
Abstract
SECISBP2 is an essential factor in selenoprotein synthesis, and its mutations result in a multiorgan syndrome, including abnormal thyroid hormone metabolism. A 10-year-old obese Turkish boy born to consanguineous parents presented with high thyroxine, low triiodothyronine, high reverse triiodothyronine, and normal or slightly elevated thyrotropin. He also had attention-deficit disorder and muscle weakness but no delay in growth or bone age. Sequencing of genomic DNA revealed a novel c.800_801insA, p.K267Kfs*2 mutation, homozygous in the proband and heterozygous in both parents and his brother. Studies showed reduction in several selenoproteins in serum and fibroblasts.
Introduction
H
Case History
The proband was born to first cousins of Turkish origin. Pregnancy, delivery at 37 weeks, birth weight, and early development were normal. He was 10 years old when one of the authors (G.C.) was consulted to evaluate the patient for obesity. He had leg weakness, fatigued easily, and had attention-deficit disorder with poor school performance. At 11 years and 5 months, his weight was 67.7 kg (SDS +2.02), his height was 148.2 cm (SDS −0.45), his body mass index (BMI) was 29.5 kg/m2 (SDS +2.19), and his bone age was 11 years. Tanner stage was III, with a testes volume of 10 mL. His mother's and father's BMIs were 29.6 and 28.4 kg/m2, respectively. Right-eye ptosis was present since infancy. He had no goiter (volume 1.7 mL on ultrasound; SDS −1.92). Neurological examination revealed Gowers' sign, indicating weakness of the proximal lower-limb muscles. Muscle biopsy was normal, though electromyography revealed myogenic involvement of the proximal upper and lower extremities, and magnetic resonance imaging (MRI) showed fatty infiltration of the muscles. His IQ score was 91. His audiogram and echocardiogram were normal.
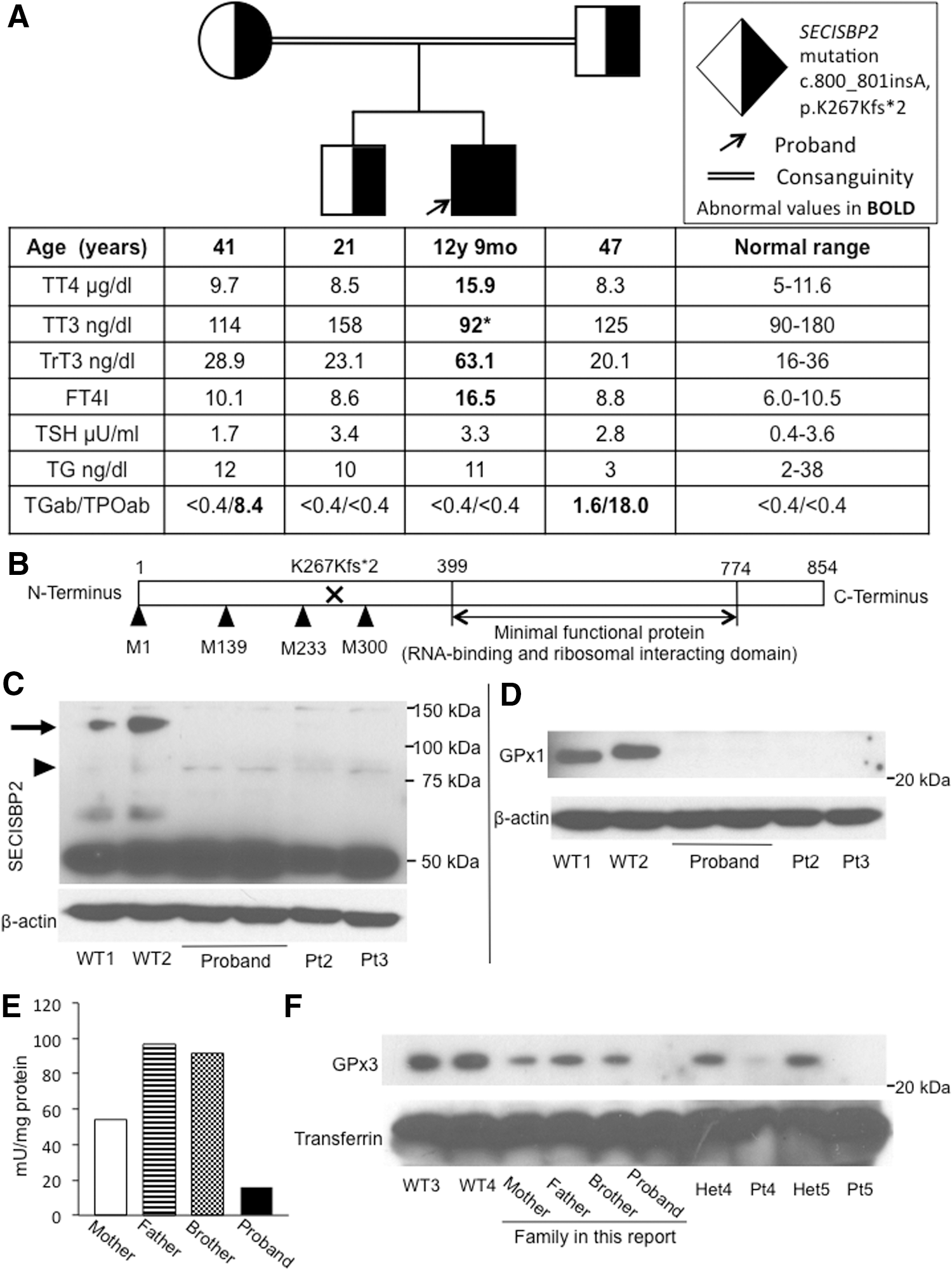
TFTs revealed elevated free thyroxine (T4), low free triiodothyronine (T3), elevated reverse T3, and normal or slightly elevated thyrotropin levels (Fig. 1A). His HbA1c was 5.6%, but his plasma glucose on oral glucose tolerance test (OGTT) was 80, 220, and 150 mg/dL at 0, 60, and 120 minutes, respectively. Neither of his parents had diabetes mellitus, and an OGTT was not performed in them. Serum selenium (Se) was low at 23 μg/dL (reference range 63–160 μg/dL).
(
Results
Informed consent was obtained for investigations approved by the Institutional Review Board. The entire coding region of the SECISBP2 gene was sequenced using genomic DNA. A c.800_801insA p.K267Kfs*2 mutation was found; the proband was homozygous, both parents and the brother were heterozygous for the mutation (Fig. 1A). Graphic representation of the SECISBP2 protein shows the location of the mutation relative to the functional domains and the alternative methionine translation initiation sites (Fig. 1B).
Supplementation of 200 μg/day sodium selenite for five months followed by 400 μg/day for three further months increased the serum Se from 23 to 74.5 μg/dL. However, serum T4 remained high and T3 low.
At the age of 12 years and 8 months, his Tanner stage was III, with testes volumes of 12 and 15 mL, and his bone age was 13 years. However, his growth velocity decreased to 3.8 cm/year (−1.46 SDS), and his height curve decreased from the 50th to the 25th percentile (Supplementary Fig. S1; Supplementary Data are available online at
Western blotting of the proband's cultured skin fibroblasts showed lack of full-length SECISBP2 protein (Fig. 1C). Assessment of selenoproteins showed greatly diminished GPX1 protein levels in fibroblasts, similar to other reports in SECISBP2-deficient patients (Fig. 1D) (1,2). The enzymatic activity of GPX in the serum was also markedly decreased (Fig. 1E), with the proband's GPX activity being the lowest compared to the other family members. This was also confirmed at the protein level, with serum GPX3 protein levels being markedly decreased in the proband and diminished in the heterozygous parents and brother (Fig. 1F). This was also the case with biallelic and monoallelic SECISBP2 mutations in two other families (Fig. 1F). These data indicate that the defective expression of full-length SECISBP2 caused a global decrease in selenoprotein synthesis in the proband as in other subjects with SECISBP2 deficiency.
Discussion
This novel homozygous early termination mutation leads to absence of the full-length SECISBP2 protein. However, a shorter isoform starting from methionine 300 containing the C-terminal functional domain is expected to be translated (3) and to provide some residual SECISBP2 function. Different from other SECISBP2 deficient patients, this child had normal height and bone age. However, decreased growth velocity developed at 13 years of age, and provocative testing showed GH deficiency, not previously reported in SECISBP2-deficient patients.
Single patients with increased fat mass and insulin sensitivity as well as recurrent fasting hypoglycemia with low insulin levels have been reported (2). This is attributed in part to decreased GPX1 expression because Gpx1-null mice showed increased insulin sensitivity. In contrast, this patient had impaired glucose tolerance in spite of decreased GPX1. His genetic and environmental background may have affected insulin sensitivity independently of SECISBP2 deficiency.
As in a previous report (4), supplementation of sodium selenite for even longer duration did not alter significantly the serum T4 and T3 abnormalities, despite normalization of the selenium level.
Footnotes
Acknowledgments
This work was supported by NIH grant DK110322 (A.M.D.). We thank Miles Tracy for performing the TFTs and Dr. Samuel Refetoff for revision of the manuscript.
Author Disclosure Statement
No competing financial interests exist.