
Abstract
Background:
Anaplastic thyroid cancer (ATC) is an aggressive and highly lethal disease with poor outcomes and resistance to therapy. Despite multimodality treatment, including radiation therapy and chemotherapy, response rates remain <15%, with a median time to progression of less than three months. Recent advances in radiotherapy (RT) delivery and gene-expression profiling may help guide patient selection for personalized therapy. The purpose of this study was to characterize the response to radiation in a panel of ATC cell lines and to test alternative RT fractionation schedules for overcoming radioresistance.
Materials and Methods:
The cellular response to radiation was characterized based on clonogenic assays. Radiation response was correlated with microarray gene-expression data. Hypofractionated and conventional RT was tested in an orthotopic ATC tumor model, and tumor growth was assayed locally and distantly with in vivo and ex vivo bioluminescence imaging.
Results:
A spectrum of radiosensitivities was observed in ATC cell lines. Radioresistant cell lines had higher levels of CXCR4 compared to radiosensitive cell lines. Compared to conventionally fractionated RT, hypofractionated RT resulted in significantly improved tumor growth delay, decreased regional and distant metastases, and improved overall survival.
Conclusions:
The findings demonstrate the heterogeneity of response to radiation in ATC tumors and the superiority of hypofractionated RT in improving local control, metastatic spread, and survival in preclinical models. These data support the design of clinical trials targeting radioresistant pathways in combination with hypofractionated RT.
Introduction
A
This study investigated the radiosensitivity and genomic profile of eight different ATC cell lines, and tested the response to HF RT in a novel orthotopic model of highly radioresistant ATC compared to CF. The data highlight the variability in response to radiation based on genetic profile. Importantly, the data demonstrate that HF RT is superior to CF in limiting tumor growth. These data provides proof of concept, supporting currently ongoing Phase I clinical trials combining HF RT with immunotherapy (NCT03122496).
Materials and Methods
National Cancer Data Base analysis
The de-identified National Cancer Data Base (NCDB) was utilized for this study. The NCDB collects data from >1500 community and academic cancer centers and has been reported to represent about 70% of all cancer cases in the United States. The de-identified NCDB file was queried for all patients with ATC diagnosed between 2004 and 2013 based on primary site code C739, grade 4 classification, and histology code 8021. Only patients with reported follow-up were included, and patients with more than two lifetime neoplasms were excluded. The analysis was limited to patients with no known distant metastases in order to focus on the cohort of patients who would be candidates for local therapy. For assessment of radiation fractionation patterns, only patients treated to the primary tumor site were selected utilizing the “RAD_TREAT_VOL” category. For the purposes of this analysis, CF was defined as 150–249 cGy per fraction, and HF was defined as 250 cGy per fraction or higher. Palliative regimens were defined as BED10 < 50 Gy and were excluded.
Cell lines and cell culture
Eight cell lines comprising seven ATC (8505C, C643, CAL62, KHM-5M, KTC-2, SW1736, and T238) and one papillary thyroid carcinoma (PTC; BCPAP) were used in this study. All cell lines were cultured in RPMI 1640 + 5% fetal bovine serum (FBS) at 37°C in 5% CO2 in humidified air, with the exception for two cell lines: T238 and T351. These two cell lines were cultured with RPMI 1640 + 10% FBS at 37°C in 5% CO2 in humidified air. All cell culture media was supplemented with antibiotic–antimycotic agent (Thermo Fisher Scientific, Waltham, MA). Cell lines were confirmed to be mycoplasma free prior to commencing experiments. All cell lines used in the study underwent short tandem repeat analysis within six months of commencing experiments.
Clonogenic assay and cell irradiation
To determine radiosensitivity, clonogenic assays were performed. Cells were grown in cell culture to 70% confluence, in which they were harvested and counted with TC20™ Automated Cell Counter (Bio-Rad Laboratories, Hercules, CA). Cells were seeded into six-well plates at appropriate seeding densities. Cells were irradiated 24 hours after seeding with the RS 2000 X-ray irradiator (Rad Source Technologies, Inc., Buford, GA) containing a 3 mm copper filter at a rate of 1.24 Gy/min. Colonies were allowed to form for 8–10 days post irradiation, after which they were stained with 0.5% crystal violet in methanol solution. Colonies containing >50 cells were counted with the assistance of a microscope. Only colonies with >50 cells were counted. Each experiment involved three technical replicates. Data shown are the average of three to four independent experiments for each cell line. The surviving fraction was determined by dividing the number of colonies by the number of cells plated, with a correction for plating efficiency. Data were plotted on semi-log graphs and fitted using the linear-quadratic (LQ) model (25).
Gene expression analysis
A previously unpublished microarray gene-expression data set from the authors' institution was interrogated on all cell lines used in this study. Transcriptome-wide gene expression data for thyroid cancer cell lines were generated using Affymetrix Human Genome U133 Plus 2.0 microarrays. Quality control was performed using the arrayQualityMetrics package from Bioconductor 3.5 in R (26). Outliers were detected using between-array comparisons and MA plots and by analyzing array intensity distributions. Fifty-six microarray profiles passed quality control and were used for downstream analysis. Background subtraction and quantile normalization were performed with Affymetrix Power Tools (
Orthotopic thyroid cancer murine model
The methodology for orthotopic murine model for thyroid cancer has been well characterized previously by Morrison et al. (28). Briefly, the 8505C cell line was previously stably transfected with pEGFP-Luc-N1 plasmid (Clontech, Mountain View, CA) and maintained in cell culture with G418 prior to orthotopic implantation into athymic nude mice (Envigo, Huntingdon, United Kingdom). 8505C cells (500,000) were suspended in 5 μL of serum-free media and injected into the right thyroid lobe of athymic mice under the guidance of a surgical microscope. Mice were monitored twice weekly, and any mice showing signs of morbidity, including, rapid weight loss, lethargy, and difficulty breathing, were euthanized according to the institutional policy on humane endpoints in animal research. All animal experiments were performed under an approved institutional animal care and use committee protocol at the University of Colorado Denver (protocol # 108515[06]1E).
Imaging
For monitoring tumor growth, animals were injected with D-luciferin (100 mg/kg in 100 μL of phosphate-buffered saline). Approximately 10 minutes later, mice were anesthetized and submitted to bioluminescence imaging (BLI) using a Xenogen IVIS Imaging System 200 Series (PerkinElmer, Inc., Waltham, MA). Total BLI was measured for durations of 0.5, 1, 5, 10, and 30 seconds in units of photons per second using Living Image software (PerkinElmer, Inc.). BLI was performed twice in the first week and weekly thereafter. Ex vivo BLI of organs at sacrifice was performed by immersing the organ in D-luciferin (300 μg/mL) for 10 minutes and imaging at 0.25, 1, 4 and 16 seconds of exposure time.
Small-animal image-guided irradiation
Irradiation was delivered using X-RAD SmART Image Guided Irradiator (Precision X-Ray, North Branford, CT). Mice were anesthetized with isoflurane, and a computed tomography (CT) scan was acquired for treatment planning using SmART Plan software. The tumor-bearing thyroid was contoured based on anatomical and bony landmarks. Two wedge-pair beams using a 10 mm square cone were applied. In all cases, the thyroid received 95–105% of the total dose (Supplementary Fig. S1; Supplementary Data are available online at
Statistics
For survival analysis, Kaplan–Meir curves were analyzed based on the log-rank (Mantel–Cox) test for comparison of all groups. Hazard ratios were generated between pairs of groups. For assessment of tumor growth differences, two-way analysis of variance was performed. All analyses were performed in GraphPad Prism v6 (GraphPad Software, Inc., La Jolla, CA).
Results
The majority of ATC patients fail CF RT
The NCDB was interrogated to assess the survival profiles and patterns of care for ATC patients registered in the 2004–2013 data set. Of the 2127 patients identified as having ATC, only patients with non-metastatic disease (n = 1070) were selected for overall survival analysis (Fig. 1A). The median survival for this cohort was 4.9 months (Fig. 1B). A cohort of ATC patients with known radiation doses was highlighted, and it was observed that 91% of the 325 patients received CF (150–249 cGy per fraction) compared to the remaining 9% who received higher does per fraction (≥250 cGy per fraction; Fig. 1A). While overall survival modestly improved in recent years, median survival remains exceptionally poor, with the majority of patients receiving CF RT.
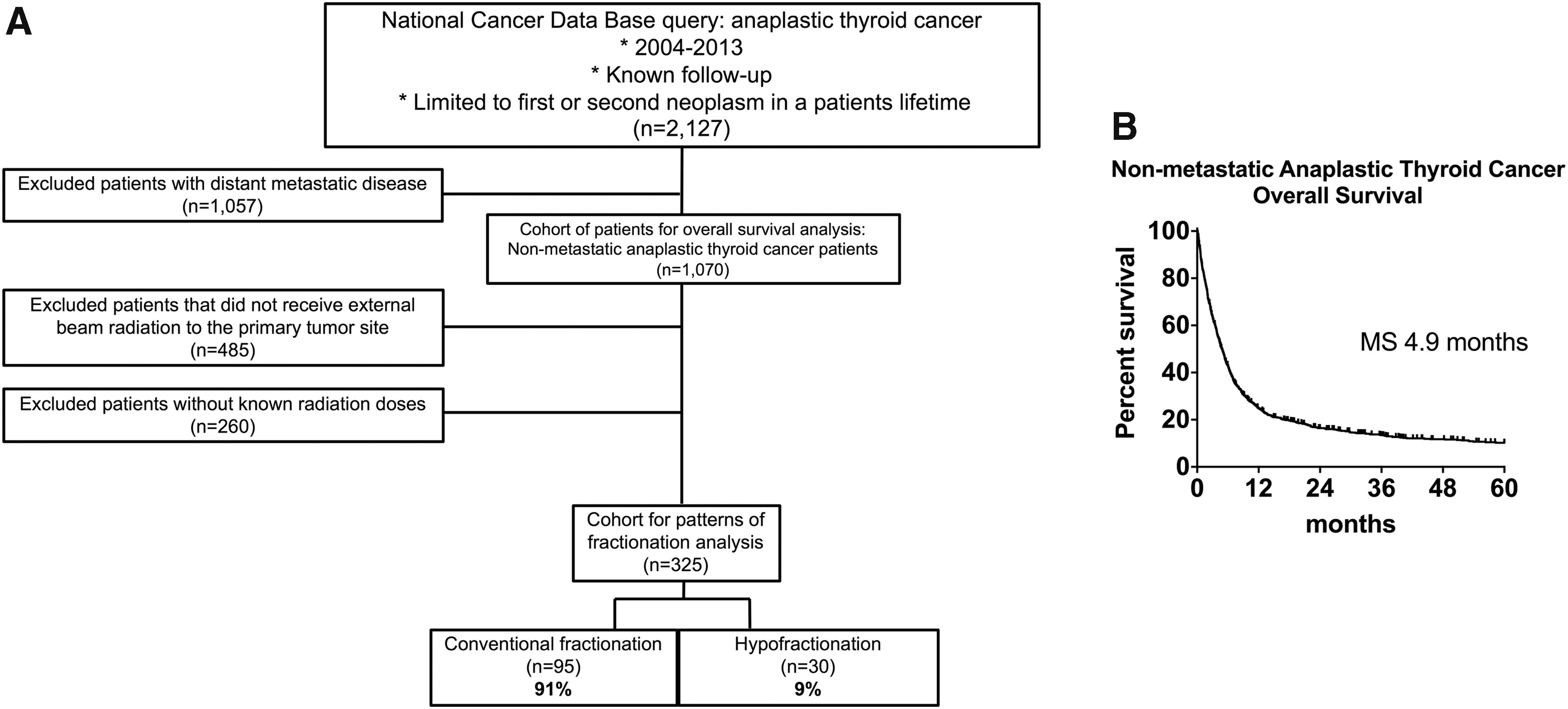
Analysis of overall survival in anaplastic thyroid carcinoma (ATC) patients based on the National Cancer Data Base. (
ATC cell lines display a range of radiosensitivities in vitro
The intrinsic radiosensitivity of seven ATC cell lines and one PTC cell line was characterized by clonogenic assay. Figure 2A displays the survival profiles of each cell line fitted to the linear quadratic model. SF2 values ranged from 0.15 to 0.55 (Fig. 2B). The cell lines were categorized into two groups—radioresistant (RR) or radiosensitive (RS)—on the basis of determined SF2 values. Five of the eight cell lines (KHM-5M, 8505C, Cal62, KTC-2, and T238) were categorized as RR, with an average SF2 of 0.45 ± 0.03, compared to the remaining three cell lines (SW1736, BCPAP, and C643), with an average SF2 of 0.18 ± 0.02 (Fig. 2B and C). Cell lines categorized as RR had significantly higher SF2 compared to RS cell lines (Fig. 2B). Notably, radiosensitivity was independent of mutational status (Fig. 2C).

Response of human ATC cell lines to radiation. (
HF RT enhances tumor control and survival compared to CF RT in a novel orthotopic murine model of radioresistant ATC
The effect of HF versus CF was investigated in a novel orthotopic murine model of ATC, which the authors previously established (28). The radioresistant 8505C cell line was employed for this study, which is known to grow orthotopically and metastasize to distant sites and regional lymph nodes (29). A total dose of 20 Gy in two fractions (one week apart) was delivered to the HF group, and the same dose in 10 fractions was delivered to the CF group (five days/week schedule; Fig. 3A).
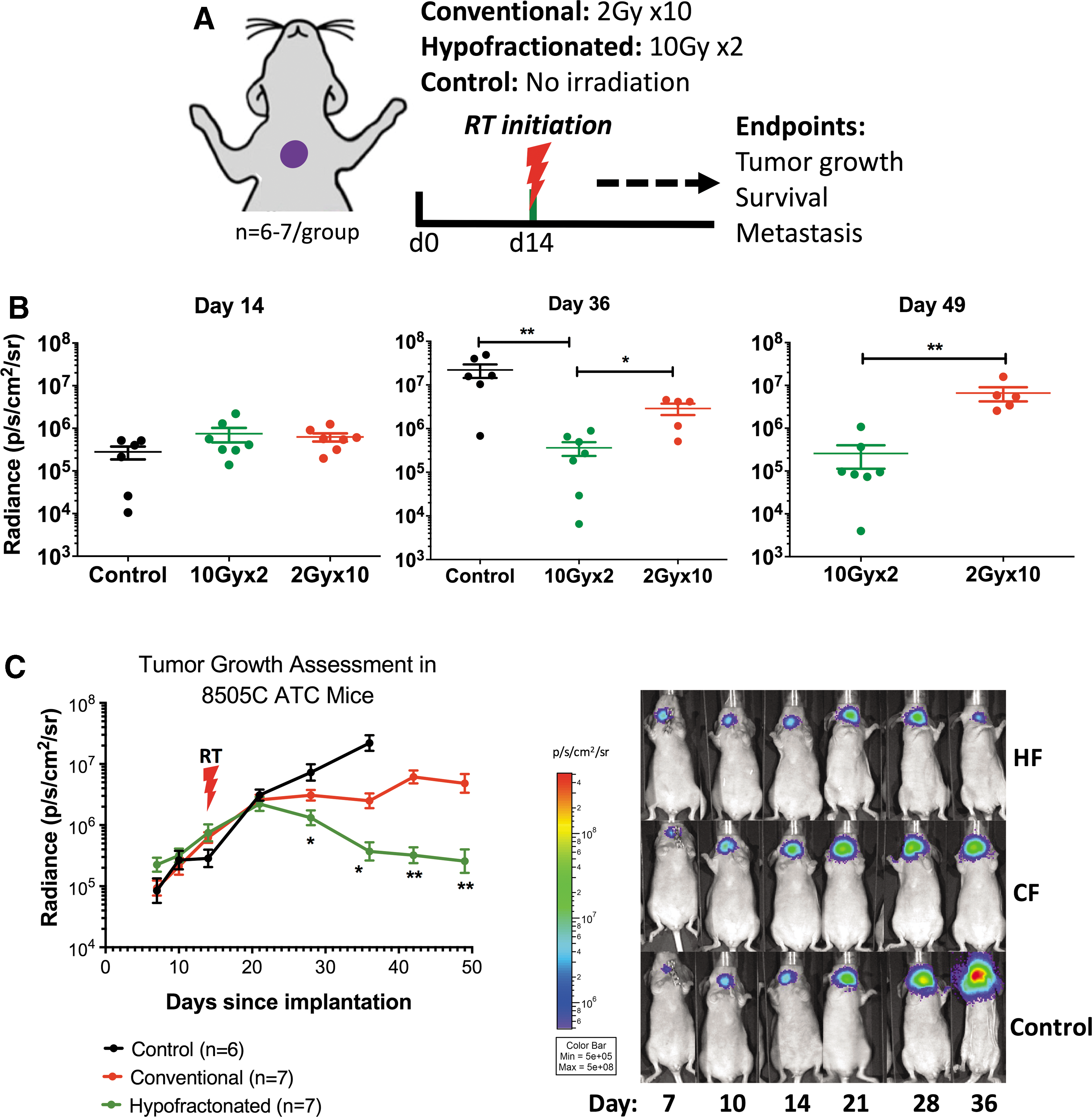
Response of orthotopic 8505C tumors to radiotherapy. (
Mice were divided into groups on the day of treatment initiation (day 14) based on BLI photon radiance signal. Mice in all the groups had comparable average photon radiance on the day of treatment initiation (Fig. 3B). Longitudinal analysis of weekly BLI revealed significant differences in local tumor growth delay in the HF group compared to the control and CF groups (Fig. 3C). On the last day in which all mice were alive (day 36), average photon radiance in the HF group was significantly lower compared to mice in the control group (51.8-fold decrease; p = 0.0097) and mice in the CF group (6.7-fold decrease; p = 0.0057; Fig. 3B). Mice in the HF group continued to have a decreased signal arising from the primary tumor over time, while mice in the CF group had an increased signal. By day 49, on which all mice from the HF and CF groups were alive, average photon radiance was significantly lower in the HF group compared to the CF group (18.8-fold decrease; p = 0.0094; Fig. 3B and C). In addition to its effect on local control, HF resulted in significantly improved survival compared to mice in the control and CF groups, which had a median survival of 55 and 65 days, respectively (Fig. 4A). Median survival for the HF group was not reached at the termination of this study (day 78 post tumor inoculation). Only two mice in the HF group were euthanized due to local failure. The remaining mice in the HF group were euthanized on day 78 for assessment of metastasis. Distant metastatic spread was assessed with BLI of organs immediately after mouse euthanasia. When lung metastases were observed on BLI, their presence was further validated by analyzing CT images acquired within the same week prior to mouse euthanasia (Supplementary Fig. S2). The results demonstrate a significant decrease in the number of lung metastases in the HF group compared to the control and CF groups (p < 0.0001 for both; Fig. 4B). In addition, metastases were not observed in regional lymph nodes or other distant organs, including the adrenal glands, liver, spleen, chest wall, and brain in mice that received HF RT (Fig. 4C). There was no difference in regional nodal or distant metastases between the CF group and the control group (Fig. 4C). No radiation-induced toxicity, such as weight loss or skin ulcerations, was observed in mice that received either HF or CF. Taken together, the data demonstrate superior outcomes on local control, distant metastasis, and overall survival with an equivalent total dose delivered in a HF regimen.
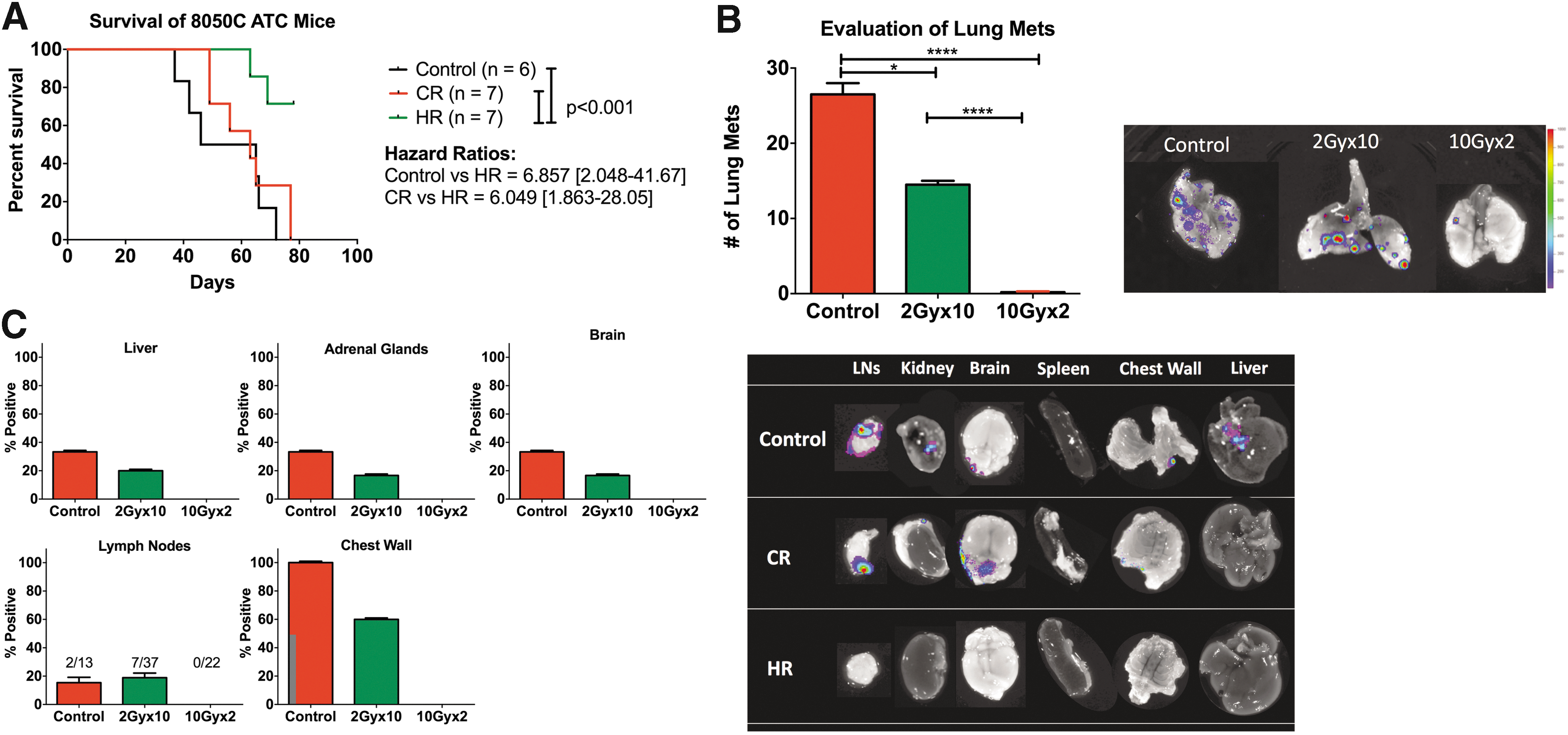
Assessment of survival and metastatic spread in orthotopically implanted 8505C ATC tumors. (
Genomic characterization of ATCs reveals markers associated with radioresistance
To identify novel targets for radiosensitization, gene-expression analysis was performed on the eight ATC cell lines, including 8505C. A classification of either radiosensitive (RS) or radioresistant (RR) was applied according to the SF2 values determined in Figure 2. To focus the investigation, the analysis was limited to gene-expression changes of ≥1.7-fold (Fig. 5). A set of 15 genes were identified as significantly differentially regulated between RR and RS cell lines (Fig. 5). Of the 15 genes, 11 were downregulated in RR cell lines, and four were upregulated relative to RS cell lines. Of these genes, CXCR4 was the most differentially expressed gene between the RR and RS cell lines. CXCR4 has been shown to play a role in mediating tumor growth, metastasis, and resistance to therapy, and its targeting has shown efficacy in various tumor animal models (30 –32).
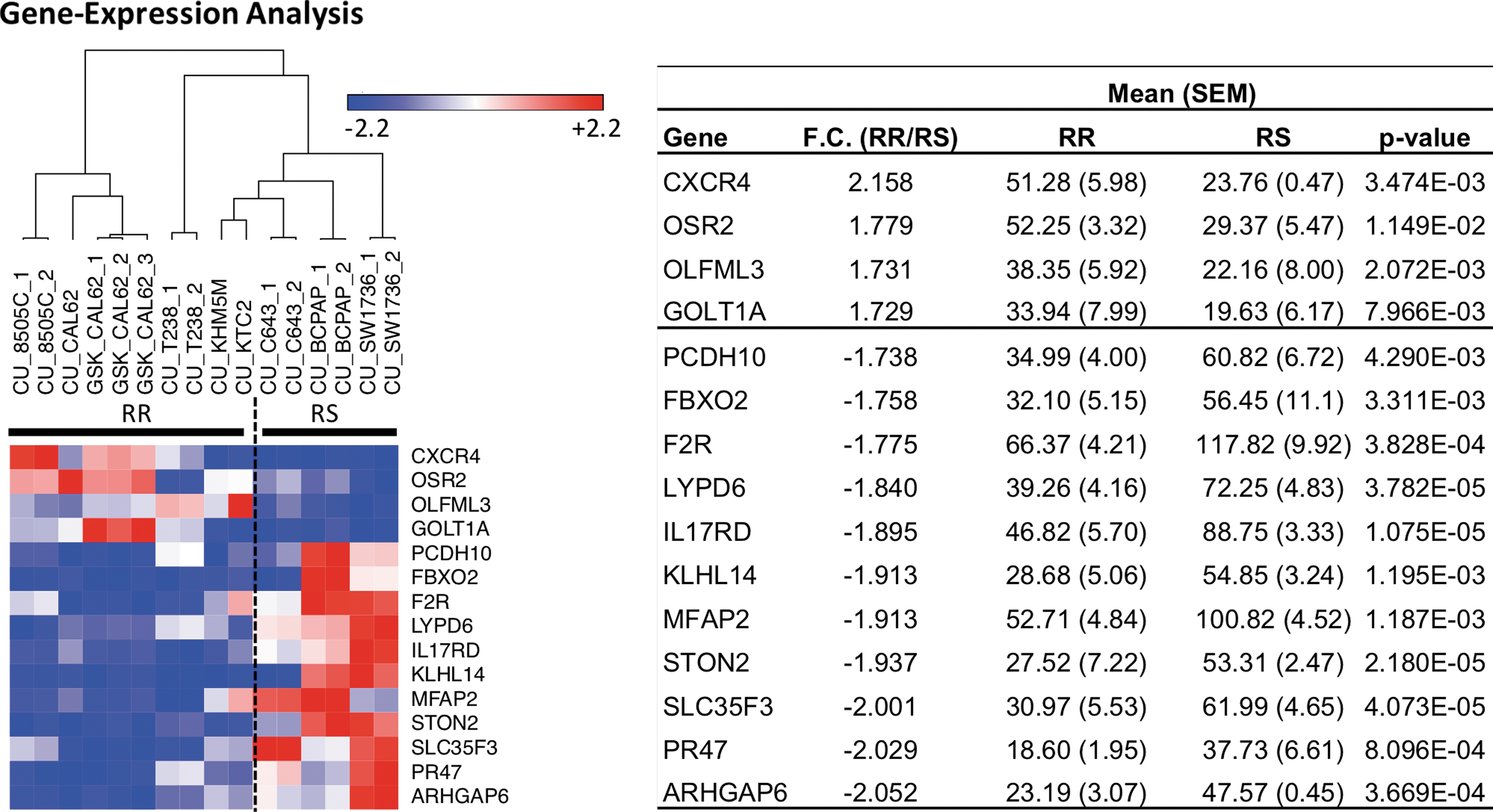
Genomic characterization using Affymetrix microarrays of eight ATC cell lines. A cutoff of 1.7-fold change between radioresistant (RR) and radiosensitive (RS) cell lines was used. The coefficient of variance was set to 0.2, and only genes that were significantly modulated were included in the analysis. Heat map shows hierarchical clustering of RR and RS cell lines. Table summarizes genes that are significantly modulated between RS and RS cell lines. Significance was determined using an unpaired t-test with a false discover rate <1%. Color images available online at
Discussion
Guidelines and treatment approaches for ATC have not drastically changed within the last decade, despite dismal outcomes (3,4). The ATA continues to recommend the use of a multimodality approach, consisting of surgery, chemotherapy, and RT (8). Recent innovative technologies in RT delivery have allowed for an increasing degree of treatment personalization through improved imaging and targeting of tumors. Technologies such as stereotactic body radiation therapy (SBRT) and intensity-modulated radiation therapy have high accuracy and precision, allowing for higher doses of irradiation to be delivered to the tumor while minimizing normal tissue toxicity (33,34). In the setting of locally recurrent head and neck cancer where SBRT is more frequently employed, it has been proven to be safe and effective when evaluated at time points that exceed the median survival of ATC patients (35).
This study characterized the relative radiosensitivities of a panel of human ATC cell lines and tested the efficacy of a HF RT regimen in a highly radio-resistant orthotopic ATC tumor model. To the authors' knowledge, this is the first study examining radiogenomic profiles of ATC cell lines. A previous study by Sambade et al., in a large panel of melanoma cell lines, observed a wide range of radiosensitivity profiles that did not significantly correlate with B-Raf mutation status (36). Similarly, a correlation between B-Raf mutation and radioresistance was not observed in the present study.
There are currently no preclinical or clinical studies comparing the efficacy of HF RT with CF RT in ATC tumors. This study utilized a novel orthotopic murine model of ATC to compare outcomes between mice receiving CF and HF RT regimens. The 8505C cell line was chose, as this cell line has been shown to be radioresistant (37). Superior local tumor control was demonstrated in mice receiving a HF dose of 2 × 10 Gy spaced one week apart compared to mice treated with an equivalent dose in daily fractions of 2 Gy. These findings are consistent with other preclinical mouse models of cancer demonstrating beneficial outcomes after HF RT (38,39). In comparing fractionation schedules, a decision was made to keep the total dose constant and to alter the dose per fraction. Although the total dose is the same, the biologically equivalent dose (BED) is drastically higher if the LQ model is applied. The BED is a measure of the true biological dose delivered through a defined number of fractions for a defined total dose. The BED for 20 Gy in two fractions is 40 Gy compared to 24 Gy when delivered with 2 Gy fractions (α/β = 10). However, the applicability of the LQ model at doses >8 Gy per fraction has been controversial (40). In addition, clinical trials assessing the efficacy of HF RT have generally used total doses similar to CF RT. For example, RTOG 0618 investigated the efficacy of 60 Gy in three fractions delivered over two weeks in patients with non–small cell lung carcinoma who would conventionally receive 60 Gy in 30 fractions.
In the clinical setting, the authors are not aware of reports on the efficacy of HF RT in ATC patients, but several studies have shown a dose–response relationship. Pierie et al. analyzed the survival of patients who received CF RT and observed a significant improvement in survival in patients who received >45 Gy compared to those who received <45 Gy (13). A more recent retrospective analysis of 1288 patients showed patients who received >60 Gy performed better compared to those who received <60 Gy (12). The present study not only shows the efficacy of delivering the same total dose in fewer fractions, but also the superiority of HF RT compared to CF RT. Mice that underwent HF RT exhibited significant tumor growth delay, improved survival, and reduced development of regional and distant metastasis. Shorter courses of radiation may not only decrease the burden of care and improve quality of life in this population, but may also improve the radiobiological response. Several studies have shown that a RT fraction >8 Gy is necessary to induce endothelial cell damage and disruption of tumor vasculature (41 –44). In addition, immune modulation by HF RT has been shown to result in significant tumor shrinkage, leading to improved local outcomes, as well as distant control (abscopal effect) (21,45,46). Although the studies were performed in an immune-deficient model, the data clearly demonstrate that HF RT provides superior local tumor control. The absence of metastatic disease in mice that received HF RT is thus likely related to absence or continued shrinkage of the local tumor.
The radiogenomic analysis in ATC cell lines highlights biomarkers that may determine radiosensitivity of ATC cell lines. In particular, C-X-C chemokine receptor type 4 (CXCR4) was identified as a potential targetable biomarker of radioresistance in ATC. CXCR4 is a G-protein-coupled receptor, which upon binding to its sole ligand CXCL12 (also known as stromal cell-derived factor-1 and expressed by macrophages and neutrophils) leads to chemotaxis, enhanced intracellular calcium, cell adhesion, survival, proliferation, and gene transcription (47). Overexpression of CXCR4 by cancer cells has been shown to contribute to tumor growth, invasion, angiogenesis, metastasis, and therapeutic resistance (48 –50). Blockade of CXCR4 signaling has been shown to disrupt tumor–stromal interactions, sensitize cancer cells to cytotoxic drugs, and reduce tumor growth and metastases (51,52). In the first study of its kind, Kioi et al. tested the hypothesis that blockade of CXCR4 signaling can overcome radioresistance in animal models of glioblastoma multiforme (53). The study found that the combination of CXCR4 inhibition and RT completely abrogated tumor growth in U251 intracranial tumors compared to either therapy alone. The study further demonstrated that CXCR4 blockade prevents infiltration of BMDCs and inhibits vasculogenesis. Future studies in the authors' laboratory are aimed at further validating the role of CXCR4 and associated signaling pathways in mediating radioresistance in ATC. Currently, several clinical trials are testing the safety and efficacy of CXCR4 antibodies in patients with advanced and metastatic solid tumors (NCT02179970, NCT03277209, and NCT02737072).
In conclusion, this study provides preclinical evidence that HF RT is superior to CF RT in a radioresistant model of ATC. HF RT significantly reduced tumor growth and metastasis development and prolonged survival. These findings have direct clinical implications for enhancing treatment outcomes and survival in ATC patients.
Footnotes
Acknowledgments
Dr. Karam is supported by the Paul Calabresi Career Development Award for Clinical Oncology (K12) and the RSNA award. This work was supported by NIH grant #P30-CA046934.
Author Disclosure Statement
No competing financial interests exist.