
Abstract
Background:
The recent update of The Bethesda System for Reporting Thyroid Cytology (TBSRTC) is a very important development in the evaluation of thyroid nodules. Clinical experience and scientific literature both show that practitioners performing thyroid fine-needle aspiration are accustomed to basing the clinical management of patients on reports using TBSRTC. Specifically, clinicians are familiar with the percent risk of malignancy corresponding to each TBSRTC diagnostic category (DC), as well as with the respective recommendation for clinical management. However, most clinicians are much less familiar with the specific considerations that lie between a given DC, on the one end, and the respective risk of malignancy and associated management recommendation, on the other end.
Summary:
A deeper understanding of the system can enlighten the clinician's thinking about the specific nodule under examination and can guide the decision-making process in a more meaningful way. Such an understanding can only be developed via close two-way communication between cytopathologists and clinicians. Through this type of interaction in the authors' tertiary medical center, recurring issues of particular importance for clinical practice were identified, which are reported here in the form of 16 frequently asked questions posed by the clinician to the cytopathologist.
Conclusions:
For each frequently asked question, an answer is provided based on the literature, the authors' experience, the new version of TBSRTC, and the new World Health Organization classification of tumors of endocrine organs.
Introduction
T
Recently, the second edition of TBSRTC was published (13). The update was necessary for two main reasons. First, recent advances in the molecular diagnosis of thyroid nodules made it important to specify their place in the post-FNA management algorithm for each specific DC. Second, the noninvasive encapsulated follicular variant of papillary thyroid carcinoma (FV-PTC) was renamed as noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), and it was recognized by the new World Health Organization (WHO) classification of tumors of endocrine organs as a lesion whose malignant potential is much lower than that of conventional papillary thyroid carcinoma (PTC) (14). As a consequence, the recalculated ROM ranges also needed to take into account whether NIFTP is considered as a carcinoma (15).
The update of TBSRTC is thus a very important and welcome development. Indeed, clinical experience shows that practitioners performing thyroid FNA are accustomed to basing the clinical management of the patients on reports using TBSRTC. Specifically, clinicians are familiar with: (i) the percent risk of malignancy associated with each TBSRTC diagnostic category and (ii) the respective recommendation for clinical management (the options in the original version were: observe, repeat FNA, or refer for surgery). However, most clinicians are much less familiar with the specific considerations and details that lie between a given DC, on the one end, and the respective ROM and associated management recommendation, on the other end. This is unfortunate, since a deeper understanding of the system can enlighten the clinician's thinking about the specific nodule under examination and can guide the decision-making process in a more meaningful way. Such an understanding can only be developed via close two-way communication between the cytopathologist and the clinician. Based on this type of interaction in the authors' thyroid clinic, as well as on an informal survey among endocrinology colleagues dealing routinely with thyroid patients in the authors' tertiary medical center, recurring issues of particular importance for clinical practice were identified, which are reported here in the form of frequently asked questions (FAQ) posed by the clinician to the cytopathologist. For each FAQ, an answer is provided based on the literature, the authors' experience, the new version of TBSRTC, and the new WHO classification of tumors of endocrine organs (13,16).
FAQ 1: What Are the Most Important Modifications in the Updated Version of TBSRTC?
The most important modification in the updated version of TBSRTC concerns the ROM. First, the ROM ranges have been updated according to the most recent literature data. Moreover, for each DC, two different ROM ranges are indicated: one by considering NIFTP as carcinoma and the other by considering NIFTP as a nonmalignant or premalignant lesion.
The general schema of six DCs is maintained, as well as the designation of each individual DC. The updated version of TBSRTC includes some explanations that were necessary to avoid subjective interpretations possible in the previous classification. In particular, the AUS/FLUS DC should not be split, meaning that it should not be used to identify separately cases with cytological (mostly nuclear) atypia—that is, AUS—and cases with architectural (mostly microfollicular) atypia—that is, FLUS. The terms “AUS” and “FLUS” are to be considered synonymous and used together as AUS/FLUS. The same applies to the terms “FN” and “SFN” (FN/SFN). The cytopathologist has the option of adding a descriptive comment to this DC (as to all other DCs), which may be useful to predict the histological diagnosis of the lesion in question better. This is particularly important after the reclassification of the noninvasive encapsulated FV-PTC as NIFTP. In the authors' institution, in case of cytological features suggestive of NIFTP, the following comments are added to the diagnosis as a note: “The presence of rare atypical nuclear features in this follicular-patterned lesion suggests the possibility of a FV-PTC or NIFTP.”
The advent of NIFTP also made an adjustment in the FN/SFN DC necessary. In the updated version, cases with slight nuclear atypia are also included in this DC, and they can correspond to NIFTPs found on histology. Conversely, because the M DC must retain a high positive predictive value for cancer, it should comprise only cases with multiple typical nuclear features of PTC. These can include nuclear enlargement, nuclear membrane irregularities, frequent nuclear grooves, abnormal chromatin clearing, and/or nuclear inclusions. Cases of NIFTP typically have less well-developed nuclear atypia and almost never have nuclear inclusions. Psammoma bodies are rare in FNAC specimens but are very helpful when present, as they are not found in NIFTP. By definition, papillary arrangement is also absent in NIFTP. Given that papillary architecture excludes NIFTP, it is important to be aware that nodules can still be classified in the M DC as a cytological diagnosis of PTC, even if they do not display abundant papillary structures, because the latter are not always present and thus are not necessary for diagnosis. In such cases, the diagnosis is usually supported by the presence of abundant and convincing nuclear atypia.
FAQ 2: What Are the Reasons for a ND/UNS Classification? Does It Depend Primarily on the Nodule, the FNA Operator, or the Cytopathologist? And What Are the Implications?
A ND/UNS classification normally does not depend on the cytopathologist because she or he needs to follow specific predefined criteria to evaluate the quality and adequacy of the sample (cf. FAQs 5–7 for more details). In that sense, it is unlikely that a more “defensive” cytopathologist will triage borderline and/or difficult cases into the ND/UNS DC (but rather into the AUF/FLUS DC; cf. FAQs 7–9).
There are some rare types of nodules that can be associated with a high risk of ND/UNS results, such as solitary fibrous tumors, schwannomas, fibrotic Hashimoto's disease, or Riedel's thyroiditis. In these cases, the target lesion contains very few, if any, follicular cells.
In the majority of cases then, the reason for ND/UNS DC rests with the FNA operator, and it has to do with poor technique in sampling, slide preparation or fixation (cf. FAQs 5 and 7 for more details on specific quality issues). According to the Bethesda guidelines, no more than 10% of specimens should be classified as ND/UNS. However, the percentage of nodules classified as ND/UNS in real life varies widely in the literature, ranging from 1–2% to as high as 45–50% (17). The higher end of this spectrum is way beyond the acceptable 10% threshold and thus clearly reflects poor practice. At this higher end, the ROM could also be significantly impacted, especially if there is a systematic bias, associated with the underlying reason for the high percentage of ND/UNS specimens, notably marginal specimens due to poor sampling or preparation techniques. Therefore, in order to keep the rate of ND/UNS reports as low as possible, or at least within acceptable limits (10%), specimen quality is of paramount importance. This is why it is imperative that non-cytopathologist operators who perform thyroid FNA (most commonly endocrinologists or radiologists) receive dedicated training on quality issues related to FNA technique and sample preparation (18). Those who do not meet the 10% benchmark should be made aware (e.g., by their cytopathologist, or by their clinical supervisor if still in training) and further structured training to reach this goal should be expected.
Poor specimen quality is a main cause of false-negative diagnoses. This can occur when the material is either not representative or so scant or poorly preserved that neoplastic cells cannot be identified (18). In addition, poor specimen quality is also implicated in false-positive diagnoses, when the cytopathologist attempts to force a diagnosis in cases with marginal material (18). Thus, high rates of ND/UNS samples cause increased cost and morbidity associated not only with repeat testing but also with unnecessary surgery. Indeed, a substantial number of patients with ND/UNS results, especially after repeat FNA, will be addressed for surgery (cf. FAQ 3), and it is well-known that after thyroid surgery about 2% of patients suffer from permanent laryngeal nerve damage and about 2% suffer from postoperative hypoparathyroidism.
FAQ 3: When a Nodule Yields a ND/UNS Result, Is It More or Less Likely To Be Malignant?
The malignancy risk associated with a non-diagnostic category was not clearly stated in the original TBSRTC publication (7). According to a large meta-analysis, the malignancy risk of this category, calculated among resected cases, was 9–32%, which is higher than that of a benign diagnosis (9,12). However, resected cases are a selected group of the total population of the ND/UNS nodules, often operated because of worrisome US features. A reasonable extrapolation of the overall malignancy risk in this category is 5–10%, as stated in the new version of TBSRTC (17). This is the reason why close follow-up or even surgery is suggested for the 30% of all ND/UNS cases that are re-aspirated and that yield a second ND/UNS result, associated or not with suspicious US features. In case of one or more ND/UNS FNAC results, one can consider performing the FNA under US guidance followed by rapid on-site evaluation (ROSE). Another option is core biopsy, as recommended by other reporting systems for such non-diagnostic cases (19,20).
FAQ 4: When a Nodule Yields a ND/UNS Result, Can the Biopsy Be Repeated Rapidly, or Does a Three- to Six-Month Waiting Period Apply, as for AUS/FLUS Results?
For the cytopathologist, the three- to six-month waiting period before repeating the FNA after a ND/UNS result is justified by the presence of reparative and regenerative changes, which, if sampled during the second FNA, can lead to a false-positive cytological diagnosis. On the other hand, from the clinician's perspective, one can just repeat the biopsy without delay and perform a delayed third biopsy in case of a AUS/FLUS result on the second FNAC. This strategy will allow many patients to be reassured immediately and avoid three months of possible worry or even distress. Two studies have actually suggested that a three-month waiting period is not necessary for initially non-diagnostic aspirates (21,22). The same might be true for initially atypical aspirates (AUS/FLUS), but this particular question has not yet been addressed with sufficiently high numbers of cases (21). The ATA 2015 guidelines state that a waiting period is probably not necessary (12).
FAQ 5: When a Nodule Aspirated Under US Guidance Yields a Few Isolated Normal (Non-Atypical) Follicular Cells, Why Is It Classified as ND/UNS and Not as Benign?
The widespread use of FNA coupled with US allows the operator to be certain that the aspirated material indeed comes from the intended target lesion. However, even if the FNA practitioner is sure about which lesion has been sampled, this is not sufficient for the cytopathologist to establish a diagnosis of benignity based only on a few normal, non-atypical follicular cells. One of the major achievements of TBSRTC was that it addressed not only DCs but also quality issues, procedures, and standardization of reporting terminology. One of these topics concerns the specimen's adequacy. The assessment of pre-analytical issues, such as specimen adequacy, according to specific criteria, is the basis to ensure a high-quality result with a low false-negative rate, as well as to ensure that any downstream molecular test is applied on the appropriate target cell population.
In general, there is a minimum requirement of six groups of follicular cells, which should contain at least 10 thyrocytes each. These follicular cell groups should be well preserved, well stained, and not covered by blood cells that obscure their features (7). Of note, the cytopathologist cannot combine cells present in two or more ND/UNS results to try to meet the above criteria. The problem with isolated thyrocytes, even when they are present in a well-prepared and well-stained specimen coming from a nodule properly sampled under US guidance, is that they do not permit the cytopathologist to appreciate the architectural arrangement of the underlying lesion. It is thus impossible to establish whether the lesion is macrofollicular or microfollicular.
The clinician should also be aware of some exceptions to the above criteria. Some FNA aspirates may be diagnosed as benign, even without the presence of six groups of follicular cells with at least 10 thyrocytes each. This concerns aspirates from: (i) colloid nodules, which are extremely dilated follicles filled with colloid, producing a specimen composed entirely of colloid material; (ii) nodules with inflammation (typically in the context of autoimmune, infectious, or chronic inflammatory thyroid disease) where, in the presence of abundant colloid and abundant inflammatory cells, a few follicular cells are sufficient to diagnose the nodule as benign; and (iii) cystic nodules, where the typical cystic content (macrophages, hemosiderophages, red blood cells, fibrin, and colloid) should be classified in the ND/UNS DC. Nevertheless, in such cases, the clinician can treat the nodule as benign based on a clinicopathologic correlation with non-suspicious US imaging compatible with a pure cyst (often aspirated for volume reduction and/or symptomatic relief of compressive symptoms) (17).
Lastly, FNAC of developmental thyroid cysts can yield only cystic fluid, macrophages, and rare epithelial cells (mostly squamous) with a benign appearance. In such cases, a diagnosis of benignity consistent with a developmental cyst such as a thyroglossal duct cyst can be rendered cytologically. A clinicopathologic correlation should be encouraged.
FAQ 6: Why Is There Still a Residual Risk of Malignancy Associated with a Benign Classification?
Indeed, even if the FNA is performed under US guidance, and thus the clinician is sure about having sampled the correct target nodule, the ROM is not equal to zero. The reported ROM range taken from TBSRTC is 1–3%, while risk estimates reported in the literature vary between 1% and 10% and can be as high as 22% in nodules >3 cm (23). One possible explanation concerns cases with suboptimal preparation and staining that are incorrectly diagnosed as benign, even though they should have been classified as ND/UNS. In this respect, it is also important to note that although six clusters composed of 10 thyrocytes each qualify a specimen as adequate for diagnosis, more abundant material generally facilitates a more secure diagnosis and thereby contributes to minimize the ROM in this category. When samples are properly prepared and stained, discrepancies arise mostly due to errors in the interpretation of the cytological features, especially in the category of FV-PTC, where nuclear changes are subtle. If such features are not properly recognized, a false-negative diagnosis may be rendered. Finally, a rare caveat is the macrofollicular variant of FTC (24,25). These tumors show capsular and/or vascular invasion. Yet, the FNA yields primarily macrofollicles, and thus the lesion is classed as ND/UNS and not as FN/SFN, which is the case with the common FTC variant, where microfollicles are predominant. These caveats justify the management recommendation to perform at least one US follow-up examination of patients with a benign FNAC diagnosis.
FAQ 7: Are There Underlying Clinical Conditions That Favor Classification of Nodules as AUS/FLUS? If So, Might Informing the Cytopathologist Change the Diagnosis?
Some lesions are classified under the AUS/FLUS category because the specimen is qualitatively compromised. A badly smeared, fixed, or stained preparation is thus classified as AUS/FLUS because of technical reasons that do not depend on the nature of the lesion itself or any associated clinical conditions. For example, FNA on patients treated with anticoagulants can yield bloody aspirates. In this case, smears can be covered by blood that obscures the characteristics of the follicular cells and prevents their correct interpretation. In such a scenario, awareness of the anticoagulation treatment will not change the classification, as the issue is technical. In contrast, when the sample shows cytological atypia, it is of paramount importance that the cytopathologist has been informed of the patient's clinical conditions in order to correlate them correctly with the cytological findings. For example, antithyroid medications (thionamides) could be responsible for the presence of atypical thyrocytes with a so-called “flaming cytoplasm.” If such treatment is not disclosed by the clinician, the cytology might be inappropriately reported as atypical (AUS/FLUS or even FN/SFN).
Other important information to disclose to the cytopathologist is prior external beam radiation therapy or radioactive iodine therapy. Both can result in cellular enlargement and nuclear atypia that can lead to classification in the AUS/FLUS or SM DC (26).
Clinically evident cases of thyroiditis are occasionally subjected to FNA for diagnostic or research purposes. In cases of florid or sclerosing thyroiditis without a clearly identified nodule on US, slightly atypical nuclei (clearing of the chromatin, increased nuclear size, grooves) in an otherwise benign-appearing aspirate can be correctly interpreted as related to thyroiditis and thus classified as benign, avoiding repeat FNA or further interventions.
Because it is widely fibrotic, sclerosing thyroiditis may yield too few cells upon FNA. In such cases, the scanty cellularity can be considered worrisome in case of the presence of some atypical cells suggesting PTC. Indeed, slightly atypical nuclei with the same characteristics as in sclerosing thyroiditis can be observed in cases of PTC with desmoid-type fibromatosis, a rare PTC variant that presents with a well-defined nodule containing a hyperechoic zone on US consistent with sclerosis/fibrosis. Thus, the clinical context, including the US characteristics of the lesion, is critical to guide the interpretation of the cytological findings (27).
These examples illustrate how communication by the clinician of relevant clinical information to the cytopathologist is essential in order to interpret atypical cytological findings correctly. The clinicopathologic correlation can facilitate a correct interpretation of the observed atypia and thus guide the further clinical management of the patient. An exhaustive yet user-friendly requisition form can greatly help to ensure that the clinician does not omit any important clinical information that the cytopathologist could need (Table 1).
FAQ 8: For a AUS/FLUS Nodule, Is It Clinically Relevant to Explain the Specific Subcategory, the Reason for the Classification, and the Type of Cancer Possibly Associated?
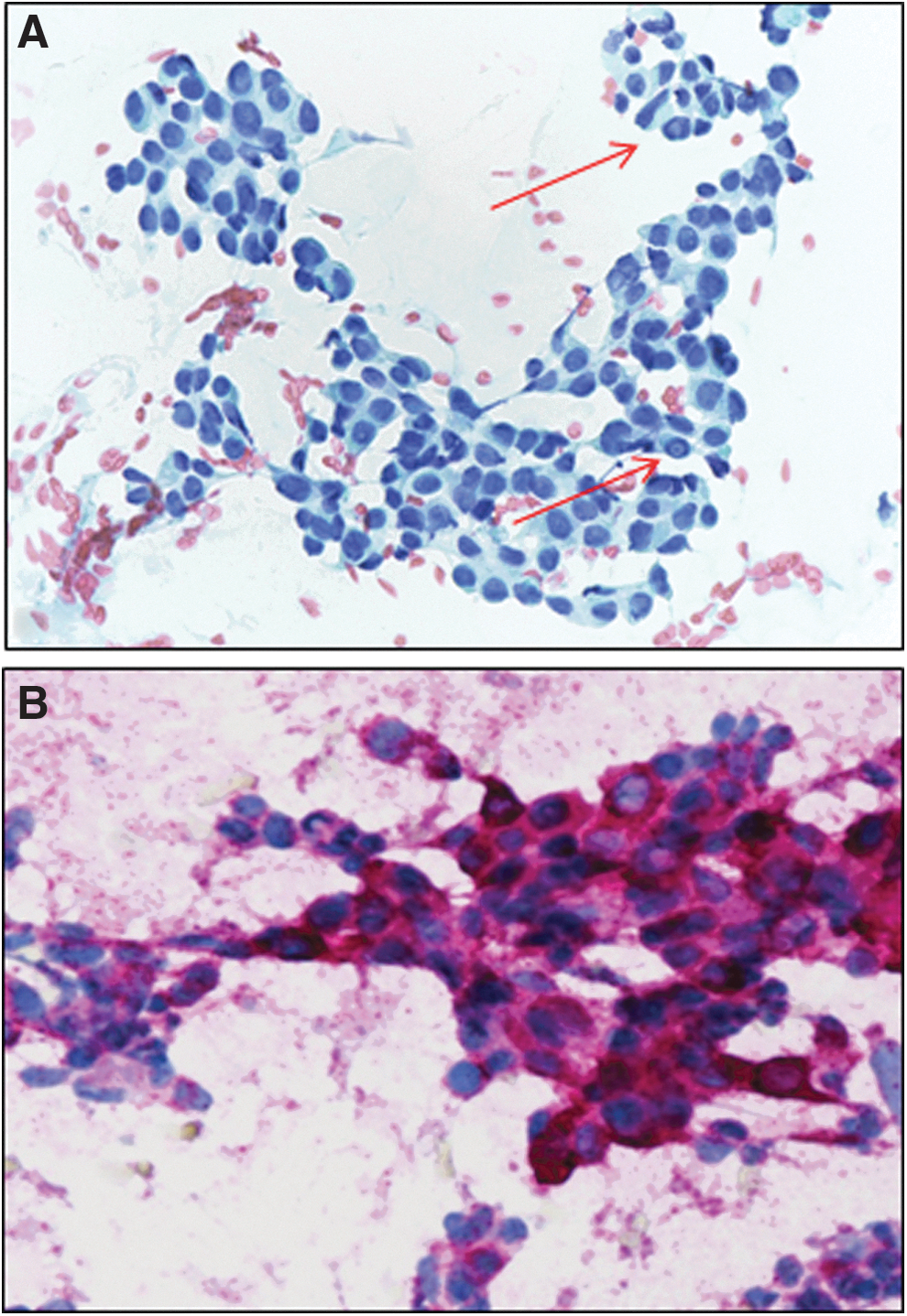
The AUS/FLUS DC comprises several scenarios with different associated ROM (28). In the new version of TBSRTC, the generic term AUS/FLUS is maintained, but it is suggested to add a note describing the pattern of the lesion among the most common patterns that have been identified in a large literature review (13). These patterns include nuclear atypia (i.e., the presence of features associated with PTC); architectural atypia (i.e., the presence of microfollicles suggesting follicular adenoma vs. follicular thyroid carcinoma [FTC]); oncocytic features (i.e., the presence of Hürthle cells with eosinophilic granular cytoplasm and prominent nucleoli); and “not otherwise specified” (NOS) in case the atypia observed cannot be classified in any of the aforementioned patterns. Among these four patterns, the malignancy risk decreases progressively from nuclear atypia (highest) to NOS (lowest). Knowledge of the precise ROM associated with the specific qualifier of a AUS/FLUS lesion can be very useful for the clinician who is charged to discuss repetition of the FNA with the patient and/or to propose alternatives. One such alternative can be molecular genetic testing, as also suggested by the ATA 2015 guidelines and the European Thyroid Association (ETA) 2017 guidelines (Fig. 1) (12,29). For example, without knowing the qualifier of the AUS/FLUS diagnosis, one might propose a molecular test for a AUS/FLUS case diagnosed as such because of quality issues (Fig. 2), which would be inappropriate. Moreover, in an effort to propose a personalized cytology, and in view of the paucity of material frequently observed in AUS/FLUS cases, the cytopathologist together with the clinician (as is the practice in our center) can also select the most appropriate molecular markers, such as mutational analysis of the BRAFV600E point mutation and RET/PTC rearrangements in cases with nuclear atypia, or the BRAFK601E , RAS point mutations, and PAX8/PPARγ rearrangement in cases with architectural atypia. The 2017 ETA guidelines provide a detailed discussion of the potential and limitations of molecular genetic testing (29).
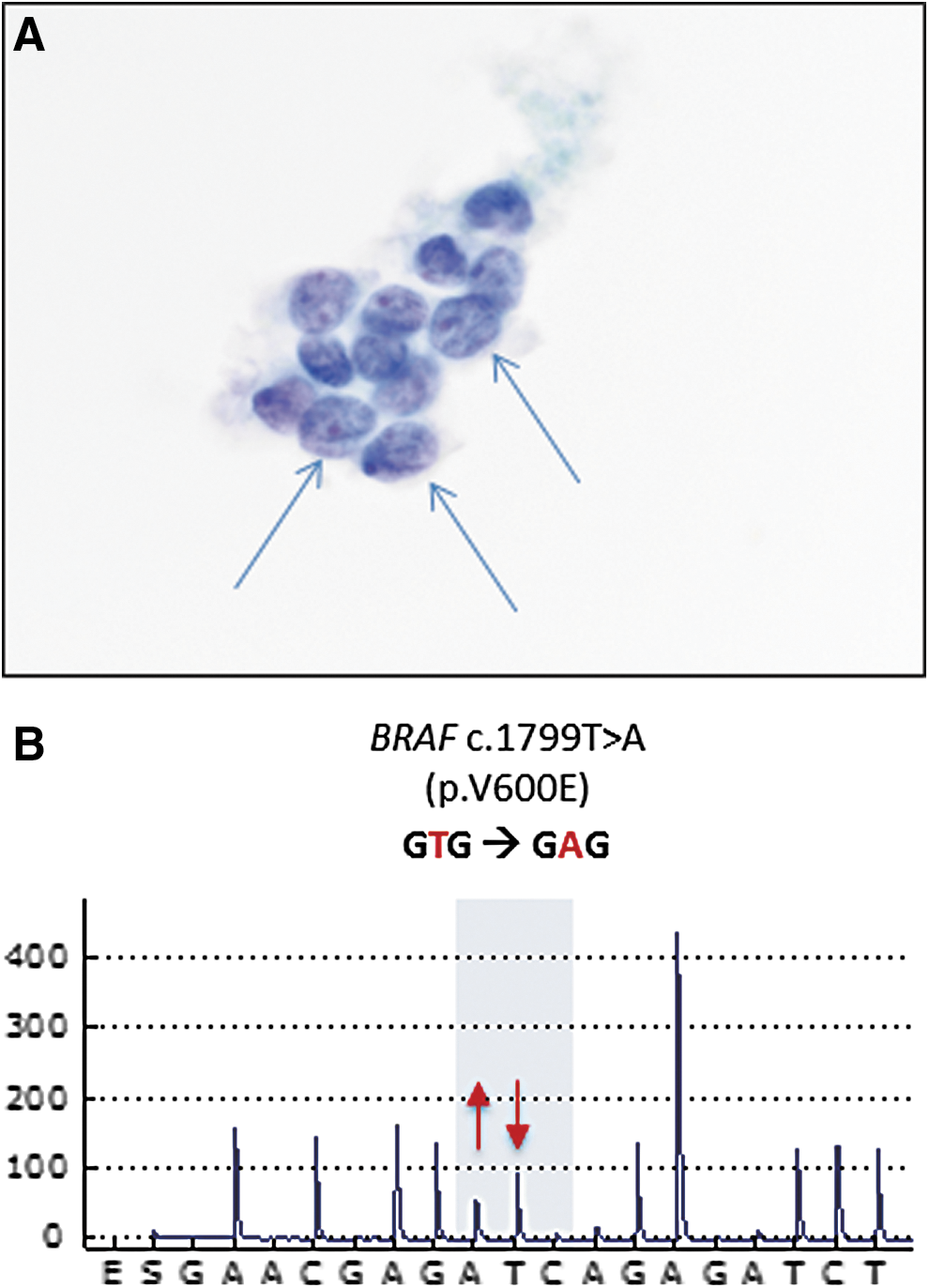
A classical variant of papillary thyroid carcinoma (PTC) initially classified as atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) and then diagnosed as malignant (M; PTC) via molecular genetic testing. A 25-year-old female with a 2.3 cm nodule in the left thyroid lobe underwent ultrasound (US)-guided fine-needle aspiration cytology (FNAC). (

A case of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) classified in the Bethesda AUS/FLUS and suspicious for malignancy (SM) diagnostic categories (DCs). A 52-year-old female with a 1.8 cm nodule located in the isthmus underwent US-guided FNAC. (
FAQ 9: When Will a Predominantly Microfollicular Lesion Be Classified as AUS/FLUS and When as FN/SFN?
Predominance of microfollicles can be observed in case of a paucicellular aspirate or in case of a highly cellular aspirate. In the first situation, the appropriate diagnosis would be “AUS/FLUS, architectural atypia.” The cytopathologist is reluctant to induce a diagnostic lobectomy in these cases and prefers to have the patient undergo a repeat FNA in the hope of obtaining more material that will allow a more accurate diagnosis to be reached. In the second situation, a highly cellular aspirate with predominance of microfollicles, the appropriate diagnosis would be FN/SFN. What is still not clearly defined is the minimum amount of microfollicles necessary for a FN/SFN diagnosis. Also, it is important to remember that slight nuclear atypia is now included in the FN/SFN DC. In fact, in the presence of a microfollicular pattern with nuclear atypia, it is also possible that the lesion is a NIFTP (which can only be diagnosed on surgical pathology), as already mentioned in FAQ 1.
FAQ 10: Can a FN/SFN Nodule Be PTC?
In the FN/SFN DC (10–40% ROM) are usually classified lesions that contain a predominant or exclusive population of microfollicles. When such lesions are subjected to diagnostic surgery (normally lobectomy), the main histological correlates of these aspirates are benign proliferations, namely hyperplasic nodules/follicular adenomas, and in a lower proportion malignant lesions, namely FTC (9,13). Some malignant cases corresponded in the past to FV-PTC. This variant is characterized by a microfollicular structure and subtle nuclear changes in the sense of PTC, namely nuclear clearing and grooves, with few or no nuclear inclusions. These subtle nuclear changes can often pass unnoticed, leading to a FN/SFN diagnosis of these lesions (30,31). With the modification in the nomenclature and the introduction of NIFTP as a lesion of low malignant potential, fewer PTC cases will be found in the FN/SFN diagnostic category, thus reducing the lower end of the ROM of the FN/SFN DC (32,33). Notwithstanding this improvement in the diagnostic classification, some invasive FV-PTC still will be diagnosed in the FN/SFN DC because the presence or absence of capsular or vascular invasion cannot be assessed on cytological material.
FAQ 11: Can a SM Nodule Be Something Other Than PTC?
In the majority of cases, a SM nodule turns out to be PTC upon histological examination. In this DC are classified cases that contain atypical nuclear features suspicious for PTC (either the classical or the follicular variant), but that are not sufficient for a conclusive diagnosis of PTC. However, the degree of suspicion is higher than that of the cytological atypia component in the AUS/FLUS DC (cf. FAQ 8). As a consequence, surgery is indicated (cf. FAQ 16). Nuclear atypia, in particular nuclear pseudoinclusions, are not seen exclusively in PTC but also sometimes in medullary thyroid carcinoma (MTC), along with salt-and-pepper chromatin, granular cytoplasm, and absence of colloid. MTC is actually the second most frequent histological diagnosis in case of SM cytological findings (when all the above characteristics of MTC are not present). Other types of tumors that can be suspected on cytology and confirmed on histology include trabecular adenoma, poorly differentiated thyroid carcinoma (PDTC), anaplastic thyroid carcinoma (ATC), lymphoma, sarcoma, and metastases of extrathyroidal primary tumors. A good percentage of NIFTP also fall in this DC, which is why the ROM of an SM classification decreases substantially when NIFTP is not considered a cancerous lesion (7,13,32,33).
FAQ 12: What Is the Major Cytological Difference Between the SM and M DCs?
The main difference between the SM and M DCs is that in the former, the cytological criteria for malignancy are not completely met, yet the level of suspicion is high. Histologically proven FTCs are typically not found in the SM or M DCs. This is because the criteria for malignancy in follicular lesions are histological, requiring examination of the tumor's capsule and of the vessels in the capsule. Therefore, these tumors cannot be diagnosed purely on cytological grounds. Except for FTC, which, as mentioned, is typically not classified in the SM DC, all other types of thyroid carcinoma may be classified in this DC based on a preoperative FNAC if the cytological criteria present are not sufficient to warrant a confident diagnosis of malignancy. Among epithelial tumors, MTC, PDTC, or ATC can be classified in the SM DC, but the most frequent type by far is PTC. For PTC, SM designation is usually reached in cases with limited material and/or when some of the following features are missing: pseudoinclusions, psammoma bodies, papillary structures, nuclear membrane irregularity, and nuclear grooves. In such a scenario, when a microfollicular pattern is present, there is a highly probability that the lesion is FV-PTC, but the cytopathologist cannot be totally certain.
FAQ 13: In Which TBSRTC DC Would a NIFTP Be Classified?
Even though a diagnosis of NIFTP can only be made on surgical pathology, it is interesting to consider the spectrum of possible presurgical cytological diagnoses associated with these lesions. It has been shown that histologically proven NIFTP had been classified preoperatively in mainly three DCs—AUS/FLUS, FN/SFN, and SM—with frequencies that were variable among different centers (32,33). As for any other lesion, a lesion later shown to be a NIFTP may be classified preoperatively in the ND/UNS category, when the material is insufficient. Beyond that, the precise DC into which a specific lesion later proven to be a NIFTP may be classified on presurgical cytology depends on various factors, including the degree of nuclear atypia, the extent of microfollicular architecture, the quality of the specimen, and, last but not least, the experience of the cytopathologist. A pathology-proven NIFTP should normally not have been classified as a benign lesion on cytology because the presence of atypia and/or microfollicles warrants classification in a DC with higher ROM. It should also typically not have been classified as a malignant lesion because papillary structures are absent, the degree of nuclear atypia is milder, and the presence or absence of capsular and vascular invasion cannot be assessed on cytological material. Nevertheless, the risk of the M DC also decreased slightly after the introduction of NIFTP (from 97–99% to 94–96%) (15), indicating that a small number of nodules ultimately shown to be NIFTP do end up in the M DC based on FNAC.
From a presurgical point of view, given that NIFTP is considered a lesion with a low malignant potential, the most important consequence of renaming noninvasive encapsulated FV-PTC into NIFTP is that it resulted in a decrease of the ROM of the aforementioned DCs (AUS/FLUS, FN/SFN, and SM). Among multicentric studies, the corresponding reduction of the ROM varied greatly (33). For this reason, the new Bethesda version provides a range for the ROM taking into account the new nomenclature (Table 2). Because the introduction of NIFTP is quite recent and not yet ubiquitously accepted, the new Bethesda version cites two ROM ranges for each DC: a higher one for when NIFTP is considered a cancerous lesion (not shown) and a lower one when it is considered a lesion with low malignant potential (Table 2). Admittedly, if one subscribes to the NIFTP concept, then only the respective lower ROM ranges are relevant.
Adapted from Cibas and Ali (7).
DC, diagnostic category; ROM, risk of malignancy; TBSRTC, The Bethesda System for Reporting Thyroid Cytopathology; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; FNA, fine-needle aspiration.
FAQ 14: Which Signs Raise Suspicion of MTC, and in Which DC Is an MTC Likely To Be Classified?
Depending on the suspicious features present in each particular case, MTC is usually diagnosed in the SM or M DC. The most striking cytological features suggestive of MTC are the absence of colloid and the presence of a salt-and-pepper chromatin and of a granular eosinophilic cytoplasm. Presence of nuclear pseudoinclusions does not exclude a diagnosis of MTC, as MTC can indeed also present with abundant nuclear pseudoinclusions (Fig. 3). MTC is in fact considered a great mimicker, as it can assume the most disparate cytological features, such as spindle cells or oncocytic cells. This can occasionally lead to classification in the SM DC as suspicious for PTC, or in the M DC as PTC or even as sarcoma or metastatic disease. In cases where MTC is suspected based on clinical features or based on cytological findings of ROSE at the time of FNA sampling, then collection of material for cell block can allow for immunocytochemical staining for calcitonin, confirming the diagnosis if cytomorphology alone does not allow for a definitive diagnosis. Measurement of calcitonin (which should be high in MTC) and possibly also thyroglobulin (which should be low or undetectable) in the needle washout is also very helpful in such cases.
A case of medullary thyroid carcinoma (MTC) correctly classified in the M DC and confirmed as a neuroendocrine tumor using immunocytochemistry. (
FAQ 15: When a Suspicious Lymph Node Is Aspirated in the Context of a Coexisting Thyroid Nodule, How Relevant Is It for the Cytopathologist That the Nodule Also Be Aspirated?
Strictly speaking, it is not necessary because in general, the cytological diagnosis of the lymph node is independent from that of the thyroid nodule. In rare cases when there are some atypical cells in the FNAC of the lymph node that are suspicious for PTC, an ancillary study, such as immunostaining for thyroglobulin or TTF-1, if positive, can confirm the presence of metastatic PTC. Finally, measuring thyroglobulin in the needle washout of the FNA sample can confirm metastatic disease when there is paucity or lack of tumor cells in the specimen and an immunohistochemical staining cannot be performed. Because this is obviously not known beforehand, routine measurement of thyroglobulin in the aspirate (or at least conservation of an appropriate sample for later measurement if necessary) should be strongly considered.
As a general point, if a thyroid nodule is suspicious and warrants FNA, it is overall logical to biopsy it at the same time as the suspicious lymph node because otherwise, if the lymph node FNA is negative, then the question about the nature of the thyroid nodule would remain and the patient would need to return for FNA of the thyroid nodule. On the other hand, if a lymph node is highly suspicious on US and the thyroid contains multiple nodules of which none is highly suspicious, it may be reasonable to perform FNA only on the lymph node, which will be sufficient to guide further management if the result confirms metastasis of thyroid carcinoma, given that total thyroidectomy with compartment-based lymph node dissection is indicated in such cases.
FAQ 16: In Which Cases Is a Frozen Section Useful to Guide Surgical Management?
Given the high risk of malignancy in SM cases, surgery is normally warranted with a diagnostic and therapeutic intent. If there is a dilemma between total thyroidectomy and initial diagnostic lobectomy (if indicated with completion surgery in case of malignancy confirmed on histology), then preoperative confirmation of malignancy may also be achieved by molecular genetic testing, in particular by detecting alterations associated with PTC with very high positive predictive value, such as a BRAFV600E mutation or a RET/PTC rearrangement. Alternatively, or for cases where molecular genetic testing results do not confirm malignancy, a frozen section analysis during diagnostic lobectomy may provide perioperative confirmation of malignancy in some cases. This depends largely upon the recognition of typical features of classical PTC, notably papillary structures and severe nuclear atypia. There are two main limitations. The first is that the quality of the specimen obtained during a frozen section is lower than that obtained during routine histopathological examination. Thus, among lesions classified in the SM DC that are finally proven to be classical PTC cases on histology, not all could be confirmed as such on frozen section analysis. The second limitation is that the single frozen section obtained may not be representative of the lesion as a whole. Therefore, follicular patterned lesions are inappropriate candidates for frozen section analysis because even in cases of invasive FV-PTC or FTC, the likelihood of detecting capsular or vascular invasion in a single frozen section is exceedingly low.
Conclusions
Although there are no formal studies on this topic, close communication between the cytopathologist and the clinician can help to optimize the diagnostic accuracy of thyroid FNAC. In the authors' experience, good ways to interact constructively and to develop a deeper mutual understanding of the intricacies and challenges of each other's discipline include joint US–FNA clinics with ROSE for selected nodules, multidisciplinary tumor boards, clinicopathologic discussions of cases in the cytopathology unit while studying the slides of typical and atypical cases under a multi-observer microscope, as well as dedicated combined workshops and practical courses. It is hoped that the present overview will serve as an additional resource to this end.
Footnotes
Acknowledgments
G.P.S. is partly supported by a Leenaards Foundation Fellowship for Academic Promotion in Clinical Medicine.
Author Disclosure Statement
No competing financial interests exist.