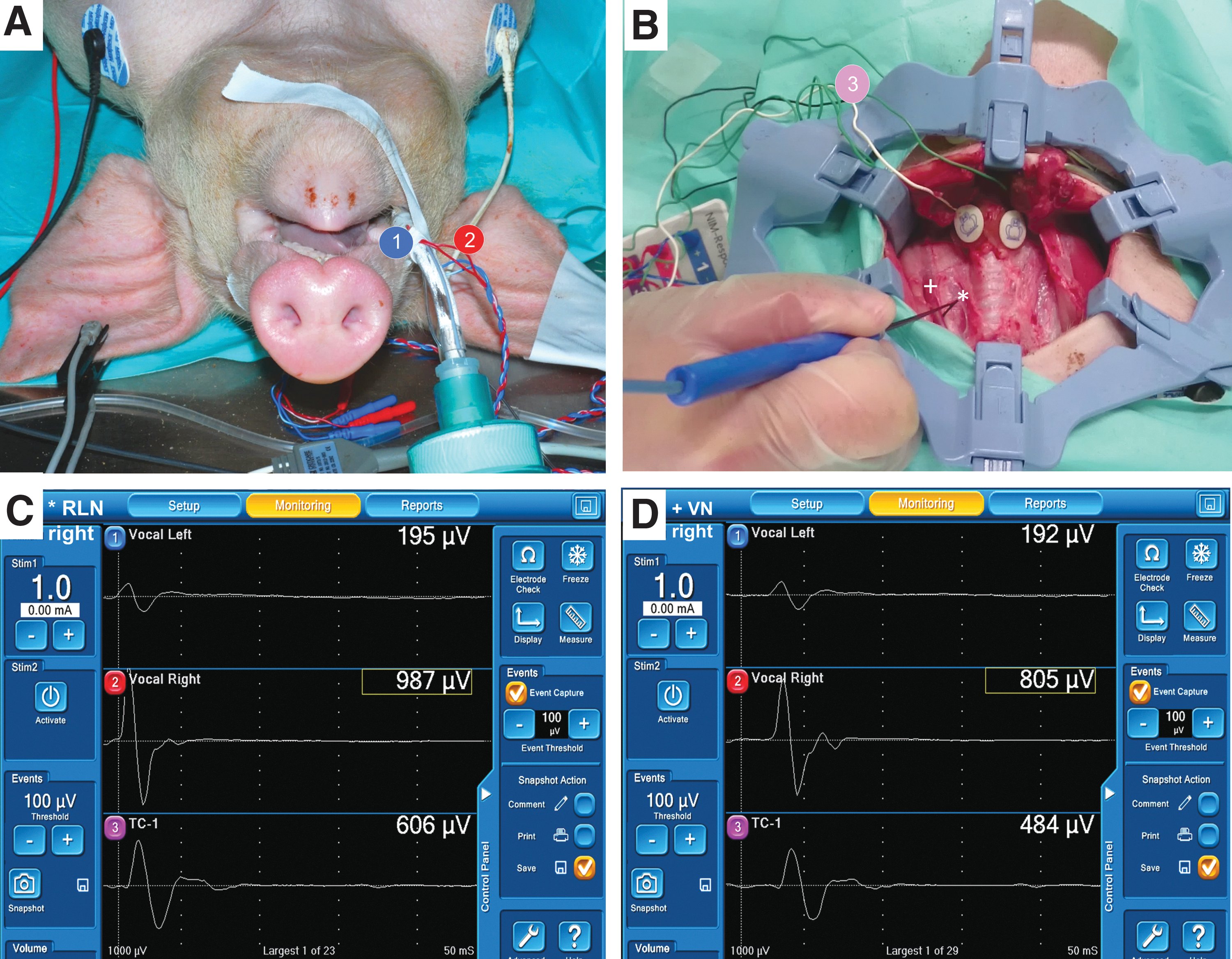
Setup of the ETT and the TC surface recording electrodes for intraoperative neuromonitoring in a porcine model. (
Operation, TC surface electrodes, and experimental design
A long, transverse neck skin incision was made, and subplatysmal flaps were raised. The neck was exposed with a self-retaining thyroidectomy retractor (WIDOX®; MOSS Spa, Lesa, Italy). A pair of adhesive pre-gelled electrodes (Neotrode II®; ConMed Corp., Utica, NY) were attached to the left and right lamina of the TC (Fig. 2B). The channel leads from the EMG ETT and TC electrodes were connected to the monitoring system (NIM-Response 3.0; Medtronic). The monitoring system generated stimuli with a time window set to 50 ms and an amplitude scale set to 0.2 mV/division. The pulsed stimuli were 100 μs in duration and 4 Hz in frequency. The event capture was activated at a threshold of 100 μV.
In each pig (n = 12), bilateral RLNs (n = 24) and VNs (n = 24) were localized, identified, and carefully exposed with a handheld stimulation probe (ball-tip 1 mm; Medtronic; Fig. 2B). Each nerve was stimulated with a 1 mA current, and the waveform morphologies of the electrically evoked EMG signals detected by both the ETT and TC electrodes were displayed on the monitor (Fig. 2C and D). Baseline amplitudes and latencies of EMG responses were recorded for further analysis.
After baseline EMG data for both ETT and TC electrodes were documented, the stability of EMG signals recorded by both electrode types during surgical manipulation was evaluated and compared under experimentally induced tracheal displacement in each pig (Fig. 3A and B). In four animals, the accuracy of the ETT and TC electrodes in reflecting adverse EMG changes of stressed RLN was further evaluated and compared under experimentally induced RLN traction during continuous IONM (Fig. 3C and D).
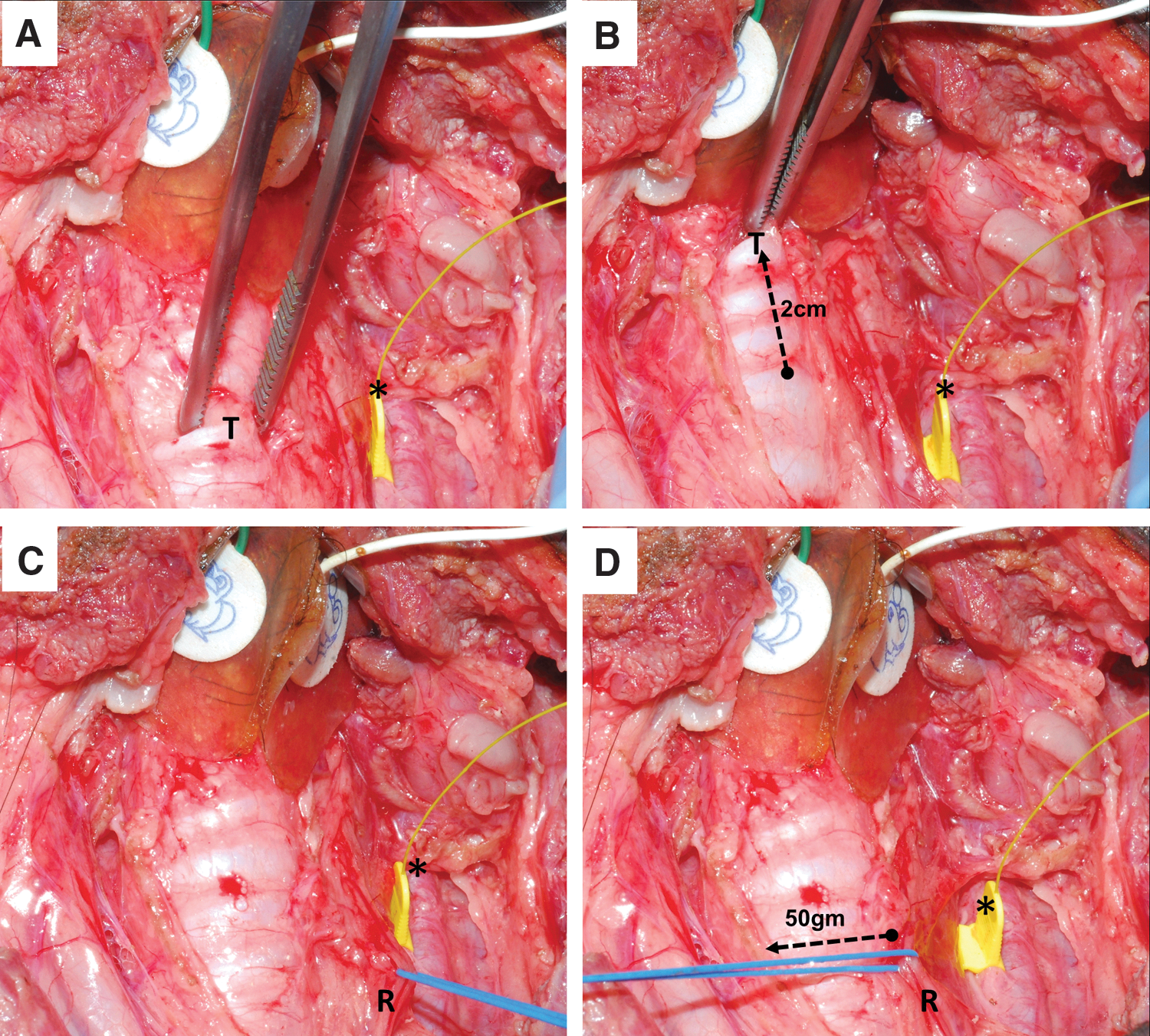
Experimental designs for trachea/cricoid displacement and nerve traction injury studies. (
Statistical analysis
Recorded EMG data are expressed as the mean ± standard deviation. Mean EMG amplitudes and mean EMG latencies for each stimulation site were compared using paired t-tests. All p-values are two-tailed, and a p-value of <0.05 was considered statistically significant. All statistical analyses were performed using Excel 2016 (Microsoft, Redmond, WA).
Results
This study analyzed left and right RLNs and VNs in 12 pigs (24 VNs and 24 RLNs). In all animals, both the ETT and TC electrodes successfully recorded typical evoked laryngeal EMG waveforms from the RLNs and VNs under stimulation with 1 mA (Fig. 2C and D).
Figure 4 compares the evoked laryngeal EMG amplitudes and latencies recorded from the ETT and TC electrodes. In each group, the ETT electrodes recorded significantly higher EMG amplitudes compared to the TC electrodes (p < 0.05). However, ETT electrodes and TC electrodes did not significantly differ in recorded EMG latency data (p > 0.05). Mean EMG amplitudes recorded under RLN stimulation were 973 ± 179 μV for ETT electrodes and 695 ± 150 μV for TC electrodes. Mean EMG amplitudes recorded under VN stimulation were 841 ± 163 μV for ETT electrodes and 607 ± 162 μV for TC electrodes. Mean EMG latencies recorded under RLN stimulation were 2.96 ± 0.15 ms for ETT electrodes and 3.01 ± 0.18 ms for TC electrodes. Mean EMG latencies recorded under right VN stimulation were 4.75 ± 0.24 ms for ETT electrodes and 4.79 ± 0.28 ms for TC electrodes. Mean EMG latencies recorded under left VN stimulation were 8.22 ± 0.72 ms for ETT electrodes and 8.25 ± 0.65 ms for TC electrodes.
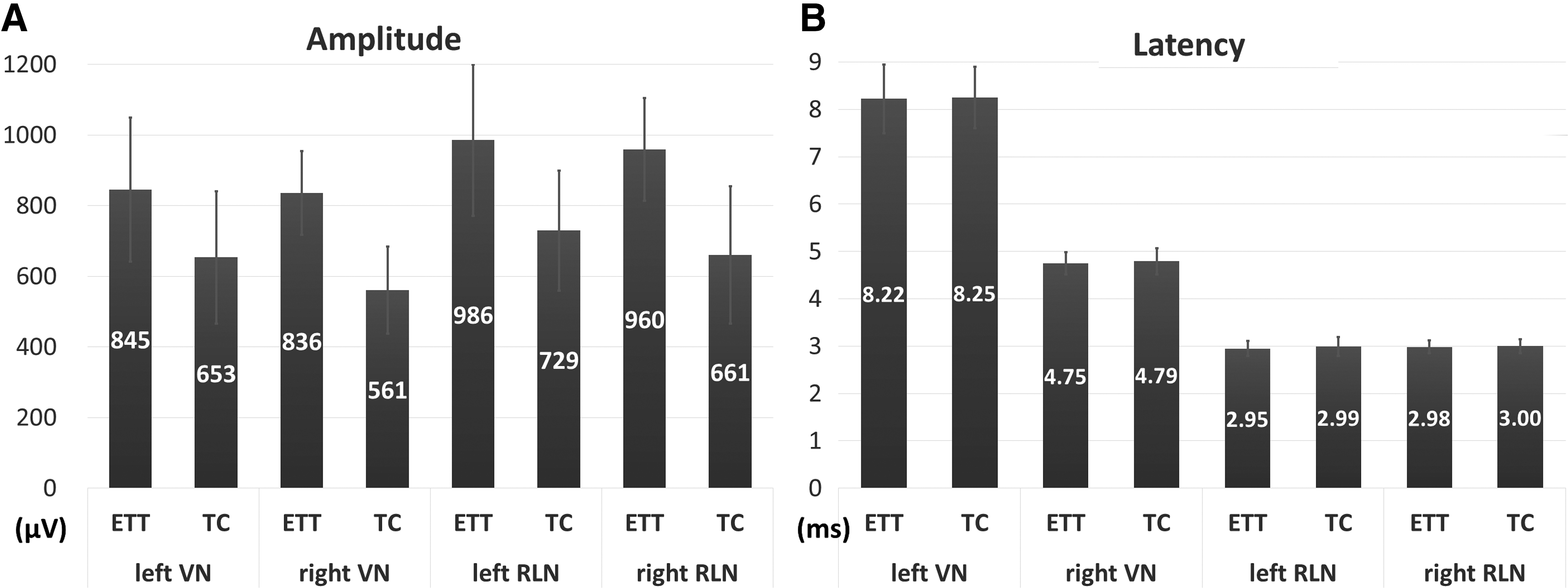
Comparison of left- and right-side evoked laryngeal EMG responses between the ETT and TC electrodes during intraoperative neuromonitoring. (
The tracheal displacement study evaluated the real-time EMG signal changes recorded by ETT and TC electrodes. The results showed that in both electrode types, tracheal displacement affected the recorded EMG signals (Fig. 5). The mean changes in EMG amplitude recorded after upward displacement of 1 cm were 7.8 ± 1.7% (range 5–11%) for ETT electrodes and 45.6 ± 8.2% (range 28–53%) for TC electrodes. The mean changes in EMG amplitude recorded after upward displacement of 2 cm were 14.3 ± 4.6% (range 8–25%) for ETT electrodes and 68.4 ± 10.6% (range 53–85%) for TC electrodes.
Comparison of real-time electromyography (EMG) signals recorded by (i) Vocalis electrode on ETT and (ii) transcartilage electrode on TC when tracheal displacement was experimentally induced. The EMG amplitude from the ETT electrodes showed >50% decrease (red dot line) when the trachea was displaced >1 cm. The EMG signals from the TC electrodes were relatively less affected by the tracheal displacement. Color images available online at
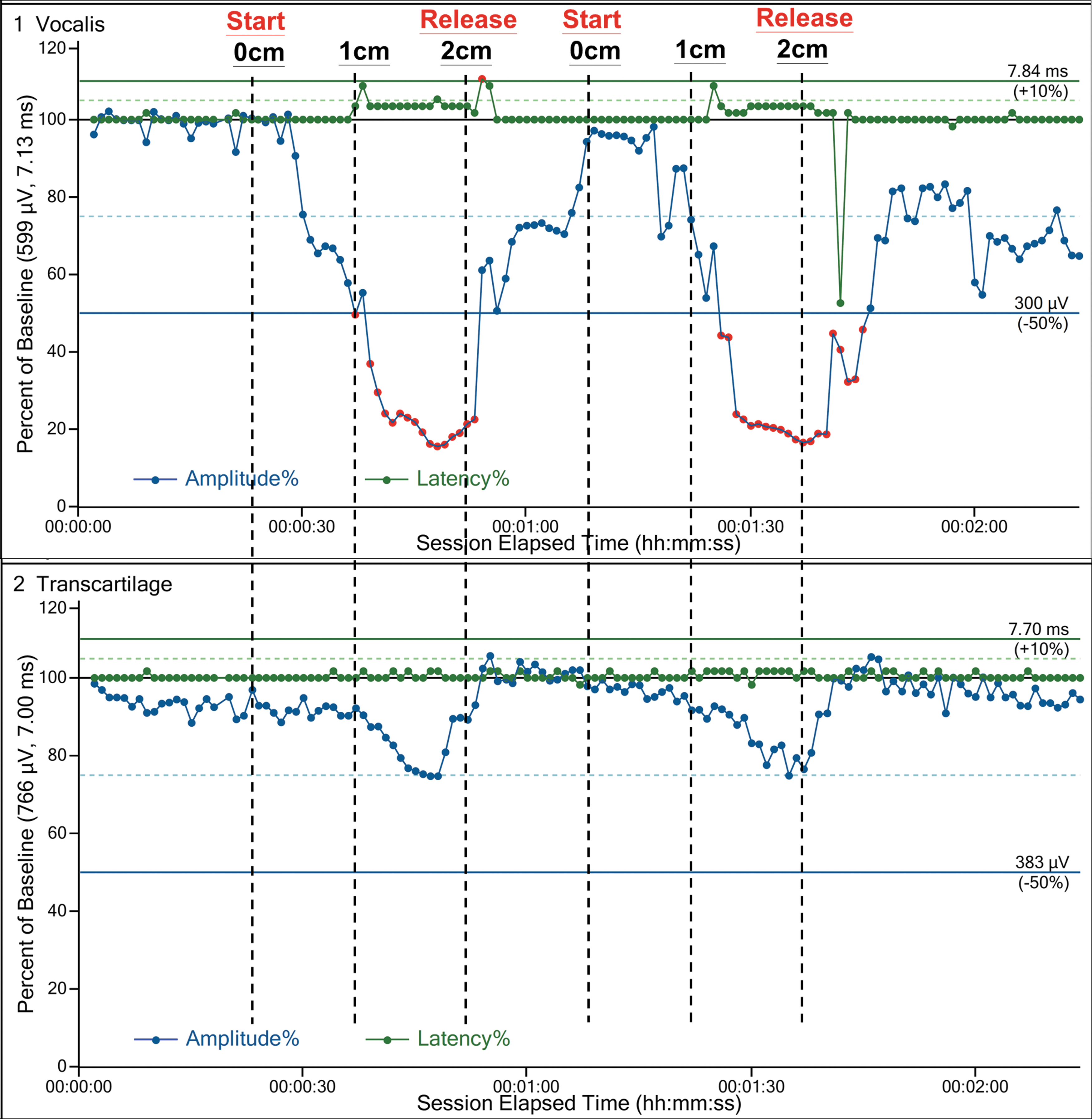
The RLN traction stress study evaluated the real-time EMG signal changes recorded by ETT and TC electrodes in four animals. Real-time EMG tracings obtained under RLN traction stress induced in all four experimental animals showed that both ETT and TC electrodes accurately recorded the typical EMG evolution pattern of progressively degrading amplitude and then gradual recovery after release of traction (Fig. 6).

Comparison of real-time EMG signals recorded by (i) Vocalis electrode on ETT and (ii) transcartilage electrode on TC when RLN traction stress was experimentally induced. Both ETT and TC electrodes accurately recorded typical patterns of progressive EMG amplitude degradation during RLN traction with 50 g-force. Both electrodes also recorded the typical patterns of gradual EMG amplitude recovery of after release of traction force. Color images available online at
Discussion
It was hypothesized that surface recording electrodes on the outer surface of the TC can obtain the EMG response of the vocal fold during IONM (Fig. 1). This hypothesis was tested in a porcine model with well established applicability in RLN and IONM research (12,20 –22). The experiments confirmed that a pair of surface recording electrodes attached to the TC is as feasible as ETT electrodes for recording evoked laryngeal EMG responses under 1 mA stimulation of the RLN or VN (Fig. 4). During experimental upward displacement of the trachea, the EMG signals obtained by TC electrodes showed less variation compared to those obtained by ETT electrodes (Fig. 5). When RLN traction stress was experimentally induced, both the ETT and TC electrodes accurately recorded the typical pattern of EMG evolution, that is, progressively degrading amplitude and gradual recovery after release of traction (Fig. 6). These experimental results indicate that this novel transcartilage approach is a feasible alternative to using ETT electrodes to monitor RLN function during thyroid surgery.
Direct visualization of the RLN is considered the gold standard for preventing RLN injury during thyroid surgery (23,24). The predominant mechanism of RLN injury is nonstructural functional nerve injury, not transection (8,9,25). Therefore, IONM is increasingly used for functional electrophysiologic assessment of the RLN in addition to visual confirmation of RLN structural integrity (3). In thyroid surgery, IONM is almost always performed with commercially available ETT surface recording electrodes placed adjacent to the vocal folds. For accurate monitoring, the ETT must be the appropriate size and must be correctly aligned (13,18). In addition, intraoperative manipulation and traction of the thyroid lobe and trachea can easily displace the contact between the ETT electrodes and vocal fold. Correcting the resulting false IONM results may require the anesthesiologist to verify and readjust the electrodes intraoperatively (8,11,13,15 –17). Several studies have investigated alternative recording approaches to address the limitations of ETT electrodes. For example, Alon and Hinni (26) and Petro et al. (27) described the use of one or two paired needle electrodes inserted through the cricothyroid membrane and into the thyroarytenoid muscles. Recently, Chiang et al. (28) described the use of two single needle electrodes inserted into the sub-perichondrium of the TC for IONM of the RLN. Needle electrode approaches theoretically overcome most limitations of ETT electrodes but are not entirely noninvasive. Needle electrodes can still cause laryngeal hematomas, lacerations, infections, or ruptured endotracheal cuffs. Additionally, a needle electrode insertion may be difficult due to scar tissue in revision surgery or due to calcified TC in older adults. The Massachusetts Eye and Ear Infirmary group recently reported their animal experiments (29) and preliminary clinical experience (30) in using postcricoid surface electrodes to obtain EMG waveforms at the posterior cricoarytenoid (PCA) muscle. Although their experimental results showed that postcricoid electrodes reliably recorded PCA EMG waveforms, constant verification of contact between the postcricoid electrodes and PCA muscle may be required because the postcricoid electrodes are susceptible to displacement during surgical manipulation.
Ideally, the recording method used during IONM should be noninvasive, reliable, reproducible, easy to perform, and cost-effective. Compared to ETT electrodes and intramuscular or intracartilage needle electrodes, an adhesive electrode placed on the TC is ostensibly simpler, faster, and less invasive, that is, it does not leave needle tracts and should cause less trauma in the mucosa, cartilage, or muscles. Adhesive electrodes are also less expensive. In our institution, for example, an EMG ETT or a paired needle electrode costs several hundred dollars more than an adhesive electrode.
However, the transcartilage recording method and the adhesive pre-gelled electrodes (Neotrode® II; Fig. 2B) used in the current study have several notable limitations. First, the transcartilage recording method requires a larger incision to expose the TC. This method slightly increases surgical time and may not be useful for procedures in which a minimally invasive approach is desirable. In the case of a large goiter extending to the TC, prelaryngeal dissection of the pyramidal lobe is required before placement of TC electrodes. Second, the size and shape of this electrode type are designed for ECG recording on the chest skin of young children. Therefore, these electrode types are somewhat larger than necessary for use on the TC. Recording traces can be distorted by the far field potentials from multitude of muscles attached to the larynx and underlying the surface electrodes (e.g., sternohyoid muscle, thyrohyoid muscle, and inferior constrictor muscle). For example, the experiments in this study showed that a stimulation current >10 mA causes some shunt stimulation of the ansa cervicalis and/ or the strap muscles. Evoked muscle potentials could be recorded more easily by large surface electrodes on the TC. However, no obvious far field potentials were recorded under the standard stimulation current of 0.5–3 mA (Fig. 1C and D). Therefore, new electrode designs with sizes and shapes optimized for TC recording are needed, and further animal and clinical studies are needed to evaluate their susceptibility to far field potentials.
Third, although this study shows that TC electrodes obtained more stable signals than ETT electrodes did during upward displacement of the trachea, the adhesive pre-gelled surface electrodes may still be dislodged during surgical manipulations. Dislodgement can occur because the vector of manipulative force applied during clinical thyroid surgery tends to include both rotatory force and displacement. Rotatory force would likely displace the contact between the ETT electrodes and vocal fold and may also dislodge the TC surface electrodes. Although a dislodged TC electrode can be confirmed by direct visualization and can be corrected immediately, the troubleshooting algorithm for loss of signal must be modified to address this limitation. To minimize dislodgement, the stability of future electrode designs must be increased by improving their adhesion to the TC. Smaller electrodes are also needed to minimize the possibility of damage to cartilage or nearby muscles upon electrode removal. Finally, the mean EMG amplitude recorded with adhesive electrodes on the outer surface of the TC was lower than that recorded with ETT electrodes. Although the difference in amplitude resulted from a procedural difference (i.e., direct contact with ETT electrodes but indirect contact with TC electrodes), further studies are needed to evaluate whether the sensitivity of surface electrodes can be improved by using different electrode materials and different transduction mechanisms of surface electrodes.
This in vivo animal study has a few additional limitations. First, this study was performed using a porcine model with a moderate sample size. However, this model has proven useful and effective for evaluating electrophysiologic correlates of laryngeal EMG during IONM in previous studies (20 –22). In addition, this approved animal study applied 3R principles (replacement, reduction, and refinement) and revealed good reproducibility between tested animals. A second limitation is the differences in cartilage ossification between juvenile pigs and adult humans. Since cartilage ossification can substantially impair recording of compound muscle action potential responses, further studies in human subjects are needed.
In conclusion, this study confirms the hypothesis that surface recording electrodes on the outer surface of the TC enable access to the EMG response of the vocal fold during IONM of the RLN. A remaining challenge in the practical clinical application of transcartilage IONM is development of surface electrodes that provide a desirable combination of proper size/shape, high adhesive stability, and high sensitivity.
Footnotes
Acknowledgments
Part of this study was orally presented at the 3rd World Congress on Thyroid Cancer, July 27–30, 2017, in Boston. The authors gratefully acknowledge the technical assistance provided by Pao-Chu Hun (veterinarian, Laboratory Animal Center, KMU). This study was supported by grants from the Kaohsiung Medical University Hospital, Kaohsiung Medical University (KMUH106-6R49) and the Ministry of Science and Technology, Taiwan (MOST 105-2314-B-037-010, 106-2314-B-037-042-MY2).
Author Disclosure Statement
The authors have no conflict of interests to declare.