
Abstract
Background:
Patients undergoing thyroidectomy may have inadvertent damage or removal of the parathyroid gland(s) due to difficulty in real-time parathyroid identification. Near-infrared autofluorescence (NIRAF) has been demonstrated as a label-free modality for intraoperative parathyroid identification with high accuracy. This study presents the translation of that approach into a user-friendly clinical prototype for rapid intraoperative guidance in parathyroid identification.
Methods:
A laboratory (lab)-built spectroscopy system that measures NIRAF in tissue was evaluated for identifying parathyroid glands in vivo across 162 patients undergoing thyroidectomy and/or parathyroidectomy. Based on these results, a clinical prototype called PTeye was designed with a user-friendly interface and subsequently investigated in 35 patients. The performance of the lab-built system and the clinical prototype were concurrently compared side by side by a single user with 20 patients in each group. The influence of (i) intrapatient and interpatient variability of NIRAF in thyroid and parathyroid glands and (ii) thyroid and parathyroid pathology on intraoperative parathyroid identification were investigated. The effect of blood on NIRAF intensity of parathyroid and thyroid was tested ex vivo with the PTeye system to assess if a hemorrhagic surgical field would affect parathyroid identification. Accuracy of both systems were determined by correlating the acquired data with either visual confirmation by a surgeon for unexcised parathyroid glands or histology reports for excised parathyroid glands.
Results:
The overall accuracy of the lab-built system in guiding parathyroid identification was 92.5%, while the PTeye system achieved an accuracy of 96.1%. Unlike the lab-built system, the PTeye could guide parathyroid identification even as the operating room lights remained on and required only 25% of the laser power used by the lab-built setup. Parathyroid glands had elevated NIRAF intensity compared to thyroid and other neck tissues, regardless of thyroid or parathyroid pathology. Blood did not seem to affect tissue NIRAF measurements obtained with both systems.
Conclusion:
In this study, the clinical prototype PTeye demonstrated high accuracy for label-free intraoperative parathyroid identification. The intuitive interface of the PTeye that can guide in identifying parathyroid tissue in the presence of ambient room lights suggests that it is a reliable and easy-to-use tool for surgical personnel.
Introduction
A
Existing methods for identifying parathyroid glands include ultrasound, sestamibi scintigraphy, computed tomography, and magnetic resonance imaging (12,13). These current modalities for localizing parathyroid glands are limited in their sensitivity, rendering them inadequate to prevent surgical complications (9). These techniques are primarily utilized for preoperative localization of an enlarged, hyperfunctioning parathyroid gland(s) and cannot be used to find a normal gland (prior or during thyroidectomy). Intraoperative parathyroid hormone (IOPTH) assays are often performed during parathyroidectomies to confirm removal of the hyperactive parathyroid glands (14 –16). However, this technique is typically not performed during routine thyroidectomy, as it increases surgery time by 20–30 minutes and does not indicate which gland is compromised (12). Thus, there is a clear need for a highly sensitive, real-time tool for identifying parathyroid glands regardless of its disease state, allowing for more effective patient management.
The potential for optical techniques as a noninvasive, real-time automated tool for tissue diagnostics has already been established in various studies (17 –21). Several groups have utilized optical techniques for parathyroid gland detection that include the application of contrast agents (22 –24), optical coherence tomography (25 –27), and diffuse reflectance imaging (28) with limited success. Others have applied autofluorescence spectroscopy to detect parathyroid malignancies as well (29,30). Paras et al. demonstrated for the first time that near-infrared autofluorescence (NIRAF) can be potentially utilized for label-free identification of the parathyroid glands, regardless of its disease state (31). These findings were further investigated by McWade et al. where the potential of NIRAF-based parathyroid identification was validated with an overall accuracy of 97% (32). Since the emergence of these studies, several other groups have tapped on the potential of NIRAF to localize healthy and/or diseased parathyroid glands (33 –35).
As the effectiveness of NIRAF-based parathyroid identification has been clearly established in the aforementioned studies, it is essential to successfully translate this optical technique into a simple, easy-to-use intraoperative tool for real-time guidance in parathyroid identification. The data output of the lab-built system as described in our earlier studies (31,36), presents NIRAF as spectral data which may not be easily interpreted by surgeons, residents or surgical first assistants. Moreover, since operation room (OR) lights interfere with NIRAF detection, OR lights need to always be turned off. This can cause frequent interruptions to the surgical workflow while using the lab-built system or other contemporary NIRAF-based modalities for parathyroid identification/localization. It thus becomes imperative to translate this system for optimal ease of use inside the OR without disrupting the routine surgical workflow during a thyroidectomy/parathyroidectomy. Simultaneously the device should possess high accuracy in real-time, noninvasive, label-free parathyroid identification. A clinical prototype called PTeye (AIBiomed Inc., Santa Barbara, CA, and Vanderbilt University, Nashville, TN) has been developed on the same principle of NIRAF-based parathyroid detection as utilized earlier in the lab-built system (31,36). The PTeye has been designed for optimum functionality in presence of ambient OR lights and is equipped with a user interface that is meant to be intuitive in aiding the surgeon for in vivo parathyroid identification. In this study, we have evaluated and compared the performance between the newly developed clinical prototype PTeye and the existing lab-built system (31,36), in accurately identifying the parathyroid gland(s) in vivo during thyroidectomy and parathyroidectomy. This study was designed to determine the equivalence of the PTeye and the lab-built system for real-time parathyroid identification. Moreover, this study aimed at investigating pertinent factors that could affect NIRAF-based parathyroid identification such as (i) intrapatient and interpatient variability, (ii) effect of thyroid and/or parathyroid disease, and (iii) influence of blood in the surgical field.
Materials and Methods
Instrumentation
Instrumentation of the lab-built system
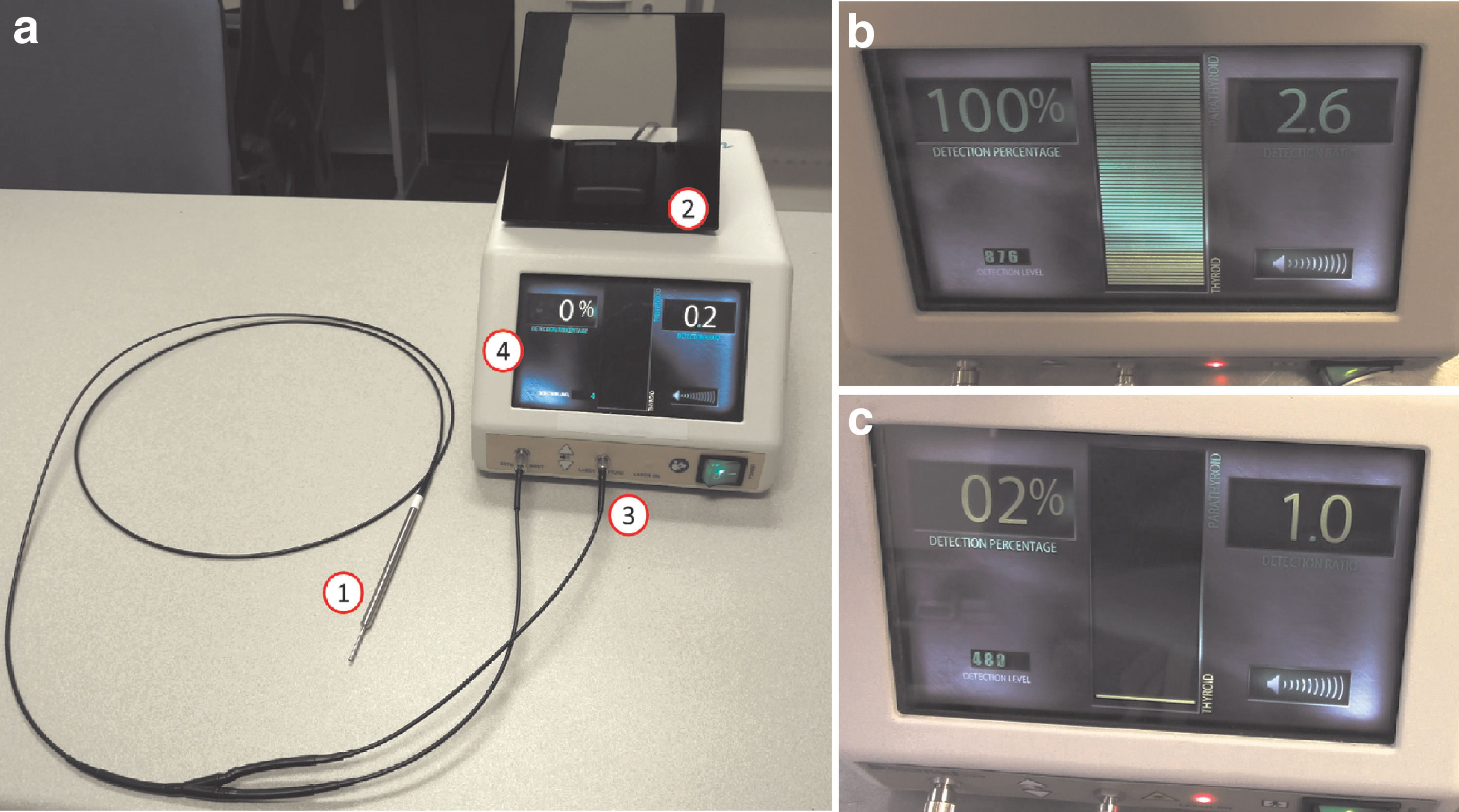
As described in earlier studies (31,36), the system consists of (i) a spectrometer (S2000-FL; Ocean Optics, Dunedin, FL), (ii) a 785-nm diode laser (I0785SL0050PA; IPS, Monmouth Junction, NJ), (iii) a custom-made fiber optic probe and (iv) a laptop computer (Fig. 1). Tissue NIRAF signal acquisition with the lab-built system is computer controlled by a customized software developed in LabView (National Instruments, Austin, TX). The fiber optic probe delivers laser light to the tissue site and simultaneously collects the corresponding NIRAF signal from the site. The detachable fiber optic probe is reusable after sterilization with ethylene oxide or Sterrad 100NX. The NIRAF signal obtained by the spectrometer is relayed to the laptop and displayed as a spectrum via the LabView software. The fiber optic probe irradiates tissue with 80 mW of light using a 400 μm spot size at an integration time of 300 milliseconds per measurement.

The lab-built system for near-infrared autofluorescence (NIRAF) detection in tissue. The components involve (
Instrumentation of the clinical prototype – the PTeye
The PTeye incorporates the same point detection technology as the aforementioned lab-built system, with a few exceptions such as using an internal microprocessor board instead of an external laptop computer. The PTeye system encases a 785 nm laser source and the detector, unlike the lab-built system, where the laser source and spectrometer are separate external components. The attachables for the PTeye system (Fig. 2a) consists of (i) the fiber optic probe, (ii) a foot-pedal for device activation, and (iii) a power supply adapter. The fiber optic probe of the PTeye can also be detached and sterilized akin to that of the lab-built system. For tissue assessment, the fiber optic probe is activated by pressing the foot-pedal, which allows the laser light to reach the tissue site through the probe. The NIRAF signal from the tissue is then relayed through the fiber probe itself to the detector within the PTeye system. The internal circuitry between the detector and the laser source are uniquely designed to allow tissue NIRAF detection without inteference from ambient OR light. The NIRAF signal obtained by the detector is analyzed by the internal microprocessor board. The processed outcome is conveyed through internal circuitry as (i) visual output to the display panel and (ii) auditory feedback to the loudspeaker, both of which constitute the distinct user interface of the PTeye. The display panel (see Fig. 2b and 2c) informs the user on the absolute NIRAF intensity, displayed as “Detection Level,” and tissue NIRAF normalized to the thyroid NIRAF, denoted as “Detection Ratio.” Based on NIRAF values and calculated ratios, the PTeye's degree of confidence on the suspect tissue being parathyroid is further expressed as “Detection Percentage.” In parallel, the auditory feedback is initiated once the “Detection Ratio” exceeds 1.2, the minimal detection ratio set for parathyroid identification. It must be noted that the PTeye probe delivered the laser light at a power of 20 mW over a spot size of ∼400 μm. A comparison between the instrumentation of the lab-built system and the PTeye is summarized in Table 1.
(
NIRAF, near-infrared autofluorescence; OR, operation room.
Intraoperative device testing for guidance in parathyroid identification
This study consisted of individuals (18–99 years of age) who presented at the Vanderbilt Endocrine Surgery Center for thyroidectomy and/or parathyroidectomy. Patient eligibility was evaluated by the attending surgeon during preoperative assessment at the Vanderbilt University Endocrine Surgery Center. Standard two-sample Student's t-test was used to estimate the minimum sample size required, assuming that the effect size and variance in enrolled patients will be comparable to an earlier study by McWade et al. (32). For a power of at least 99% and a level of significance of 1%, a minimum sample size of at least 20 patients was required per group for comparison between the lab-built system and the PTeye system. Evaluation of both systems involved independent device testing with four endocrine surgeons: three for the lab-built system and two for the PTeye.
Testing with the lab-built system
A total of 162 patients were consented for testing with the lab-built system to determine the device accuracy as described in earlier studies (31,36,37). Written informed consent was obtained from all patients enrolled in the study that was approved by the institutional review board (IRB) of Vanderbilt University (IRB No. 070795). After switching off the OR lights, initial testing steps included recording background measurements with the laser turned off prior to each tissue measurement. Following this, three spectra were collected per tissue site with the OR lights remaining off, with approximately 300 milliseconds taken per spectrum. The first set of measurements routinely involved five measurements on random thyroid sites for establishing a thyroid baseline for NIRAF. Upon testing the lab-built system in the recruited patients, 485 parathyroid measurements (369 parathyroid glands) and 643 nonparathyroid measurements (thyroid, fat, neck muscles, and trachea sites) were acquired. The surgeon remained blinded to the NIRAF spectral data acquired.
Testing with the clinical prototype PTeye
Thirty-five patients were consented for the study approved by Vanderbilt IRB (IRB No. 141648) using the clinical prototype PTeye. The OR lights remained on during measurements with the PTeye device. The entire process per measurement was in real-time, taking less than two seconds. In each patient, a thyroid baseline for NIRAF baseline was first obtained by recording five measurements on random sites of the thyroid as described earlier with the lab-built system. Subsequent tissue NIRAF measurements in the patient were normalized to this baseline thyroid value and expressed as a NIRAF ratio. In this study, bias of surgeon's judgement was avoided by muting the audio feedback and turning the PTeye display panel away from the surgical team, being visible only to the investigator during all patient measurements. We obtained 201 parathyroid measurements (96 parathyroid glands) and 314 nonparathyroid measurements (thyroid, fat, neck muscle and trachea sites) using the PTeye system.
Parallel testing of lab-built system and clinical prototype with a single user
Forty patients were randomly consented for the study approved by Vanderbilt University for testing with the lab-built system (IRB No. 070795) and the clinical prototype PTeye system (IRB No. 141648). Each group consisted of 20 patients, and both devices were tested by a single surgeon who was blinded to the system output. Testing was performed to compare performance between the two systems with a single user. Patients evaluated with the lab-built system yielded 140 parathyroid, 103 thyroid, 42 fat, 47 neck muscle, and 48 tracheal measurements, while 120 parathyroid, 66 thyroid, 40 muscle, 40 fat, and 40 tracheal measurements were obtained from patients investigated with the PTeye system.
Estimating the effect of blood on thyroid and parathyroid specimen measurements ex vivo
Three fresh frozen specimens each of normal thyroid and parathyroid adenoma were obtained from the Co-operative Human Tissue Network (Vanderbilt University Medical Center, Nashville, TN). After thawing the specimens, at least six NIRAF measurements were obtained per specimen ex vivo. To simulate a hemorrhagic surgical field of view, 0.5 mL of heparinized murine blood was ejected onto the specimen surface. NIRAF intensity of the specimens determined by the lab-built system and PTeye were normalized to thyroid NIRAF and grouped into four categories: (i) thyroid without blood, (ii) thyroid with blood, (iii) parathyroid without blood, and (iv) parathyroid with blood, with each group consisting of 18 NIRAF measurements Statistical significance between the four groups was determined by a two-tailed Student's t-test for unequal variance, with p < 0.01 considered significant.
Data analysis and validation with both devices
For the lab-built system, NIRAF spectra were processed using MATLAB (Mathworks Inc., Natick, MA) as described earlier (31,36). After subtracting background noise, NIRAF intensity at 820 nm was quantified from spectra of various tissue sites. Tissue NIRAF intensities in each patient was then normalized to the NIRAF intensity of the thyroid at 820 nm in that patient, which yields the NIRAF ratio for each tissue site. In comparison, the PTeye system data—the absolute NIRAF intensity and the NIRAF ratios—that appeared on the display panel was noted manually for each tissue site in individual patients and compiled specifically.
For both systems, a NIRAF ratio above 1.2 was considered positive for parathyroid identification. Normalized NIRAF intensity (NIRAF ratios) for both systems were correlated with either (i) the surgeon's visual identification of the in situ parathyroid, (ii) the histology report of the excised parathyroid glands, or (iii) a combination for both in situ and excised glands. Sensitivity, specificity, false positive rate, false negative rate, positive predictive value (PPV), negative predictive value (NPV), overall accuracy and kappa-value were accordingly calculated for both systems and compared. Statistical significance in normalized NIRAF intensities between thyroid, parathyroid, fat, muscle, and trachea were determined using a two-tailed Student's t-test for unequal variance, where a p-value <0.01 was considered significant. The same statistical approach was adopted to determine if there was a significant difference between NIRAF measured from normal and diseased thyroid or parathyroid glands. Fischer two-sample test for variance was utilized to determine if the variance of demographic variables such as age and body mass index was significantly different between the patients tested with the lab-built system and those with the clinical prototype PTeye system. A chi-squared test was applied similarly for categorical variables such as sex, race/ethnicity, and disease types between the two groups.
Results
Patient demographics
A total of 197 patients were recruited (Table 2): 162 patients were tested with the lab-built system, while the other 35 patients were evaluated with the PTeye. Distribution based on age, body mass index, sex, race/ethnicity, and disease were found to be comparable with no significant difference in between the patients enrolled for the lab-built system and the clinical prototype PTeye system.
Performance of lab-built system
Upon analyzing normalized NIRAF intensity of tissues obtained with the lab-built system in 162 patients, parathyroid glands were measured to have the highest values among the evaluated tissues, followed by the thyroid glands with minimal values being detected in fat, neck muscles and trachea (see Fig. 3). On an average, normalized NIRAF intensity for parathyroid was found to be significantly higher than that for the thyroid and other neck tissues (p-value = 1.33 × 10–32). The lab-built system identified parathyroid glands (both in situ and excised) with 89.1% sensitivity (448/503 parathyroid measurements) and 95.2% specificity (612/643 nonparathyroid measurements). Overall accuracy attributed for parathyroid identification was 92.5% (kappa = 0.85) with 4.8% false positive rate and 11.9% false negative rate as indicated in Table 3. The PPV stood at 93.5%, while NPV was determined to be 91.8% for the lab-built system.
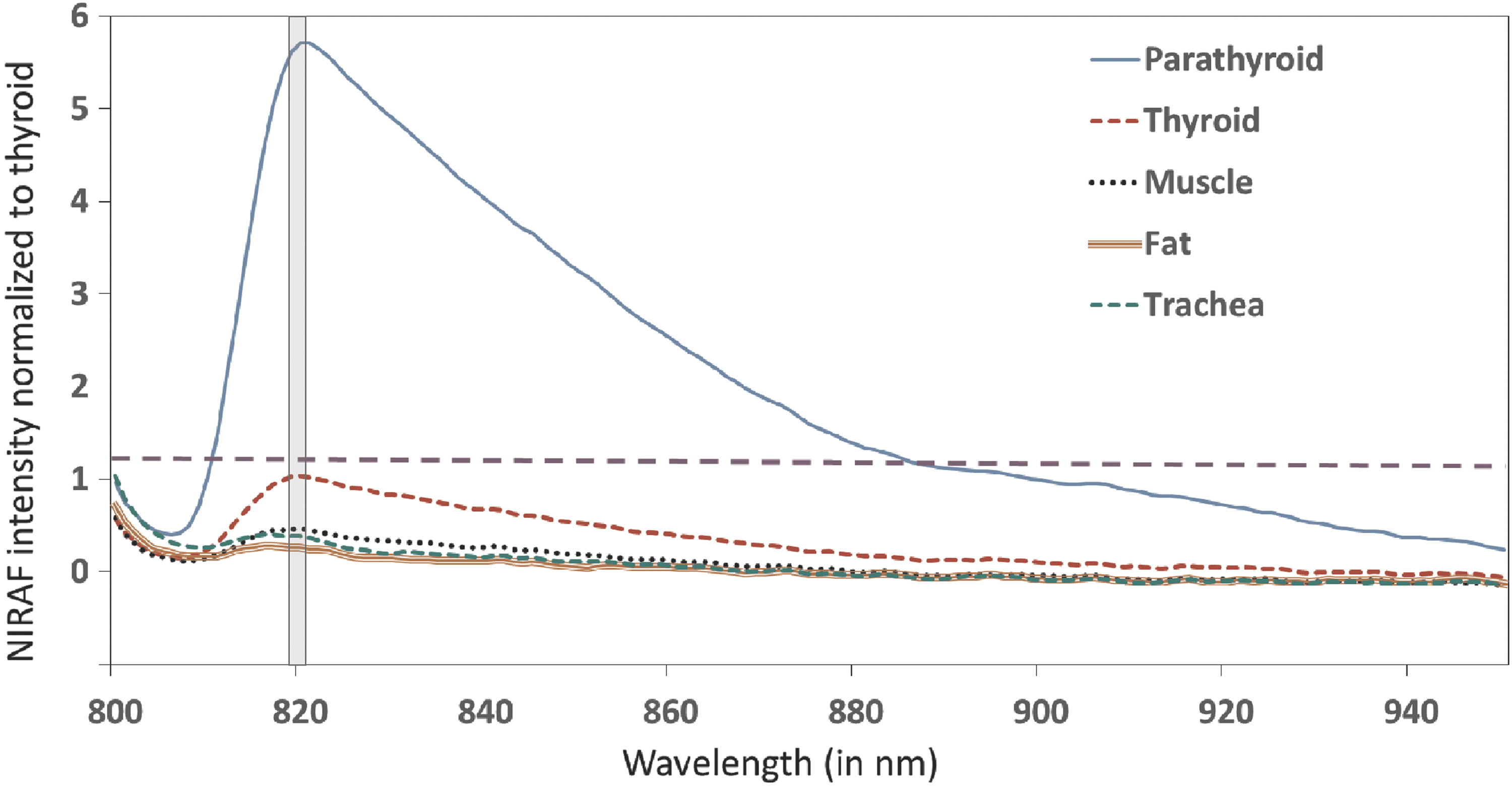
Averaged NIRAF intensity normalized to thyroid obtained with the lab-built system in 162 patients for thyroid, parathyroid, fat, neck muscles and trachea. Tissues were classified based on NIRAF intensity at 820 nm (indicated by grey zone) as parathyroid or nonparathyroid by setting a threshold at 1.2 denoted by the dashed purple line.
Device NIRAF+ or NIRAF− indicates device positive or negative for parathyroid.
r-SHP, renal failure-induced secondary hyperparathyroidism.
When data of the lab-built setup were evaluated separately for in situ tissues based on the surgeons' visual assessment (with high/moderate confidence), a 91.8% accuracy (kappa = 0.83) was achieved. The lab-built system performed better by yielding 95.0% accuracy (kappa = 0.91) in identifying parathyroid glands that were later excised and validated with histology. An earlier study had found that renal-induced secondary hyperparathyroidism (r-SHP) patients tend to have elevated NIRAF intensities in parathyroid glands only sporadically (32). Therefore, upon eliminating the five r-SHP cases from the lab-built system dataset, the accuracy of the lab-built system for excised glands improved further to 96.9% (kappa = 0.94) when validated with histology. Upon excluding r-SHP cases, the overall accuracy of lab-built system for parathyroid gland identification (both in situ and excised) increased slightly to 92.7% (kappa = 0.85).
Performance of the clinical prototype system, PTeye
Normalized NIRAF intensity measured from parathyroid glands with the PTeye system in 35 patients was significantly higher than that of the thyroid and the other tissues in neck such as fat, muscle and trachea (p-value = 1.07 × 10−40), following a similar trend as obtained with the lab-built system in 162 patients (Fig. 4). As reported in Table 3, the PTeye was capable of identifying parathyroid glands (in situ and excised) with 95.5% sensitivity (192/201) and 96.5% specificity (303/314). Parathyroid identification with the PTeye system had an overall accuracy of 96.1% (kappa = 0.92) with 3.5% false positive rate and 4.5% false negative rate. The PPV and NPV for this system were 94.6% and 97.1% respectively. Validating the PTeye measurements for only in situ tissues with the surgeons' visual assessment yielded 97.4% accuracy (kappa = 0.96). When corroborated with histology for excised tissues, the device obtained an accuracy of 90.7% (kappa = 0.81), that improved further to 95.4% (kappa = 0.91) upon excluding the one r-SHP patient assessed with the PTeye. By discounting the sole r-SHP case, the overall accuracy of PTeye for parathyroid gland identification (both in situ and excised) rose further to 97.3% (kappa = 0.95). It must be further considered that this performance of the PTeye system in identifying parathyroid tissue was achieved despite presence of ambient OR lights.

Comparison of normalized NIRAF intensity obtained with the lab-built system in 162 patients and the PTeye in 35 patients for thyroid, parathyroid, fat, neck muscles, and trachea. NIRAF intensity has been normalized to that obtained by the thyroid. **p < 0.001 for normalized NIRAF intensity of parathyroid compared with other neck tissues such as thyroid, fat, muscles, and trachea. Horizontal line in blue box, data median; upper tail, data maxima; lower tail, data minima; red crosses, data outliers.
Parallel comparison of the lab-built system and PTeye upon testing with a single user
Upon concurrent testing of both systems with a single user, the lab-built system achieved 90.7% sensitivity and 90.9% specificity. In this parallel study, the lab-built system achieved 90.8% accuracy in parathyroid identification (kappa = 0.81) with 9.1% false positive rate and 9.3% false negative rate. The PPV and NPV was found to be 85.2% and 94.4% respectively for the lab-built system. In comparison, the PTeye device performed with a 100% sensitivity and 96.2% specificity, leading to an overall accuracy of 97.7% (kappa = 0.95) with 3.8% false positive rate and 0% false negative rate. The PPV and NPV for the PTeye were 94.5% and 100% respectively for the PTeye in this single user comparison. The performance comparison between both systems is summarized in Table 4.
Number of measurements at different locations on parathyroid or nonparathyroid tissues.
Intrapatient and interpatient variability of NIRAF in parathyroid and thyroid tissues
Among the 35 patients tested with the PTeye, no parathyroid glands were seen by the surgeon in patient 4, while patients 17 and 26 had no thyroid remnants visible due to previous thyroid interventions. Intrapatient variability of normalized NIRAF in the thyroid ranged from 7.9 to 94.2% (mean = 28.7%), while that of the parathyroid gland(s) varied between 12% and 74% (mean = 35.2%). When the interpatient variability was analyzed as the deviation of individual patient NIRAF from the mean calculated across all patients expressed as a percentage, the interpatient variability for normalized NIRAF in thyroid was 30.4%. In comparison, the mean interpatient variability for normalized NIRAF in parathyroid gland(s) was about three times higher at 92.9%. Despite the higher intrapatient and interpatient variability, normalized NIRAF intensities for parathyroid glands were consistently higher than that of the thyroid glands across most patients, except patient 29, an r-SHP patient, as seen in Fig. 5. It should be noted that in cases where there were no visible thyroid remnants such as in patients 17 and 26, NIRAF intensities were normalized to neck muscles instead of the thyroid.
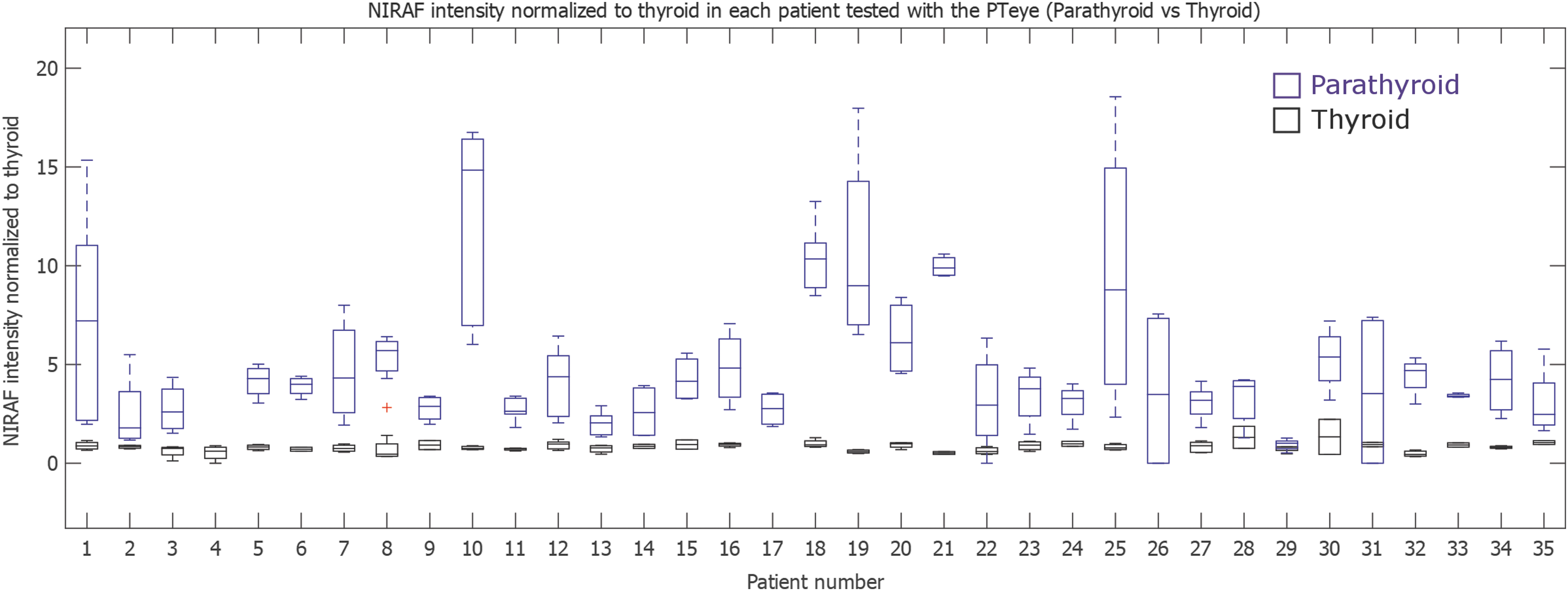
Intrapatient and interpatient variability of normalized NIRAF intensity in parathyroid and thyroid in the 35 patients assessed with the PTeye. No parathyroid glands could be visualized by the surgeon in patient 4, leading to lack of parathyroid measurements. Patients 17 and 26 were postthyroidectomy cases who underwent parathyroidectomy during this study; the NIRAF intensity were normalized to the neck muscle, instead of the thyroid for these cases. Patient 29 was the only renal-induced secondary hyperparathyroidism case assessed with the PTeye. Horizontal line in boxes, data median; upper tails, data maxima; lower tails, data minima; red crosses, data outliers.
Effect of thyroid and/or parathyroid pathology on NIRAF intensity assessed by the lab-built system and the PTeye
As seen in Table 2, patients evaluated with the lab-built system consisted of 39 subjects with non-toxic benign thyroid disease (nontoxic solitary/multinodular goiter/Hashimoto's thyroiditis), 25 with thyrotoxic benign thyroid disease (Graves' disease/toxic multinodular goiter/thyroiditis), 32 with malignant thyroid disease (papillary carcinoma/follicular carcinoma), 48 with primary hyperparathyroidism, 5 with renal-induced secondary hyperparathyroidism (r-SHP), 2 with tertiary hyperparathyroidism, and 11 with concurrent thyroid–parathyroid disease. Patients assessed with the PTeye system included 9 subjects with nontoxic benign thyroid disease, 5 with toxic benign thyroid disease, 4 with malignant thyroid disease, 13 with primary hyperparathyroidism, 1 with r-SHP, and 3 with concurrent thyroid–parathyroid disease. Parathyroid tissue exhibited significantly higher normalized NIRAF intensity as compared to the thyroid gland, irrespective of parathyroid or thyroid disease state for both the lab-built system (p < 0.001) and the PTeye (p < 0.001) as observed in Figure 6.

Variation of normalized NIRAF intensity between normal thyroid, diseased thyroid, normal parathyroid, and diseased parathyroid states among 162 patients tested with the lab-built system and 35 patients tested with the PTeye. **p < 0.001 for normalized NIRAF intensity of parathyroid compared with thyroid. Horizontal line in blue box, data median; upper tails, data maxima; lower tails, data minima; red crosses, data outliers.
Performance of both systems in cases of renal failure induced secondary hyperparathyroidism
Normalized NIRAF intensities of the parathyroid gland(s) in r-SHP patients were frequently found to be lower than 1.2 (the threshold set for parathyroid identification), in contrast with healthy and other types of diseased parathyroid gland(s). This finding was consistent in patients evaluated with the lab-built system and the PTeye. Among the 5 r-SHP patients evaluated with the lab-built system, 15 out of 21 measurements from different parathyroid locations had a normalized NIRAF intensity >1.2. In comparison, only 1 out of 8 measurements in parathyroid glands within the sole r-SHP patient tested with PTeye yielded an elevated normalized NIRAF intensity. The sensitivity of parathyroid identification with the lab-built system and the clinical prototype system is notably improved at 95.8% (92/96 parathyroid measurements) and 97.3% (73/75 parathyroid measurements) respectively when validated with histology for excised glands, if patients with r-SHP were excluded from performance analysis for both devices.
Effect of blood on NIRAF on thyroid and parathyroid specimens ex vivo
The influence of blood on intraoperative parathyroid identification with the lab-built and PTeye systems was studied with an ex vivo simulated experiment using thyroid and parathyroid specimens covered with heparinized murine blood. The findings as illustrated in Figure 7 indicate that the parathyroid specimens were found to have NIRAF intensity significantly higher than the thyroid, regardless of the presence of blood on the parathyroid or the thyroid (p < 0.001).
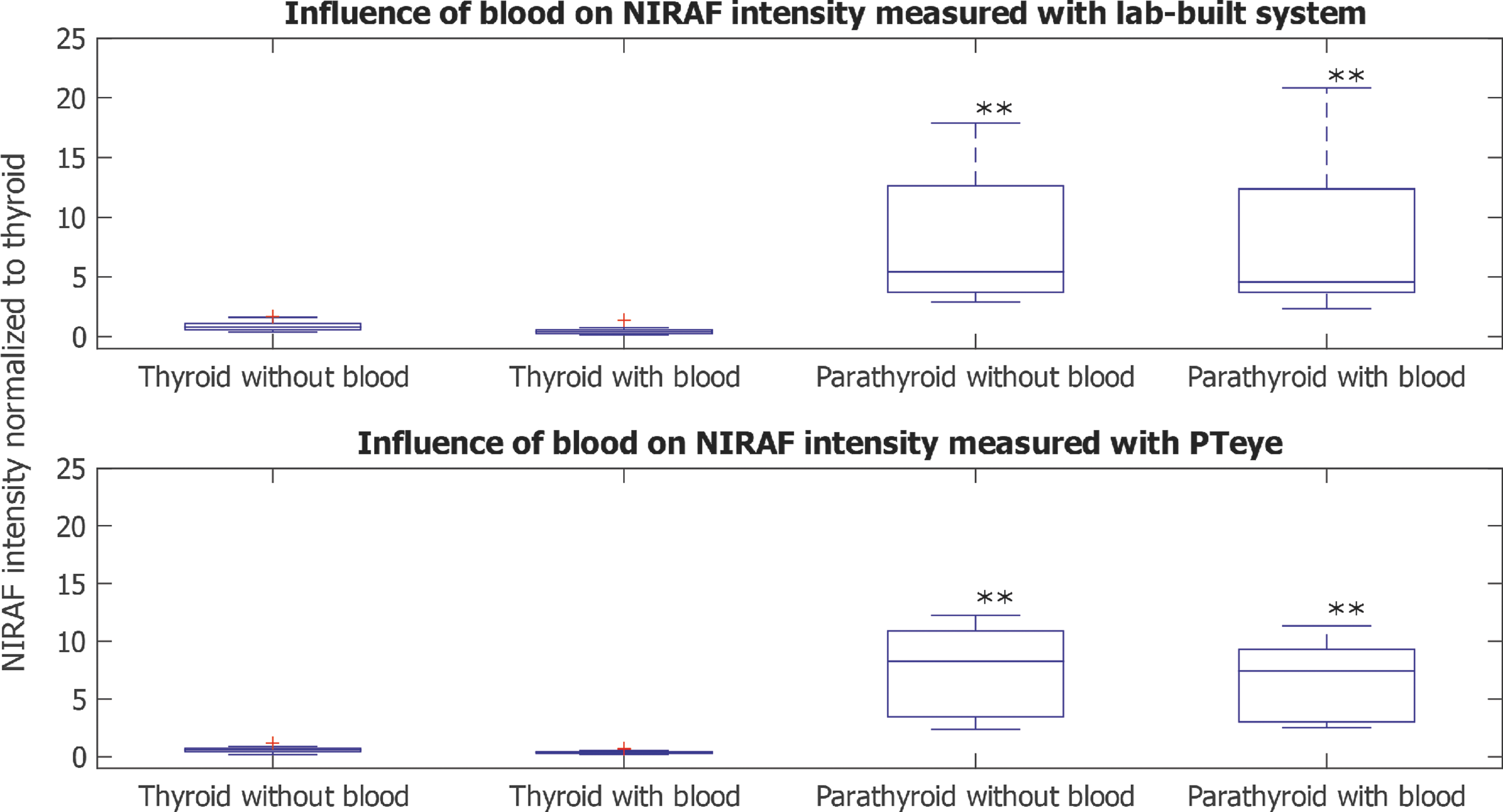
Influence of blood on NIRAF intensity measured ex vivo from thawed frozen human parathyroid and thyroid specimens with the lab-built system and the PTeye. **p < 0.001 for NIRAF intensity of parathyroid compared with thyroid. Horizontal line in blue box, data median; upper tails, data maxima; lower tails, data minima; red crosses, data outlier.
Discussion
In this study we tested a clinical prototype called PTeye for real-time, label-free intraoperative guidance in parathyroid identification using NIRAF and compared its performance with a lab-built system. Our findings reported here suggest that the PTeye performed comparably with the lab-built system, with the accuracy of the latter having already been validated earlier (31,32,36,37). Despite higher intrapatient and interpatient variability, the normalized NIRAF intensity of the parathyroid detected by the PTeye stayed consistently higher than that of the thyroid by at least a factor of 1.2, regardless of thyroid and/or parathyroid pathology or presence of blood. An important exception was however observed in renal-induced secondary hyperparathyroidism (r-SHP) patients evaluated with both devices. The overall findings of this study demonstrate the clinical readiness of the PTeye for intraoperative parathyroid identification, as it is equipped with (i) an interface that can be easily interpreted by surgeons and (ii) the ability to function with ambient OR lights, causing minimal interference to routine thyroidectomy/parathyroidectomy procedures.
Demonstrable equivalence of the PTeye with the lab-built system
The PTeye was found to have an overall accuracy of 96.1% for guidance in real-time intraoperative parathyroid identification, which is comparable to the performance of the original lab-built instrument tested in this study and validated earlier with an accuracy as high as 97% (32,36,37). Normalized NIRAF intensity for the parathyroid as detected by the PTeye was greater than that of the thyroid, while fat, muscle, and trachea exhibited minimal NIRAF as seen in Figure 4 and also observed by Paras et al. (31). Upon comparing the performance of the lab-built system and the PTeye, the former scored a 92.5% accuracy when compared with the latter that achieved a 96.1% accuracy. This trend was noted again when both the systems were evaluated side by side by a single user, as the PTeye demonstrated 100% sensitivity in parathyroid identification (120/120) in 20 patients, while the sensitivity reported with the lab-built system was 90.7% (127/140) in an equivalent set of 20 patients. Appropriate probe positioning is essential for NIRAF measurements with the lab-built system and the sensitivity may have been affected potentially due to the optical probe occasionally slipping from measurement tissue site when the OR lights were switched off. This disadvantage is annihilated with the PTeye system as the OR lights remain on and the surgeon can clearly confirm that the probe is in a steady position over the tissue during NIRAF measurements, leading to a higher sensitivity. It must be noted, though, that when the devices were validated exclusively with histology of excised parathyroid glands, the lab-built system and the PTeye provided an accuracy of 95.0% and 90.7% respectively. A drop in the performance accuracy of PTeye with excised glands may be attributed to irregular NIRAF levels in r-SHP patients which has also been reported earlier (32). Excluding data from r-SHP patients for both systems then provided comparable accuracy for both lab-built system and PTeye at 96.9% and 95.4% respectively.
Upon comparing the results acquired with the lab-built system and the PTeye (Figures 4 and 6), in addition to results obtained with the lab-built system earlier (31,32,36,37), it can be clearly demonstrated that the clinical PTeye performs comparably to the already validated lab-built system. Furthermore, the PTeye is able to achieve this comparable performance by requiring 20 mW, which is only 25% of the laser power that was typically being used by the lab-built system. In addition to its intuitive user interface, one of the distinct features of the PTeye is its ability to remain functional for parathyroid identification in presence of ambient OR lights. This aspect is particularly beneficial for the surgeon, as turning the OR lights on or off for NIRAF measurements of the parathyroid with the lab-built system was often disruptive to the tempo and flow of the surgery. With optimal functionality in ambient OR lights and real-time NIRAF measurements, use of the PTeye system can be easily implemented into the workflow of routine thyroidectomy and parathyroidectomy procedures.
Indications for use of the PTeye and further steps for clinical translation
The PTeye is ultimately indicated for surgical guidance to aid in identifying parathyroid gland(s) in real time, regardless of whether the gland is normal or diseased, based on results demonstrated in Figures 4 –6. The PTeye can also be used for effectively detecting parathyroid gland(s) in a hemorrhagic surgical field, as demonstrated in this study that blood has no effect on the NIRAF intensity of parathyroid or thyroid tissue (Figure 7). It must be noted that the effect of blood was investigated ex vivo on fresh frozen specimens with heparinized murine blood and may not be completely representative of parathyroid identification in vivo within a hemorrhagic surgical field. In a standard thyroid/parathyroid surgery, estimated blood loss is typically less than 50 mL, making the impact of intraoperative hemorrhage likely negligible. Although thicker blood clots could potentially obstruct NIRAF signal from underlying parathyroid gland(s), adequate irrigation of the surgical field can ensure optimal NIRAF measurements from parathyroid tissue candidates.
Currently the PTeye is a handheld probe-based system that relies on point-based measurements and thus cannot aid in spatially mapping the parathyroid within the surgical field. Our group had earlier implemented a NIRAF imaging device to view the entire surgical field and localize the parathyroid with 100% accuracy (37), which was further explored by other research groups (34,35,38,39). Commercially available NIRAF imaging systems described in the aforementioned studies typically utilize a camera that detects NIR signal, which enables the surgeon to visualize the parathyroid gland on a remote display monitor. In contrast, the PTeye is a device with a handheld probe, an internal NIR detector, and a console monitor that simultaneously displays the tissue probability of being parathyroid in real time, with accompanying auditory feedback. The innate differences between the instrument design of NIRAF imaging devices and a handheld fiber-optic probe system like the PTeye endow both types of systems with an unique share of advantages and disadvantages. While wide-field NIRAF imaging systems are advantageous in providing spatial information without requiring tissue contact, it is extremely sensitive to ambient OR lights. Acquiring NIRAF images would thus require remote darkness in the OR that can impede surgical workflow. Parathyroid NIRAF intensity could also notably fluctuate depending on the height of the NIR camera held by the surgeon above the surgical field which may affect parathyroid gland visualization from the acquired NIRAF images. These imaging systems may further require neck incisions to be wider to properly visualize deep seated parathyroid glands. As a result, imaging with these systems can be challenging if the parathyroid glands are situated at aberrant or deeper lying zones—such as retro-esophageal sites—that are not easily accessible or visualized by the NIR camera. In contrast, the PTeye allows the surgeon to position the probe onto these difficult sites in the presence of ambient OR lights and reach the suspect tissue to obtain NIRAF measurements. The inability of PTeye to spatially visualize parathyroid gland(s) stems from the fact that PTeye was designed to be a simple and compact portable device that fits on a desk (Fig. 2a) as compared with wide-field NIRAF imaging systems. The suitability for either system would eventually depend on ease of use as dictated by the surgeon's preference and experience.
Since NIR wavelengths can only penetrate down to a depth of few millimeters, it could be challenging to detect NIRAF signal from deeply situated parathyroid as in an intrathyroidal location or buried under a layer of fat. Due to this limitation, PTeye cannot aid the surgeon in localizing a “missing” parathyroid. Moreover, the ability to localize a deeply situated parathyroid gland, heavily depends on the thickness, optical property and NIRAF intensity of tissue above it (thyroid, fat, or muscle) compared with that of the underlying parathyroid itself. The possibility of using NIRAF to localize a parathyroid gland below a layer of fat would be more feasible than a parathyroid gland under thyroid tissue. This is primarily because thyroid tissue tends to have higher NIRAF intensity than fat (Fig. 3) and different optical property, which can conceal the NIRAF intensity of the underlying parathyroid gland to a greater degree. While Kim et al. have demonstrated the potential to detect parathyroid glands that were located below fibrofatty layers, the study did not describe how thick those layers were (33). A more controlled study is thus mandatory for assessing depth-related NIRAF detectability from parathyroid gland(s). Based on our current findings, the PTeye should not be applied for localizing a “missing” parathyroid and be solely used as an aid for parathyroid identification only after the suspect tissue has been visualized and adequately exposed by the surgeon. Ultimately the ability to locate a “missing” parathyroid gland rests on the skill, knowledge, and experience of the surgeon, regardless of the parathyroid imaging/detection modality used.
Another limitation of NIRAF-based modalities like the PTeye is that while it can identify parathyroid tissues with high accuracy, it does not inform the surgeon about the vascularity/viability of the visualized parathyroid gland. Surgeons still tend to rely on their visual skills/experience to assess parathyroid perfusion/viability, although optical modalities such indocyanine green–based NIR fluorescence (40,41) and label-free laser speckle imaging (42) have recently demonstrated potential for objective assessment of parathyroid viability. For concurrent identification of parathyroid glands and evaluation of its viability, NIRAF-based devices such as the PTeye may need to be used complementarily with the aforementioned techniques.
Our study further reveals that while PTeye is associated with a comparatively low false positive rate of 3.5% and false negative rate of 4.5%, there is a need for appropriate risk mitigation strategies. This is mandatory to ensure that there is no additional risk imposed onto the patient upon utilizing the PTeye. In the rare occasions where the surgeon disagrees with the information provided by the PTeye, frozen biopsy section analysis and/or IOPTH assays could be performed to minimize risk from false positives and/or negatives. The applicability of these techniques would depend on (i) whether a thyroidectomy or a parathyroidectomy is being performed and (ii) whether thyroidectomy is associated with additional lymph node dissection. During surgeries for benign thyroid conditions, if the surgeon left behind thyroid/fat/lymph node tissue, assuming it was a parathyroid gland as denoted by the PTeye (false positive), patient outcomes remain unaffected. More caution needs to be exerted for surgeries of thyroid malignancies with extensive lymph node dissection. In such situations, the surgeon should ideally send frozen sections of the tissue, even when indicated as ‘parathyroid positive’ by PTeye. With such an approach, the surgeon minimizes the risk of leaving behind residual malignant thyroid tissue or metastatic lymph nodes, while simultaneously being left with the option to auto-transplant the parathyroid gland upon frozen biopsy confirmation. Similarly, frozen section analysis can be used to confirm a suspect tissue strongly felt to be parathyroid by surgeon, while PTeye did not indicate the same (false negative). During a parathyroidectomy procedures where routine IOPTH assays are performed, if the surgeon were to accidentally remove thyroid/fat/lymph node assuming it was a diseased parathyroid as indicated by PTeye (false positive), parathyroid hormone (PTH) levels obtained 10 minutes after excision will fail to drop below 50% of baseline PTH levels (43,44). Similarly, the PTH levels will not drop if the surgeon was to leave behind a diseased parathyroid assuming it was healthy thyroid/fat/lymph node tissue (false negative). Both these scenarios can prompt the surgeon to further explore until the diseased parathyroid is identified. It must be however be borne in mind that reliance on frozen biopsies and IOPTH assays as an adjunct to the PTeye would only occur in such specific circumstances, as evidenced by the low false positive rate of 3.5% and false negative rate of 4.5% obtained with the PTeye. These risk mitigation strategies can still not circumvent accidental excision of healthy deep seated or intrathyroidal parathyroid glands, as these types of glands are poorly detected even with routine imaging modalities. The utility of these risk mitigation strategies would eventually vary from patient to patient and would be best applied based on the surgeon's discretion.
Another notable finding reported in our study is that r-SHP cases exhibited reduced normalized NIRAF intensities, the reasons for which remain presently unknown. It had been previously reported by McWade et al. that only 54% of the r-SHP cases (7/13) could be detected with the lab-built system (32), while a sensitivity of 94–100% was achieved for all other categories of thyroid and/or parathyroid pathology. In our study, false negative readings commonly occurred in r-SHP patients, resulting in a false negative rate of 11.9% and 4.5% for the lab-built system and the clinical PTeye system respectively. This was further evidenced by the improved performance of the PTeye in the single user comparison study (sensitivity = 100%) as compared with the overall performance (sensitivity = 95.5%), as no r-SHP patients enrolled during the single user comparison study. Excluding data from r-SHP patients lead to improved sensitivity of parathyroid identification of 89.8% and 99% for the lab-built and the PTeye system respectively. It can therefore be assumed that the PTeye system will not be able to identify diseased parathyroid glands seen in r-SHP patients as effectively. Since only one r-SHP case was investigated with PTeye as compared with five for the lab-built system, further studies involving a larger sample size will be required to draw any conclusion on the ability of PTeye to guide the surgeon in parathyroid identification for r-SHP patients.
Potential impact and benefits of the PTeye on surgical management, patient care and health care costs
The true impact of the PTeye in improving patient outcomes is yet to be determined, as the participant surgeons in the current study were blinded. Nonetheless, Benmiloud et al. recently demonstrated that NIRAF-based parathyroid localization could help in minimizing postoperative hypocalcemia in thyroidectomies (45). Since our study clearly demonstrates that PTeye can also identify parathyroid tissue with high accuracy when used as indicated, this device could similarly reduce postsurgical complications and provide optimal patient outcomes. Impact of PTeye on surgical management could also vary due to differences in (i) surgical training and experience, (ii) surgical volume among centers, and (iii) variability in surgical techniques and OR practices worldwide and would therefore need to be evaluated in more diverse clinical settings. While high-volume surgeons are proficient in locating parathyroid glands visually due to their considerable years of surgical experience, they may still find it challenging to identify parathyroid glands during (i) high-risk cases (Graves' disease and total thyroidectomy with central neck dissection), (ii) re-operative surgeries (distorted anatomy/scar from previous surgeries), (iii) surgeries involving ectopic parathyroid glands, (iv) excision of nodular thyroid coexisting with hyperparathyroidism (to differentiate between thyroid nodules and parathyroid glands), and (v) thyroidectomies for Hashimoto's thyroiditis (reactive lymph nodes can be confused with parathyroid glands). These complex circumstances can result in postoperative hypocalcemia or incomplete parathyroidectomies for high-volume surgeons as well (46,47). In such scenarios, the surgeon can utilize the fiber-optic probe of the PTeye to screen the surgical field for potential parathyroid glands and be alerted via auditory feedback in a manner similar to nerve monitoring devices (48), in order to carefully conduct the ongoing dissection. In contrast, it becomes vital to assess the cost-effectiveness of modalities like the PTeye for low-volume surgeons who typically perform <25 thyroid surgeries or <15 parathyroid surgeries per year (47,49 –51). Assuming a minimal rate of 20 thyroid and 10 parathyroid surgeries per year, with an associated cost of at least one frozen section analysis (cost ∼145 USD/specimen) and additional 20 minutes of anesthesia administered during the procedure (cost ∼210 USD) (52), health care costs that could be minimized per year would amount to 10,650 USD even for a low-volume center. Higher costs would need to be factored for additional frozen sectional analysis per surgeries and health care expenses for postoperative complications (hypocalcemia following thyroid surgeries or completion surgeries after failed parathyroidectomies) that tend to be even higher with low-volume surgeons (51,53). Thus, a reusable device like PTeye with a one-time purchase expense can reduce or offset these recurrent health care costs for low-volume surgeons. It should also be noted that low-volume, lesser experienced surgeons can be employed at high-volume centers during early stages of their career, where they are on a learning curve at becoming adept in thyroid/parathyroid surgeries. In addition, PTeye can be a beneficial tool utilized for teaching resident or fellow surgeon trainees. As they transition into experienced/high-volume surgeons at high-volume centers, devices such as the PTeye can be cost effective as well by reducing unnecessary frozen section analyses, decreasing surgery duration, and minimizing postoperative complications.
The role and need of a real-time guidance tool such as PTeye for parathyroid identification may also vary depending on the type of surgery and the condition of in situ parathyroid glands (disease state, vascularity) during the operative procedure. While PTeye can identify both normal and diseased glands (except r-SHP cases) with high accuracy during parathyroidectomies, this device is not designed to differentiate between normal and diseased parathyroid glands and should be used complementarily with standard IOPTH assays as described earlier. Nonetheless, PTeye could assist the surgeon to rapidly identify parathyroid glands regardless of disease state and thus reduce surgical exploration time during parathyroidectomies. For thyroidectomies in benign disease, a suspected parathyroid that appears well perfused and viable may often be left behind in situ regardless of whether it was correctly identified or not. Considerable surgical time would however be expended for pericapsular dissection and preserving blood vasculature of a presumed healthy parathyroid that may be a fat lobule/lymph node/thyroid nodule. The PTeye can minimize these instances by aiding the surgeon in differentiating parathyroid glands from these tissues noninvasively in real time. In circumstances when the suspect parathyroid appears ischemic, it may need to be excised regardless and would need to be confirmed as parathyroid tissue via frozen section analysis prior to auto-transplantation. Yet, some surgeons tend to postpone excision of an ischemic-appearing parathyroid gland until the end of the surgical procedure to assess whether the parathyroid has regained its vascularity as the parathyroid gland discoloration may only be transient (54). In such situations, key decision-making occurs towards the end of the procedure and would be contingent on (i) whether an autotransplantation is required and (ii) whether the visualized candidate is parathyroid tissue or not. Parathyroid autotransplantation would then need to be deferred by about 20 minutes till the frozen section analysis report arrives, which could be circumvented with PTeye being able to perform real-time parathyroid identification. The device can also be beneficial for noninvasively differentiating between a lymph node that requires excision and a healthy viable parathyroid gland that should be preserved during total thyroidectomies for malignant thyroid diseases that require central or lateral neck lymph node dissection. On the other hand, biopsy of a suspect ischemic parathyroid gland should be obtained for frozen section analysis regardless of the output displayed by PTeye, to mitigate the risk of autotransplanting a metastatic lymph node as described previously.
While it may not be able to totally eliminate intraoperative frozen section analysis for parathyroid gland confirmation, the PTeye with an overall accuracy of 96.1% does demonstrate the potential to minimize unnecessary frozen section analyses. Therefore, implementing the use of the PTeye during routine thyroidectomy and/or parathyroidectomy procedures could guide surgeons in rapid and accurate intraoperative parathyroid identification, cutting down on lengthy wait-times and additional costs associated with unnecessary frozen biopsies, while alleviating the workload for surgical pathology. In turn, the PTeye can aid in preserving healthy parathyroid glands while ensuring removal of diseased ones, thereby curtailing postoperative morbidity, related hospitalization expenses and resultant malpractice litigations that could occur following head and neck surgeries (4,55).
Footnotes
Acknowledgments
The authors acknowledge the financial support of National Science Foundation Graduate Research Fellowship Program under grant No. 0909667 (to M.A.M) and Grant No. 1R01CA212147-01A1, R42CA192243 from National Institute of Health (to A.M-J.). The authors are also thankful to Christine O’ Brien, Isaac J. Pence, and John Nguyen for their guidance in study design, instrumentation of the lab-built system and ex vivo testing of both the devices. The authors are grateful to Naoko Brown and Dr. Jeff Reese for providing access to murine blood samples utilized for this study.
Author Disclosure Statement
Professor Anita Mahadevan-Jansen and Vanderbilt University have a licensing agreement with AiBiomed Instruments (Santa Barbara, CA) for developing the clinical prototype system, PTeye, that has been investigated in this study. AiBiomed Instruments is the exclusive licensee of the intellectual property on the described NIRAF detection method from Vanderbilt University.