
Abstract
Background:
Metformin is the most-prescribed oral medication to lower blood glucose worldwide. Some data suggest that metformin may have a role in the treatment of patients with thyroid nodules, but contrasting results are reported in different settings. This study explores and critically reevaluates the knowledge on this topic.
Methods:
A literature search identified 250 records. Studies evaluating the size of thyroid nodules before and after metformin treatment were included. Assessed outcomes were the size of thyroid nodules, thyrotropin (TSH) level, thyroid gland volume, and insulin resistance index (HOMA-IR). After screening and full-text assessment, five studies were included in the systematic review. Random-effects meta-analyses of the standardized mean difference (SMD) were performed for the four outcomes of interest. Heterogeneity was estimated using I 2, and the quality of evidence was assessed for each outcome using the Grading of Recommendations Assessment, Development, and Evaluation guidelines.
Results:
A total of 189 patients were included in the final analysis. After metformin treatment, a slight but significant reduction in thyroid nodule size was found in four studies, which included a total of 167 patients (SMD 0.46 [confidence interval (CI) 0.00–0.93]; p = 0.05). Similarly, in four studies reporting on a total of 146 patients, significant reductions in TSH level (SMD 0.30 [CI 0.07–0.53]; p = 0.01) and HOMA-IR level (SMD 0.90 [CI 0.12–1.67]; p = 0.02) were reported after treatment with metformin. In two studies, which included 114 patients, no change in thyroid gland volume was discovered after treatment with metformin (SMD 0.21 [CI −0.05 to 0.47]; p = 0.11). Quality of evidence was generally assessed as low or very low.
Conclusions:
Metformin induces reductions in thyroid nodule size and TSH and HOMA-IR levels in patients with thyroid nodules and insulin resistance. In contrast, no change in thyroid gland volumes was found. Whether metformin treatment for thyroid nodules has clinical significance remains to be demonstrated.
Introduction
Thyroid nodules arise from a proliferative disease of the thyroid gland, with a published prevalence ranging from 26% to 67% (1 –3). Thyroid nodules are formed by local enlargement of the thyroid involving excessive growth and structural transformation of one or multiple areas in the normal thyroid gland (4). The clinical significance of thyroid nodules involves the possibility of thyroid cancer, which is found in 8–15% of patients (5), depending on sex, age, and exposure to other risk factors (3,6,7). Recent findings have demonstrated that individuals with hyperinsulinemia, a consequence of insulin resistance (IR), have a higher prevalence of thyroid nodules and larger thyroid glands (8). In an area of Turkey with mild to moderate iodine deficiency, patients with metabolic syndrome (MetS), of which IR is a major component (9), also have significantly increased nodule prevalence and thyroid volume (10). In the same literature, thyrotropin (TSH) was significantly positively correlated with IR diagnosis. In addition, an increasing worldwide incidence of thyroid cancer is also reported to be associated with IR (11). Taken together, these findings suggest that IR may play a crucial role in thyroid nodule formation and cancer development. These effects may be explained by previous findings that insulin and TSH can serve as growth factors and stimulate thyroid cell proliferation (12,13). This proliferative effect is partially mediated by insulin-like growth factor-1 (IGF-1). In IR, increased insulin may decrease the production of IGF-1-binding proteins and further increase the level of free IGF-1 (14).
Metformin is one of the most widely prescribed anti-hyperglycemic agents and has been irreplaceable as a first-line drug for the management of type 2 diabetes for decades (15). Its main function is to control basal glucose output by reducing glucose production in the liver and increasing glucose uptake in muscle (16). Metformin can also increase insulin binding to its receptors and abrogate IR and MetS (17,18). There is now considerable evidence that TSH and IGF-1, and the signal transduction mechanisms they regulate, are modulated by metformin (19 –22). Furthermore, the insulin-induced increase in cell proliferation can almost be abolished by metformin therapy (23). Recent clinical studies demonstrated that metformin therapy significantly decreased thyroid volume and nodule size in subjects with IR (24). Additionally, higher remission rates and survival in diabetic patients with thyroid cancer were found in clinical trials of metformin treatment (25). Therefore, as an effective insulin-sensitizing drug, metformin may play an important role as an adjuvant therapy to reduce the growth of benign and malignant thyroid lesions.
Although some studies support the effect of metformin on thyroid nodules, contrasting results were described in different clinical settings. With this background, this study appraised the evidence concerning the effectiveness of metformin for patients with thyroid nodules and IR by undertaking a meta-analysis and systematic review.
Methods
This study is registered with PROSPERO (CRD42017077868) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (see Supplementary Table S1) (26).
Search strategy
A systematic search of the literature published before July 20, 2017, was conducted in eight databases (PubMed, Embase, the Cochrane Library, Web of Science, ClinicalTrials.gov, EBSCO, Scopus, and SinoMed) to identify all articles evaluating effects on thyroid nodules in patients receiving treatment with metformin. The search strategy was developed without any language restriction. The following search terms were used: “metformin” and “thyroid nodules.” These terms were used in every possible spelling and as synonyms, acronyms, and key or text words. Details of the search strategy are provided in the Supplementary Data.
Study selection
Records returned from this search were checked for the following inclusion criteria: in humans; in adults (age ≥18 years); a clearly stated diagnosis of thyroid nodules; at least 10 participants receiving metformin; population not defined as having preexisting cancer; and a reported mean and standard deviation (SD; or median and range) of any of the following outcomes of interest: thyroid nodule size, TSH level, thyroid gland volume, or homeostasis model assessment for insulin resistance (HOMA-IR) level. There was no restriction based on the duration of follow-up. After de-duplication, titles and abstracts were screened for eligibility, and the full text of potentially relevant articles was retrieved. In addition, the references included in the relevant original papers and review articles were also screened to identify potential other relevant publications. At the study selection stage, two of the authors analyzed each article independently. In case of disagreement, a third investigator was consulted. Discrepancies were resolved by discussion and consensus. Figure 1 depicts the study selection process.
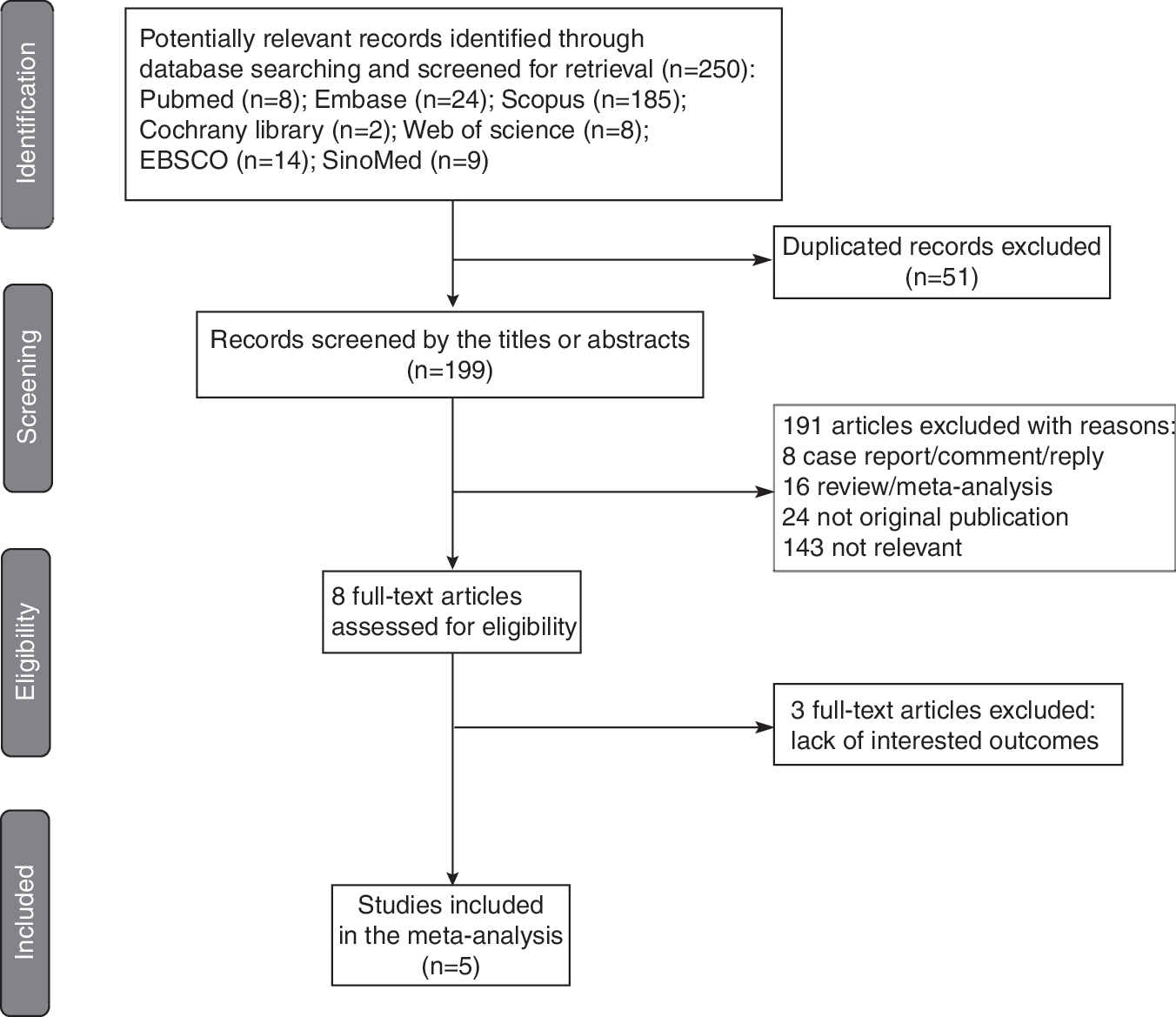
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart of the study selection process, showing the number of studies excluded at each step and the reasons for exclusion from the systematic review and meta-analysis.
Data extraction
Data concerning sample size, participant characteristics, metformin dose, duration of follow-up, and outcomes were extracted independently by two of the three authors, and any disagreement was resolved by discussion.
Statistical analysis
Statistical analysis of before/after changes for each outcome (with confidence intervals [CI]) was performed with Review Manager software v5.3 (The Cochrane Collaboration). The standardized mean differences (SMDs) were combined for each outcome in a random-effects model and presented as a forest plot. Heterogeneity between the studies was assessed using the I 2 statistic, where 0% indicates no heterogeneity, 25% may represent low heterogeneity, 25–49% may represent moderate heterogeneity, and ≥50% may represent high heterogeneity (27). Potential sources of heterogeneity were investigated. A sensitivity analysis was performed to examine the influence of individual studies. In this analysis, the meta-analysis estimate was computed after omitting one study at a time (28). To assess the potential effect of the baseline characteristics of the patients (mean age, sample size, baseline size of thyroid nodule or baseline HOMA-IR level, percentage of female patients, body mass index [BMI], length of follow-up, and metformin dose) included in the studies on the different results observed across studies, a meta-regression analysis was performed with changes in thyroid nodule size or HOMA-IR level as the dependent variable and the above-mentioned variables as independent variables.
The risk of publication bias was analyzed using Egger's test and was presented as a funnel plot of the standard difference in means versus standard error (SE) for each outcome. In contrast to the overall test of heterogeneity, the test for funnel plot asymmetry assesses a specific type of heterogeneity and provides a more powerful test in this situation. However, any analysis of heterogeneity depends on the number of trials included in a meta-analysis, a number that is generally small, and this limits the statistical power of the test. Therefore, p < 0.1 has been used as evidence of asymmetry (29).
Risk of bias was assessed and included in the analysis according to the methods recommended by the Cochrane Collaboration (30). For item allocation concealment, all studies were judged to have an unclear risk of bias because this item is not applicable in these studies and the effect of unconcealed allocation on each outcome is unknown (31). The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used to assess the quality of the evidence for each outcome.
Results
Literature research
After the removal of duplicates, the initial electronic search identified 199 articles (Fig. 1). Following the screening of titles and abstracts, the full text of eight articles was reviewed, and five articles reporting the change in thyroid nodule size after metformin treatment were included. The main reason for exclusion at the full-text stage was the lack of outcomes of interest.
Study characteristics
The characteristics of the included studies are shown in Table 1. The studies were published between 2011 and 2015. Two were undertaken in China (32,33), one in Turkey (24), one in Iran (34), and one in Argentina (35). A total of 189 patients were included in the final analysis. Of the nodules, 18.5% underwent fine-needle aspiration biopsy (FNAB), and all proved benign. Four studies reported 167 patients with a change in thyroid nodule size after metformin treatment; four studies reported 146 patients with changes in TSH levels and HOMA-IR levels after metformin treatment; and two studies reported 114 patients with a change in thyroid gland volume after metformin treatment. Duration of follow-up ranged from 3 to 12 months. No studies were assessed as having a low risk of bias. The average age of the recruited participants ranged from 46 to 60 years, and participants tended to be overweight/obese (average baseline BMI ranged from 26.4 to 34.5 kg/m2) with elevated IR (average baseline HOMA-IR scores ranged from 3.3 to 4.5).
Characteristics of the Included Studies
BMI, body mass index; HOMA-IR, homeostasis model assessment for insulin resistance; TSH, thyrotropin; IR, insulin resistance; T2DM, type 2 diabetes mellitus.
Meta-analysis
Patients demonstrated a slight but significant reduction in the size of thyroid nodules after metformin treatment (four studies: SMD = 0.46 [CI 0.00–0.93]; p = 0.05; I 2 = 69%), as shown in Figure 2A and Table 2. There was a significant decrease in TSH levels after metformin treatment (four studies: SMD = 0.30 [CI 0.07–0.53]; p = 0.01; I 2 = 0%), as presented in Figure 2B and Table 3. In contrast, no change in thyroid gland volume was discovered after treatment with metformin (two studies: SMD = 0.21 [CI −0.05 to 0.47]; p = 0.11; I 2 = 0; Fig. 2C). Figure 2D shows a significant reduction in HOMA-IR levels after treatment with metformin (four studies: SMD = 0.90 [CI 0.12–1.67]; p = 0.02; I 2 = 84%).

The role of metformin treatment in patients with thyroid nodules and insulin resistance. (
Changes in Thyroid Nodule Size After Metformin Treatment
Changes in TSH Level After Metformin Treatment
Sensitivity analysis
Meta-analyses of the change in thyroid nodule size and change in HOMA-IR levels (the two outcomes with high heterogeneity) after metformin treatment were performed both including and excluding each study. None of the results changed following the sensitivity analysis (Supplementary Fig. S1).
Meta-regression analysis
No correlation was found between the SMD of the change in thyroid nodule size after metformin treatment and mean age (p = 0.68), sample size (p = 0.32), baseline size of thyroid nodule (p = 0.51), percentage of female patients (p = 0.48), BMI (p = 0.59), length of follow-up (p = 0.58), baseline TSH concentrations (p = 0.21), or metformin dose (p = 0.71). In the analysis of the percentage of females, two studies included only females, and the remaining three included 91%, 68%, and 56% females. In absolute numbers, the total sample size was 189, only 40 of whom were male. Notably, in a meta-regression analysis evaluating the possible relationship between differences in baseline clinical and demographic characteristics and changes in HOMA-IR level, the mean age of the population was the only significant predictor of HOMA-IR changes (β = −0.15; p = 0.05), as illustrated in Supplementary Figure S2.
Publication bias
Publication bias was examined using funnel plots (Supplementary Fig. S3) and by performing Egger's test. The analysis revealed no evidence of publication bias (Egger's test: thyroid nodule: p = 0.37; TSH: p = 0.211; IR: p = 0.47; insufficient studies were available to perform Egger's test for thyroid gland volume).
Risk of bias
The included studies had, in general, low or unclear risk of bias (Supplementary Fig. S4). The two most obvious characteristics were the lack of a description regarding whether the participants and personnel were blinded and insufficient information to assess whether the intervention was random and hidden. The majority of data for this review did not show reporting bias; only one study provided no SD for the size of thyroid nodules (35). Two studies were considered to have possible limitations due to incomplete outcome data because the attrition rates in these studies were >20% (24,35). The reports of all included studies presented no other overt bias.
Quality of evidence assessment
Quality of evidence was assessed for each outcome (Supplementary Fig. S5) using the GRADE guidelines (36 –44). Inconsistency was therefore assessed by comparing the findings of the studies. Imprecision was concluded when CIs included a null effect. All outcomes were downgraded for risk of bias due to the high risks of attrition bias and reporting bias, as well as the unclear risks for selection bias, performance bias, and detection bias that exist in the included studies. The quality of evidence regarding the changes in thyroid nodule size and TSH level was assessed as low, while quality of evidence for the change in thyroid gland volume and HOMA-IR level was assessed as very low.
Discussion
To the best of the authors' knowledge, this is the first meta-analysis to assess the role of metformin in patients with thyroid nodules and IR. It was found that metformin can significantly reduce thyroid nodule size. Additionally, a reduction in TSH was induced by metformin treatment. Most likely, the metformin therapy reduced HOMA-IR. In contrast, no change in thyroid gland volume was reported in these patients.
The low I 2 values for the heterogeneity of the TSH level change and the change in thyroid gland volume strongly indicate no heterogeneity, as previously published (45). However, high clinical heterogeneity with an I 2 of >50% was found in studies reporting the change in thyroid nodule size. Interestingly, after the removal of one study conducted by Wang (33) from the analysis, similar results were confirmed, but the heterogeneity was changed to 9%. This special study included only female patients with the highest baseline thyroid nodule size (1.10 ± 0.33 mL) and TSH levels (2.78 ± 0.78 μIU/mL). Similarly, the I 2 value for the change in HOMA-IR, which was analyzed in populations with varying background characteristics, was also >50%. Notably, the meta-regression analysis showed that the mean age of the population can predict HOMA-IR level change, with less change in the HOMA-IR level observed in elderly patients.
The mechanism by which metformin acts on thyroid nodules presenting with IR is complex and remains largely unknown. Metformin has been domestically and internationally recognized as a first-line insulin sensitizer that acts by decreasing insulin/IGF-1 signaling, thereby improving hyperinsulinemia and enhancing insulin sensitivity (46). Ayturk et al. mentioned that IR can be an independent risk factor for thyroid nodule formation, with mild IR as the main factor (47). Therefore, it can be inferred that IR and hyperinsulinemia may contribute to increased nodule prevalence, and the improvement of insulin sensitivity by metformin therapy may act to ameliorate these morphological abnormalities.
Both rosiglitazone (48) and pioglitazone (49) have been reported to improve IR much more than metformin. The long-term use of rosiglitazone has been associated with a reduction in the risk of thyroid cancer, but there is no significant dose–response relationship (50). In contrast, the use of pioglitazone is not related to a risk of thyroid cancer (51). Metformin, however, significantly reduced the risk of thyroid cancer after a short period and showed a significant p trend (52). These observations argue against a potential role of IR and suggest the existence of some other mechanisms affecting the development of thyroid cancer and, likely, thyroid nodules.
Another hypothesis is that metformin can inhibit the growth of thyroid cells (53). Studies at the cellular level demonstrate that metformin activates adenosine monophosphate-activated protein kinase, which is a key regulator of intracellular energy homeostasis that can inhibit thyroid cell growth through the suppression of mammalian target of rapamycin/p70S6K signaling (54).
As mentioned above, IGF-1 plays a meaningful role in metformin treatment for proliferative disease (55,56). IGF-1 is also actively involved in the TSH-mediated proliferation of thyrocytes. The insulin/IGF-1 signaling pathway has long been known to modulate the regulation of thyroid gene expression and might be an important factor in thyrocyte proliferation, differentiation, and malignant transformation. In addition, Kimura et al. noted that TSH, via cAMP together with insulin or IGF-1, can stimulate cell cycle progression and proliferation in various thyrocyte culture systems. Therefore, it is necessary to analyze the role of insulin/IGF-1 in the action of metformin on thyroid nodules.
In a recently published meta-analysis of TSH level change in 54 euthyroid patients after treatment with metformin, a significant reduction in the TSH level was reported both in overt and in subclinical hypothyroidism. No change in TSH level was found in euthyroid people. However, a significant decrease in TSH level was demonstrated in the present study, which included only euthyroid individuals. This finding is supported by a recent study conducted in 170 euthyroid patients showing that metformin has a TSH-lowering effect in patients who test positive for thyroid peroxidase antibodies (57). In another large retrospective study conducted by Cappelli et al., a significant reduction of TSH was also shown in euthyroid patients with higher baseline TSH levels (20). Various hypotheses have been proposed to explain the mechanisms by which metformin exerts its TSH-lowering effect in euthyroid patients. Rezzónico et al. noted that the effect of metformin on TSH secretion might depend to some extent on the hormone's circulating concentration (35). In addition, Santos-Palacios et al. believed that metformin may have a “buffer effect” on serum TSH levels in euthyroid diabetic patients (58). Kouidhi et al. strongly support the notion that the changes in TSH after metformin therapy may be influenced by adiposity and its metabolic consequences, such as IR (59), a notion that is supported by the results of the present study.
In addition to TSH, the effect of metformin on thyroid hormone has been widely discussed. Vigersky et al. first discovered that metformin can suppress TSH without changing free thyroxine (fT4) or free triiodothyronine levels in patients with chronic hypothyroidism (19). These results were confirmed by Isidro et al. in obese, diabetic women with primary hypothyroidism (60). In a study conducted in 72 diabetic patients with either primary hypothyroidism or normal thyroid function, no significant change in fT4 levels was observed after one year of metformin administration (61). Similar results were found in hypothyroid patients with polycystic ovary syndrome (PCOS) (62). Serum TSH levels were significantly reduced, and fT4 levels remained unchanged. In addition, Cappelli et al. reported that serum fT4 levels did not change in diabetic patients, regardless of whether metformin or levothyroxine (LT4) was used (20). For patients with thyroid nodules, more studies are needed to demonstrate the effect of metformin treatment on thyroid hormone levels.
Strengths and weaknesses
The strengths of this meta-analysis include the robustness of the conclusions of the sensitivity analysis and the fact that the nodules diagnosed by histopathology all proved to be benign. By meta-analyzing populations from different studies, the present study was able to evaluate the effects of metformin on thyroid nodule size, TSH level, thyroid gland volume, and HOMA-IR level simultaneously in a larger study sample and to adjust the results for the presence of some confounding factors. Indeed, age was confirmed as a predictor of metformin-induced changes in HOMA-IR level by means of a meta-regression approach. Notably, the Cochrane Handbook of Systematic Reviews recommends that at least 10 studies be included in meta-regression analysis. Therefore, the present results regarding the relevance of age and metformin-induced changes in HOMA-IR level should be interpreted with caution, and further study is needed to demonstrate the corresponding results.
This meta-analysis has some potential limitations. First, the number of male subjects in this meta-analysis was low, and two studies (33,35) included only females. This may be attributed to the female predominance in thyroid disease and the higher tendency of women to participate in these research projects. A larger sample size may help solve this problem, and it is expected that sex differences will be discovered in future studies. Second, the follow-up ranged from 3 to 12 months. However, three months might be too short to observe changes in thyroid volume and nodule size. Third, the limited number of studies hindered the implementation of subgroup analysis. Fourth, the percentage of FNAB was relatively low. In future studies, it will be necessary to diagnose thyroid nodules with both ultrasound and FNAB. In addition, the quality of evidence for metformin treatment depends on the quality of individual studies. In this study, descriptions regarding blinding and allocation concealment were not always reported, limiting the assessment of risk. In future trials, a detailed description of the process and methods used is important. At the same time, randomized controlled trials (RCTs) of a higher methodological quality are needed to improve the quality of evidence. Finally, all the patients had IR, and the effect of metformin may not be applicable to patients without IR.
Implications of findings
Many studies have examined the effect of metformin on thyroid nodules, but the sample size and the outcome indicators were limited in these studies. Using this meta-analysis, relevant outcomes can be integrated and a more comprehensive analysis can be obtained, which can provide guidance for clinicians. This study found that metformin may have clinical significance apart from the treatment of type 2 diabetes. First, IR is common in patients with newly diagnosed type 2 diabetes, PCOS, MetS, or obesity. Early use of metformin may block the insulin/IGF-1 pathway, thereby reducing the incidence of thyroid nodules. Second, although most thyroid nodules are benign, the size of thyroid nodules tends to increase with time, decreasing the quality of life (63). If metformin treatment can reduce thyroid nodule size or prevent any increase in size, slowing or preventing the natural process of nodule development will be possible, resulting in a benefit to patients. In addition, a decrease in nodule size may relieve patient anxiety about malignant change. Finally, the effect of LT4 therapy in reducing nodule size is modest, and LT4 treatment may cause iatrogenic thyrotoxicosis (64). If metformin is a viable alternative to LT4 in these patients, it may reduce the risk of iatrogenic hyperthyroidism caused by LT4 treatment. Meanwhile, additional high-quality RCTs and multicenter studies are needed to demonstrate the efficacy and safety of metformin in patients with thyroid nodules and IR.
Conclusions
This meta-analysis suggests that metformin treatment is effective for patients with thyroid nodules and IR and is able to reduce the size of thyroid nodules and decrease TSH and HOMA-IR levels. These findings suggest a broader use of this drug not only for type 2 diabetes but also for proliferative thyroid disease and MetS. Further exploration, including mechanistic studies and well designed prospective studies, is needed to address relevant issues.
Footnotes
Acknowledgments
We thank Dr. Fabian Pitoia for providing information and assistance regarding one of the included studies (![]() ). This study was supported by grants from the National Natural Science Foundation of China (81370920, 81770773), the Natural Science Foundation of Jiangsu Province (BK20171499), the Project of “Six Talents Peak of Jiangsu Province” (2013WSN-023), the Jiangsu Province Key Medical Talents (co-construction) Program, the Project of “333” Talent in Jiangsu Province, the Jiangsu Province Official Hospital Scientific Research Initial Funding (RPF201501), and the Jiangsu Province Official Hospital Talents Construction Fund Research Project (IR2015101).
). This study was supported by grants from the National Natural Science Foundation of China (81370920, 81770773), the Natural Science Foundation of Jiangsu Province (BK20171499), the Project of “Six Talents Peak of Jiangsu Province” (2013WSN-023), the Jiangsu Province Key Medical Talents (co-construction) Program, the Project of “333” Talent in Jiangsu Province, the Jiangsu Province Official Hospital Scientific Research Initial Funding (RPF201501), and the Jiangsu Province Official Hospital Talents Construction Fund Research Project (IR2015101).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.