
Abstract
Background:
The fact that serum thyrotropin (TSH) levels increase with age may influence the diagnosis of thyroid diseases in older adults. This study aimed to establish an age-specific serum TSH reference range, examine the prevalence of thyroid diseases in older adults ≥65 years, and analyze the risk factors.
Methods:
A cross-sectional study of adult populations in 10 cities in China was conducted from 2010 to 2011. A total of 15,008 subjects were randomly selected and completed the present study. Urinary iodine concentration, serum TSH, thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TgAb) titers were measured. Thyroid ultrasonography and questionnaires were completed by all the subjects. When the TSH level was abnormal, free thyroxine and/or free triiodothyronine levels were measured.
Results:
When the reference range of the general population was used, the prevalence rates of overt hypothyroidism (Ohypo) and subclinical hypothyroidism (Shypo) in older adults ≥65 years were significantly higher than those in younger adults <65 years (2.09% vs. 0.80% and 19.87% vs. 16.23%, respectively; p < 0.001). Positive TPOAb and positive TgAb were associated with the prevalence of Shypo in older adults. An age-specific serum TSH reference range was formulated according to guidelines set forth by the National Academy of Clinical Biochemistry. Both the median and upper limit values of serum TSH in older adults were higher than those in younger adults (2.58 [0.75–8.86] mIU/L vs. 2.38 [0.76–6.57] mIU/L; p < 0.001). Using the age-specific serum TSH reference range, the prevalence of Shypo in older adults was 3.3%, which was significantly lower than the prevalence based on the reference range of the general population (3.3% vs. 19.87%). The prevalence rates of Ohypo, overt hyperthyroidism (Ohyper), and subclinical hyperthyroidism (Shyper) did not change much (Ohypo: 1.6% vs. 2.09%; Ohyper: 0.7% vs. 0.52%; and Shyper: 3.8% vs. 0.73%). Positive TPOAb, but not positive TgAb, was also associated with the prevalence of Shypo as diagnosed with the age-specific serum TSH reference range.
Conclusion:
The serum TSH level increases with age, which may represent a normal compensatory phenomenon in older adults ≥65 years. To prevent misdiagnosis and mistreatment, the use of an age-specific serum TSH reference range is recommended in older adults for the diagnosis of thyroid diseases.
Introduction
The prevalence of thyroid diseases in older adults remains controversial. Studies have reported that aging is associated with an increased prevalence of thyroid dysfunction, although the results of epidemiological studies in various regions differ. The reasons for these differences may be due to different diagnostic criteria, different target selection, the radioimmunoassay of TSH used in the past, and other factors.
The serum thyrotropin (TSH) level increases with age, particularly in women. This increase is believed to be due to high levels of thyroid antibodies. However, more recent studies have indicated that even if the interference of thyroid disorders and thyroid antibodies is excluded, the serum TSH distribution curve is shifted to the right, and the 97.5th percentile of the serum TSH still increases with age (1 –6). The third American National Health and Nutrition Examination Survey (NHANES III) demonstrated that after 30–39 years of age, the 97.5th percentile of serum TSH increases by 0.3 mIU/L for every age increase of 10 years (7).
Basic studies have demonstrated that the thyroid gland in older people takes up less iodine and that the thyroid weight, colloid component, and follicular volume decrease in the general older population. Consequently, the thyroid gland synthesizes fewer hormones in older adults. Because of the slow rates of degradation, serum triiodothyronine (T3) and thyroxine (T4) are maintained at steady states (8). However, serum TSH in older adults increases (9), presumably due to a reduction in TSH bioactivity or a reduction in the responsiveness of the thyroid to TSH (10). The increase in serum TSH levels in older people without a reduction in circulating T4 may represent a phenomenon of physiological adaptation.
Studies have revealed that persistent subclinical hypothyroidism (Shypo) influences the structure and function of the heart (11,12) and increases the risk of heart failure (13,14), cardiovascular events, and overall mortality rates (15,16). However, such correlations have not been confirmed in people >65 years of age or in people >80 years of age (16 –20). Subclinical hyperthyroidism (Shyper) can lead to osteoporosis and increases in atrial fibrillation in older adults. Shyper is also related to left ventricular hypertrophy (21). Recently, a randomized trial (the TRUST study) revealed that levothyroxine elicited no clinical benefit in older adults who were at least 65 years of age with Shypo when compared to a placebo group (22). Moreover, increases in TSH in the old and very old have been associated with longevity (18,19,23). The overtreatment of Shypo due to inappropriate diagnosis can induce atrial fibrillation, nervousness, and a decrease of bone mineral density, and is even associated with increased mortality in the aged (24). Resetting an age-specific serum TSH reference range is strongly required before any diagnosis is made and treatment is implemented (23).
The above-mentioned studies indicate that older individuals comprise a special population, and thyroid diseases should be diagnosed and treated carefully. In this study, epidemiological data from 10 Chinese cities were used to analyze the prevalence of thyroid diseases in older adults and to study the risk factors for Shypo. The use of an age-specific reference range of serum TSH for the diagnosis of thyroid disorders in the older population is also discussed.
Methods
Subjects
An epidemiological study addressing thyroid diseases was conducted in 10 cities in China from 2010 to 2011. One or two communities were randomly chosen from each city, and 1500 subjects were enrolled to yield a total of 15,008 participants. Because the data were incomplete and due to other reasons, 23 subjects were lost to follow-up. A total of 14,985 subjects completed the study. Their ages ranged from 15 to 92 years (45.5 ± 14.9 years), and the ratio of men to women was 6315:8670 (1:1.4) (23,25).
The exclusion criteria were: (i) women who were pregnant or lactating within one year; (ii) patients taking contraceptives or estrogens; (iii) patients taking glucocorticoids, dopamine, dobutamines, and so on.; (iv) patients taking antiepileptic drugs (phenytoin sodium, carbamazepine, etc.); (v) patients with adrenal insufficiency, renal insufficiency (failure), or other serious systemic diseases; (vi) patients who had undergone tests using an iodine contrast agent and those who had taken amiodarone within half a year; and (vii) patients who had lived in the city for <10 years.
Older individuals were defined as those aged ≥65 years. Participants were divided into two groups: (i) an group of older individuals consisting of 1917 people with a ratio of men to women of 818:1099 (1:1.4) and an average age of 71.32 years (range 65–92 years); and (ii) a group of younger adults consisting of 13,068 people with a ratio of men to women of 5497:7571 (1:1.4) and an average age of 41.67 years (range 15–64 years).
According to Guideline 22 of the National Academy of Clinical Biochemistry (NACB) (26), a reference population of 8041 people (age ≥65 years, 747 people; age <65 years, 7294 people) was selected to formulate a serum TSH reference range. The exclusion criteria included positivity for thyroid antibodies (thyroid peroxidase antibody [TPOAb] and thyroglobulin antibody [TgAb]), a personal or family history of thyroid dysfunction, thyroid goiter or nodules that could be distinguished or were touchable, and the use of thyroid medications.
Urinary iodine concentration and serum TSH, TPOAb, and TgAb titers were measured. Thyroid ultrasonography and questionnaires were completed by all subjects. When the TSH level was lower than the laboratory reference range, free thyroxine (fT4) and free triiodothyronine (fT3) were measured. When the TSH level was higher than the laboratory reference range, fT4 was measured.
Methods
Fasting venous blood and urine samples were collected between 8.00am and 10.00am. All samples were stored at −20°C and transferred within one month to the laboratory in Shenyang for centralized measurements.
Serum TSH, fT3, fT4, TPOAb, and TgAb were measured with the electrochemiluminescence immunoassay method using a Cobas 601 analyzer (Roche Diagnostics, Basel, Switzerland). The laboratory reference ranges used in this study were: TSH 0.27–4.2 mIU/L, fT4 12–22 pmol/L, fT3 3.1–6.8 pmol/L, TPOAb 0–34 IU/L, and TgAb 0–115 IU/L. The functional sensitivity for serum TSH was 0.002 mIU/L. The intra-assay coefficients of variation (CVs) of the serum TSH, fT3, fT4, TPOAb, and TgAb were 1.1–6.3%, and the inter-assay CV values ranged from 1.9% to 9.5%.
Thyroid ultrasonography was performed by well-trained physicians using a LOGIQa50 (7.5 MHz linear transducer; GE, Milwaukee, WI).
Diagnostic criteria
The criteria for overt hyperthyroidism (Ohyper) were: TSH <0.27 mIU/L, fT4 > 22.0 pmol/L, and/or fT3 > 6.8 pmol/L. The criteria for Shyper were: TSH <0.27 mIU/L and fT3 and fT4 in the reference ranges. The criteria for overt hypothyroidism (Ohypo) were: TSH >4.2 mIU/L and fT4 < 12.0 pmol/L. The criteria for Shypo were: TSH >4.2 mIU/L and fT4 in the reference range. The criteria for positive thyroid antibodies were: TPOAb >34 IU/mL or TgAb >115 IU/mL. Normal thyroid ultrasonography included: (i) homogeneous glandular echogenicity, (ii) no nodule(s), (iii) no goiter, (iv) no obvious small or absent thyroid gland, and (v) no calcifications or acoustic halo. The criteria for diffuse goiter included: thyroid volume >19.4 mL for women and >25.6 mL for men, and no nodules (thyroid volume was defined as length × width × thickness × 0.479).
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). The Kolmogorov–Smirnov method was used to test for normal distribution of the data. The distribution of TSH was non-normal, whereas the logTSH was close to normally distributed. t-Tests were used to analyze the mean values of the continuous variables with normal distributions, which included age and the logTSH. The Student–Newman–Keuls test was used to analyze the TSH levels in the various groups. Continuous variables with non-normal distributions, such as body mass index (BMI) and urinary iodine, were compared using the Mann–Whitney rank sum test. Proportions were compared using the chi-square test for categorical variables. The prevalence rates of thyroid diseases in the subgroups were compared using binary logistic regression with adjustments for both age and sex. The TSH reference range was defined by the 2.5th and 97.5th percentiles. p-Values of <0.05 were considered significant.
Medical ethics
The research protocols were approved by the medical ethics committee of China Medical University. All subjects provided written informed consent after having been given a full explanation of the study.
Results
Prevalence of thyroid diseases in older and younger adults
The subjects were divided into two groups by age (<65 years and ≥65 years). There was no statistically significant difference in sex distribution between the two groups (p = 0.616). The median and distribution of the BMI were higher in older adults than in younger adults (p < 0.001). The positive rate of TPOAb was 13.77% in older adults, which was higher than that in younger adults (11.20%; p = 0.037) after adjusting for sex and BMI. However, there was no obvious difference in the positive rate of TgAb. Among the older adult population, 19.30% were positive for at least one antibody, 8.19% were positive for two antibodies, 5.58% were positive for TPOAb only, and 5.53% were positive for TgAb only.
A total of 23.21% of the individuals in the older adult group had thyroid disorders. The prevalence of thyroid goiter, Shypo, and Ohypo in the older adult group was higher than in younger adults (p < 0.001) after adjusting for sex, BMI, urine iodine, TPOAb, and TgAb. The prevalence of Shypo in older adults was 19.87%, which was 1.397 times higher than that in younger adults (16.23%; p < 0.001). There were no statistically significant differences in the prevalence rates of Ohyper or Shyper between the two groups. The results of the screening for thyroid disorders in older and younger adults are presented in Table 1.
Prevalence of Thyroid Diseases in the Elderly and Non-Elderly
p < 0.05; ** p < 0.01.
TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody; Shypo, subclinical hypothyroidism; Ohypo, overt hypothyroidism; Shyper, subclinical hyperthyroidism; Ohyper, overt hyperthyroidism.
Risk factors for Shypo in older adults
After multifactor correlation analysis, the increasing prevalence of Shypo in older adults was found to be related to positivity for TPOAb and TgAb (p = 0.020 and p = 0.029, respectively). Sex, age, BMI, and urine iodine did not influence the prevalence of Shypo. Further analysis comparing the prevalence of Shypo after dividing the older adult population into different subgroups yielded similar results (Table 2).
Risk Factors of Shypo in the Elderly
p < 0.05; ** p < 0.01.
OR, odds ratio; CI, confidence interval; BMI, body mass index; AII, adequate iodine intake; MTAII, more than adequate iodine intake.
Serum TSH reference range in older adults
The reference population was divided into six subgroups according to age. The age-specific reference ranges for serum TSH are presented in Table 3. The serum TSH level in the ≥65-year-old group was significantly higher than those in the younger groups (Fig. 1). There were no significant differences between the other age groups. In the reference population, the median concentration of serum TSH in older adults was 2.58 mIU/L, which was higher than that in younger adults (2.38 mIU/L; p < 0.001). The 2.5th–97.5th percentile ranges for TSH were 0.75–8.86 mIU/L in older adults and 0.76–6.57 mIU/L in younger adults. The upper limit was higher in the older reference population (Table 3).
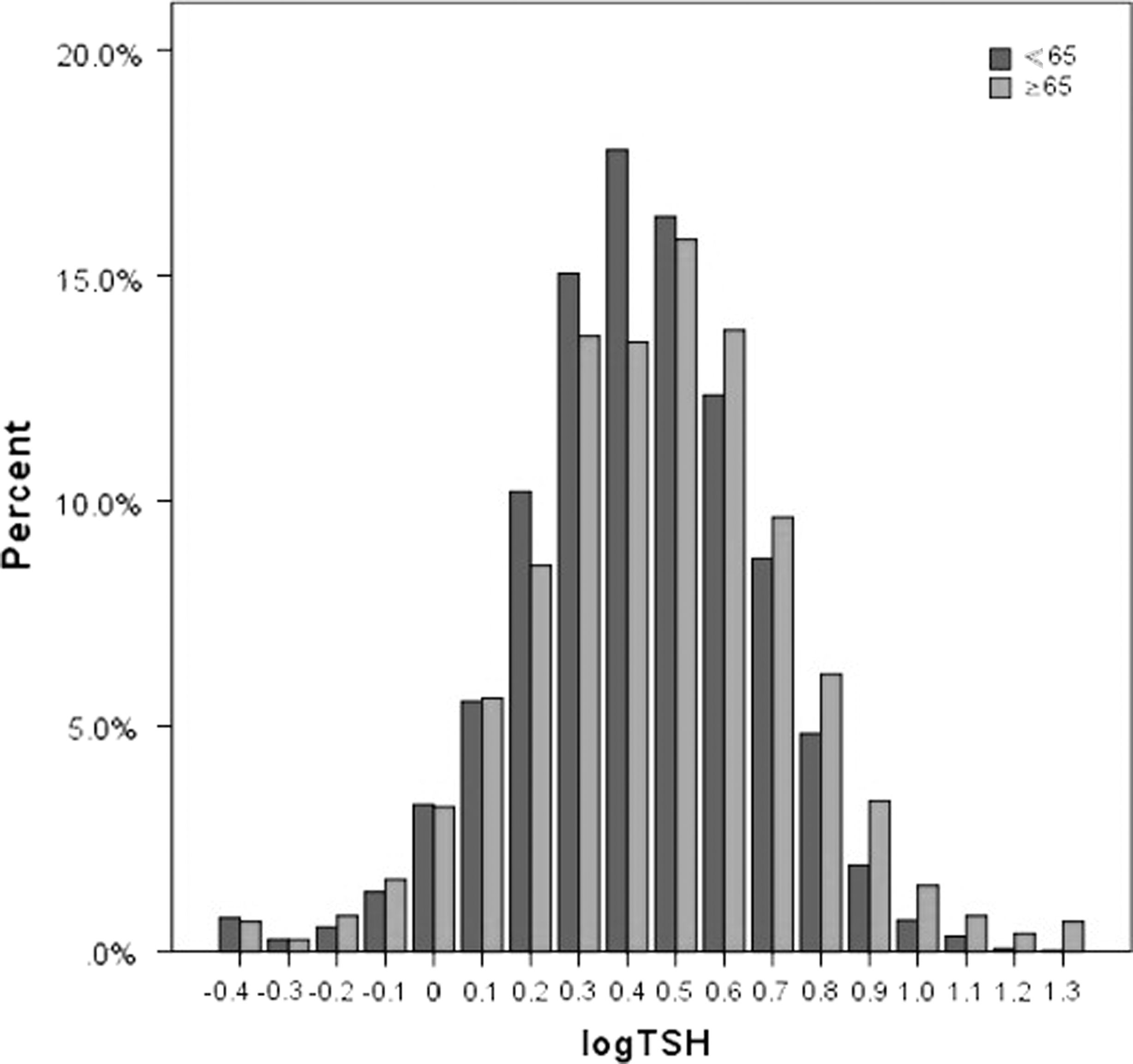
Serum TSH levels by age.
Serum TSH Ranges of Different Age Subgroups in the Reference Population
p < 0.05 compared to any other group.
TSH, thyrotropin.
Prevalence of thyroid diseases in older adults, depending on the age-specific serum TSH reference range
Depending on the age-specific serum TSH reference range, the prevalence of Shypo in older adults was 3.3%, which was lower than that in younger adults (4.3%; p = 0.049). However, the prevalence rates of Ohypo and Shyper were higher in older adults than those in younger adults (Ohypo: 1.6% vs. 0.7%, p < 0.001; Shyper: 3.8% vs. 2.4%, p = 0.017; Table 4).
Prevalence of Thyroid Diseases with Age-Specific Serum TSH Reference Ranges
p < 0.05; ** p < 0.01.
Using the age-specific serum TSH reference range, the prevalence of Shypo in older adults was 3.3%, which was significantly lower than that based on the reference range for the general population (3.3% vs. 19.87%). The prevalence rates of Ohypo, Ohyper, and Shyper were similar to those based on the reference range of the general population (Ohypo: 1.6% vs. 2.09%; Ohyper: 0.7% vs. 0.52%, Shyper: 3.8% vs. 0.73%).
Risk factors for thyroid diseases diagnosed with the age-specific serum TSH reference range in older adults
Among older adults, the Shypo individuals, as diagnosed using the age-specific serum TSH reference range, had higher positive rates of TPOAb and TgAb than those diagnosed based on the laboratory reference range (TPOAb: 31.3% vs. 22.8%; TgAb: 28.1% vs. 21.5%).
After multifactor correlation analysis, the older people with positive TPOAb results were more likely to suffer from Shypo (p = 0.016), whereas positive TgAb status, sex, age, BMI, and urine iodine were not relevant. Further analyses after dividing the older subjects into different subgroups yielded similar results and thus ruled out the influence of positive TgAb on the prevalence of Shypo (Table 5).
Risk Factors of Shypo Diagnosed with Age-Specific Serum TSH Reference Ranges in the Elderly
p < 0.05; ** p < 0.01.
Discussion
The present study formulated an age-specific serum TSH reference range based on NACB guidelines. The median (2.5th–97.5th percentile) serum TSH levels were 2.58 mIU/L (0.75–8.86 mIU/L) in older adults and 2.38 mIU/L (0.76–6.57 mIU/L) in younger adults, and the two groups exhibited significant differences. When thyroid diseases in the older subjects were re-diagnosed using the age-specific serum TSH reference range, almost 16% of the older people diagnosed with Shypo using the serum TSH reference range for the general population were found to be euthyroid. After using the age-specific serum TSH reference range, the prevalence of Ohypo changed from 2.09% to 1.6%, and the prevalence of Shyper changed from 0.73% to 3.8%. Therefore, to avoid older individuals with slightly increased TSH being overtreated and older subjects with Shyper experiencing delayed treatment, it is recommended that the age-adjusted TSH reference range should be considered when diagnosing thyroid diseases in older adults.
Based on the general analyses of the existing research results, the prevalence of Ohyper in older adults is 0.5–4%, and Graves' disease remains the main etiology (27). In a report by Boelaert et al., a large multicenter study of 3049 older people revealed that the majority of older patients had one or two symptoms, whereas the majority of young patients had more than five symptoms. Due to a lack of signs and symptoms in older people, Ohyper can be difficult to diagnose, which may lead to treatment delays or even more serious outcomes (28). Compared to Ohyper, the prevalence of Shyper is as high as 3–8%, and the prevalence in women is higher than in men (29,30). In the present study, the prevalence rates of Ohyper and Shyper as diagnosed with the laboratory reference range in older adults did not differ significantly from those in younger adults. When using the age-specific reference range for diagnosis, the prevalence of Shyper in older adults differed significantly from that in younger adults (3.8% vs. 2.4%, respectively; p = 0.017), while the prevalence of Ohyper did not show a difference (0.7% vs. 1.1%; p = 0.128).
Existing studies have demonstrated that the prevalence of Shypo in older adults is 2.9–15% (31 –36) and increases with age, especially in women (34,37). In this study, the prevalence of Shypo in older adults was 19.87% and was higher than that in younger adults (16.23%; p < 0.001). The prevalence of Shypo in women was 21.57%, which was slightly higher than that in men (17.60%), but the difference was not significant (p = 0.210). The prevalence rates of Ohypo (2.09%) and goiter (5.79%) were also both significantly higher in older adults. The cause of the higher prevalence of Shypo in older adults in this study was related to the lower upper limit of the serum TSH reference range. A study conducted in the United States to investigate Shypo in older adults based on 3233 individuals aged ≥65 years demonstrated that the prevalence was 15.0% when the upper limit of the TSH range was 4.5 mIU/L (32). Another study in the United Kingdom with 5960 individuals aged ≥65 years demonstrated that the prevalence of Shypo was 2.9% when the upper limit of the TSH range was 5.5 mIU/L (34). The upper limit of the TSH reference range as defined by the authors' laboratory was 4.2 mIU/L, which was lower than those utilized in the studies described above. Therefore, the upper limit of the TSH reference range has a great influence on the prevalence of Shypo in older adults.
Serum TSH increases with age. Surks et al. also considered that the distribution of TSH shifts to the right in older adults, and in the normal population, the TSH level is higher in older people than in younger individuals (4,38). In this study, after establishing the age-specific serum TSH reference range, the serum TSH upper limit was significantly higher in older adults than in younger adults. After subdividing the reference population by 10-year intervals into six subgroups, the TSH was significantly higher in the >65-year-old group than in the other groups. A recent study measured the TSH distributions of different age groups among 153,127 people and revealed that the 97.5th percentile TSH level increased with age, while the 2.5th percentile decreased (39), which is in agreement with the present results. Bremner et al. followed a reference group of 908 individuals for 13 years and found that the largest TSH increase occurred in the people with the lowest TSH at baseline and not in those with higher TSH levels (10). This finding indicated that a slight increase in the TSH level in older adults does not suggest Shypo and reflects a normal phenomenon. Therefore, some researchers believe that the TSH reference range should be broadened with progressing age. Not all individuals with slightly increased TSH levels are Shypo patients who should be treated with levothyroxine replacement. This study analyzed the prevalence of Shypo in older people with the age-specific serum TSH reference range and found that the prevalence of Shypo decreased from 19.87% to 3.3%, whereas the prevalence of Ohypo decreased from 2.09% to 1.6%. Nevertheless, one study suggests the opposite (40). The authors of that study analyzed TSH results from 148,938 participants and reached the conclusion that the use of age-specific reference ranges for TSH has only minor effects on thyroid status except among the very old. Only 0.1–1.9% of individuals were reclassified as normal or abnormal when using the age-specific upper limits compared to a common cutoff of 4.0 mIU/L (40). However, in the present study, the percentage of diagnoses changed by approximatively 16%. These results indicate that older people with a slightly elevated TSH level may be overdiagnosed. A resetting of the TSH normal range according to age is strongly required.
Some studies have reported that the positive rate of TPOAb in older adults is 15–20% (7,41) and that the positive rate in older patients with Shypo reaches up to 40–67% (42). In the present study, the positive rate of TPOAb was 13.77% in older adults, which was significantly higher than that in younger adults (11.20%; p = 0.037). The positive rate in the older Shypo patients reached 22.83%. The NHANES III indicated that the positive rate of antibodies is higher in women than in men. The TPOAb and TgAb positive rates increased with age, and the trend was more obvious in women (7). The phenomenon of thyroid antibody positive rates increasing with age has also been reported in other studies. Because the main etiology of Shypo is thyroid autoimmunity, the present study reached a similar conclusion by comparing the prevalence rates among subgroups and utilizing multifactor correlation analysis; positive TPOAb and positive TgAb statuses were relevant to the increasing prevalence of Shypo in older adults (p = 0.020 and 0.029). Sex, age, BMI, and urine iodine did not influence the prevalence of Shypo. In older adults, the risk of developing Shypo was 1.59 times higher for the TPOAb-positive individuals than for the TPOAb-negative individuals, 1.52 times higher for the TgAb-positive individuals than for the TgAb-negative individuals, and 2.43 times higher for those who were positive for both antibodies than for those who were negative for both antibodies. However, the positive rate of TPOAb was 31.25% in older adult patients with Shypo who were diagnosed using the age-specific serum TSH reference range. The prevalence of Shypo was only relevant to positive TPOAb status. The NHANES III also indicates that positive TPOAb status is relevant to hyperthyroidism and hypothyroidism, whereas positive TgAb status has no influence on the prevalence of thyroid diseases (7).
Positive TPOAb status has also been identified as a risk factor for the progression from Shypo to Ohypo in most studies. The Whickham 20-year follow-up study conducted in the 1970s revealed that the incidences of Ohypo were 4.3% in female patients with both an increased serum TSH level and positivity for thyroid antibodies, 2.6% for those with an increased serum TSH level only, and 2.1% for those with positive thyroid antibodies only (43). However, another study from the United States on cardiovascular health reported that the progression from Shypo to Ohypo in older people is independently related to a TSH value >10 mIU/L but not related to a positive TPOAb status (44). Considering that TPOAb are involved in the pathogenesis of Shypo, a risk factor for developing into Ohypo and an indicator for guiding treatment, their significance, especially in older people, should be further explored.
Serum TSH concentrations gradually increase during healthy aging, but fT4 concentrations remain unchanged (23). However, in patients with primary autoimmune hypothyroidism, the logTSH exhibited an inverse linear correlation with age, which means that for the same degree of low serum T4, the serum TSH level was lower among older adults (45). In another study that established reference intervals for TSH and fT4, age, sex, and the hour of the day were found to affect serum TSH significantly but did not affect fT4 (46). Age-specific serum fT4 was not discussed when thyroid diseases in older adults were studied, which may be a limitation but may not have strongly influenced the results.
The current study has some limitations. This is a cross-sectional study, and the study subjects were not followed longitudinally. Additionally, the oldest population (at least 80 years of age) accounted for a small proportion, and further analyses were not conducted on these individuals.
It is concluded that the serum TSH level increases in older people, and the use of an age-specific serum TSH reference range for the diagnoses of thyroid diseases in older adults is recommended.
Footnotes
Acknowledgments
This work was supported by the International Cooperation Foundation of the Ministry of Health of the People's Republic of China (2009); the Guanghua Science and Technology Foundation of China (grant 2007-02); the Research Foundation of Innovative Team in Advanced Educational Institute (grant LT201215); the Foundation of Science and Technology for Universities in Liaoning Province; and the Foundation for The Key Laboratory in Liaoning Province (2010).
Author Disclosure Statement
The authors have no potential conflicts of interest to declare.