
Abstract
Background:
Low-risk patients with differentiated thyroid cancer can be treated with thyroid lobectomy. Serial measurements of serum thyroglobulin (Tg) are recommended for surveillance, but the cutoff values indicating recurrence are not known. This study documented the natural course of serum Tg levels during follow-up after lobectomy for low-risk papillary thyroid carcinoma (PTC) and evaluated whether changes in serum Tg levels predict disease recurrence.
Methods:
This historical cohort study included 208 patients with low-risk PTC who underwent lobectomy but did not require hormone replacement. Postoperative serum Tg levels and Tg/thyrotropin (TSH) ratios and neck ultrasound were evaluated during a follow-up period with a median of 6.9 years.
Results:
The serum Tg levels increased gradually, and the proportion of patients with levels >10 ng/dL increased annually by 13.9%, 18.8%, 22.1%, 21.9%, 28.4%, and 28.9% during the six-year follow-up period (β = 0.574, p = 0.027). The relative serum Tg levels increased by 10% annually (β = 0.105, p < 0.001), and the levels of Tg and Tg/TSH ratios in 19 patients with recurrent disease did not differ significantly (β = 0.150, p = 0.090). Patients without recurrent disease were more likely to have serum Tg levels increased by >20% (p = 0.022). There were no significant differences in the proportions of patients with serum Tg levels increased by ≥50% or ≥100% in terms of the disease recurrence.
Conclusions:
Serum Tg levels and the Tg/TSH ratio increased gradually after lobectomy in patients with and without recurrences, without any significant differences. Periodic measurements of serum Tg levels seem to have limited value in predicting recurrent PTCs after lobectomy.
Introduction
T
Measurements of serum thyroglobulin (Tg) levels and neck ultrasonography (US) examinations on a regular basis play a key role in the surveillance of DTC patients after surgery (4). The serum Tg level is a specific marker of residual or recurrent disease for patients who undergo total thyroidectomy and subsequent RAI remnant ablation because any detectable Tg levels have a highly diagnostic value under those circumstances (4,9). However, the serum Tg levels play a less important role as a biochemical marker for tumors when there are remnants of normal thyroid tissue after surgery (4). Previous studies have suggested that follow-up neck US examinations with serum Tg measurements can predict the recurrence of DTC in patients with remnant thyroid tissue and without RAI remnant ablation therapy in those who underwent lobectomy (3,10). However, no studies have elucidated serial changes in serum Tg levels and determined serum Tg cutoff values for predicting DTC recurrence in lobectomy patients.
The aim of this study was to evaluate the changes of serum Tg levels during follow-up (median 6.9 years) of patients who underwent lobectomy for low-risk PTC and who did not need thyroxine (T4) replacement therapy. The study also evaluated whether changes in serum Tg levels can predict PTC recurrences after lobectomy.
Methods
Patients
This historical cohort study initially included 637 patients with low-risk PTC who underwent lobectomy between 2008 and 2009 at the Asan Medical Center in Seoul, Korea. Low-risk DTC was defined according to the following criteria: intrathyroidal DTC, with a tumor <4 cm in size, with no extrathyroidal extension, no vascular invasion, and no clinical lymph node (LN) metastases or five or fewer pathological N1 micrometastases (<0.2 cm in largest dimension). Initially, patients whose serum TSH levels remained in the reference range (0.4–4.5 mIU/L) without thyroid hormone replacement therapy were included, and patients who received thyroid hormone replacement therapy after lobectomy (n = 71) or whose serum TSH levels were out of the reference range during follow-up (n = 112) were excluded. However, patients with follow-up durations shorter than five years (n = 66), those lacking follow-up data (n = 8), and those with positivity for anti-Tg antibodies (n = 172) were also then excluded. Finally, data from 208 patients were analyzed for this study. Only 4/208 patients experienced a recurrence. To evaluate the serial changes of serum Tg levels in patients with recurrent PTC after lobectomy, an additional 15 patients with recurrent disease after initial lobectomy between 2008 and 2012 were included. All these patients had initially undergone lobectomy due to low-risk PTC. The Institutional Review Board of the Asan Medical Center approved this study.
Laboratory measurements and follow-up
The patients were followed up starting within the first three to six months after lobectomy, with exams every 6–12 months thereafter. Serum TSH, free T4 (fT4), Tg, and anti-Tg antibody (TgAb) levels were measured, as described in the literature (11,12). The reference ranges for TSH and fT4 were 0.4–4.5 mIU/L and 0.80–1.90 ng/dL, respectively. The serum Tg levels were determined using an immunoradiometric assay (Tg-plus RIA kit; BRAHMS AG, Henningsdorf, Germany). The functional sensitivity of the assay is 0.2 μg/L, with a coefficient of variation of 20% and an analytical sensitivity of 0.08 μg/L. The serum TgAb levels were determined by radioligand assays (anti-Tg RIA kit; BRAHMS AG), with a functional sensitivity of 20 IU/mL. A positive TgAb thought to interfere with the Tg measurement was defined as serum TgAb ≥60 IU/mL (13). Details of these assays have been previously described (13). Neck US examinations were performed every six months during the first year after lobectomy and were repeated every 12–24 months thereafter.
Definitions
The changes in serum non-stimulated Tg levels were determined for each patient during each follow-up exam. The relative changes in serum Tg were defined as the level during follow-up divided by the first value obtained postoperatively. The maximum increase in serum Tg levels was defined as an increase of ≥20%, ≥50%, or ≥100% in two consecutive measurements. A 20% cutoff value was adopted, which was reported to be clinically significant in a previous study (14). The values of ≥50% and ≥100% maximal increase were arbitrarily chosen. The presence of recurrent/persistent disease was defined by cytologically or histologically proven lesions in suspicious LNs, in the thyroid bed, or in the contralateral lobe on neck US images, as previously described (15). The initial tumor-node-metastasis (TNM) staging was determined based on the guidelines of the seventh edition of the American Joint Committee on Cancer/Union for International Cancer Control staging system (16).
Statistical analysis
The data were analyzed using R software v3.0 (R Foundation for Statistical Computing). Continuous variables are described as means and standard deviation or medians with interquartile ranges (IQR). Categorical data are described as numbers and percentages, with comparisons performed with the chi-square test. The significance of change in serum Tg levels was evaluated using the mixed linear model. All p-values were two-sided, and p-values of <0.05 were considered statistically significant.
Results
Baseline characteristics of patients
The baseline clinical and pathological characteristics of the 208 patients with low-risk PTC who underwent lobectomy and did not require thyroid hormone replacement are described in Table 1. Their mean age was 47.04 ± 10.14 years, and 76.9% of them were women. The mean primary tumor size was 0.76 ± 0.46 cm, and microscopic extrathyroidal extension was present in 24 (11.5%) patients. Central cervical LN metastases were found in 55/208 (26.4%) patients, but no lateral cervical LN metastases were found. According to the TNM staging, 34.6% of patients had stage III disease, and the remainder had either stage I or stage II disease. There were no cancer-related deaths, and only four (1.9%) patients had recurrent/persistent disease during follow-up.
Categorical variables are described by numbers and percentages, and continuous variables by means and standard deviations. The TNM stage was determined according to the seventh American Joint Cancer Committee TNM stage system.
Microscopic extrathyroidal extension.
LN, lymph node; TNM, tumor-node-metastasis.
Serum Tg levels changes after lobectomy
The median follow-up duration after lobectomy was 6.9 years (IQR 5.93–6.99 years). Serum Tg levels were classified into five groups: <1 ng/dL, 1–5 ng/dL, 5–10 ng/dL, 10–30 ng/dL, and >30 ng/dL. The distribution of serum Tg levels during the follow-up periods are presented in Figure 1A. At the first year after lobectomy, serum Tg levels were between 1 and 5 ng/dL in 89/208 (42.8%) patients and between 5 and 10 ng/mL in 69 (33.2%) patients. In addition, the serum Tg levels were >30 ng/mL in only two (1.0%) patients. The proportion of patients with serum Tg levels <5 ng/dL decreased annually thereafter by 52.9%, 42.8%, 42.3%, 39.8%, 43.3%, and 40.2% between one and six years after surgery. At the same time, the proportion of patients with serum Tg levels >10 ng/dL increased annually by 13.9%, 18.8%, 22.1%, 21.9%, 28.4%, and 28.9% during the same follow-up period (β = 0.574; p = 0.027).
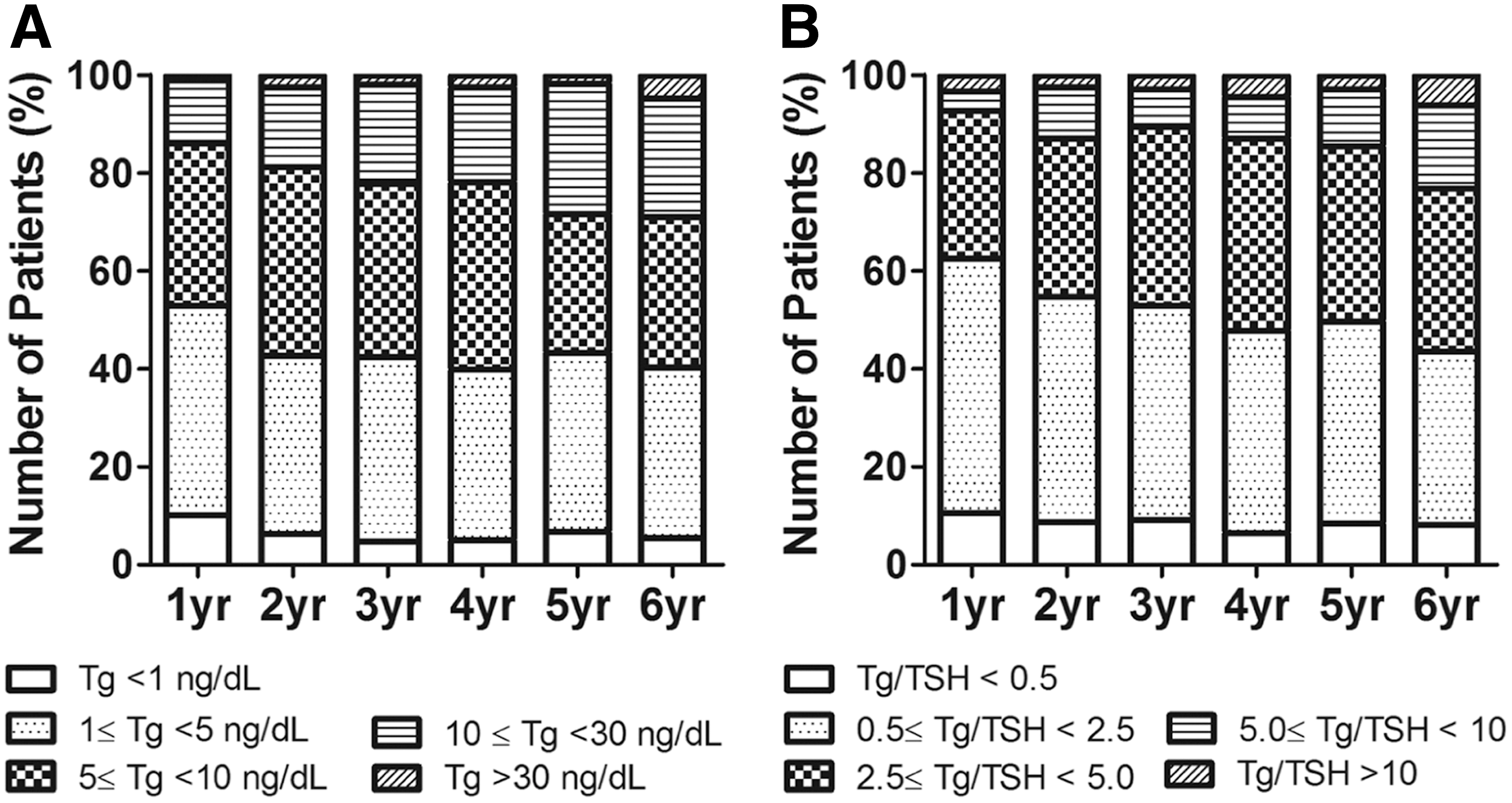
Annual changes in postoperative serum thyroglobulin (Tg) levels in papillary thyroid carcinoma (PTC) patients who underwent lobectomy. (
The changes in the ratio of serum Tg divided by serum TSH levels (Tg/TSH ratio) were also evaluated to account for the impact of serum TSH on the serum Tg levels (Fig. 1B). Tg/TSH ratios were classified into five groups: <0.5, 0.5–2.5, 2.5–5, 5–10, and >10. It was found that the trends of serum Tg/TSH ratios were similar to those of the serum Tg levels in the study patients. The proportion of patients with Tg/TSH ratios <2.5 decreased annually by 62.5%, 54.8%, 52.9 47.8%, 49.7%, and 43.5% between one and six years after lobectomy, while the proportion of patients whose Tg/TSH ratios >5 increased annually by 7.2%, 13.0%, 10.6%, 12.9%, 14.5%, and 23.1% during the same periods (β = 0.277; p = 0.265).
The serial trends of relative serum Tg levels were also evaluated annually during the follow-up period (Fig. 2). A significant increasing trend was found of relative serum Tg levels after lobectomy. The serum Tg levels increased about 10% annually (β = 0.105; p < 0.001).
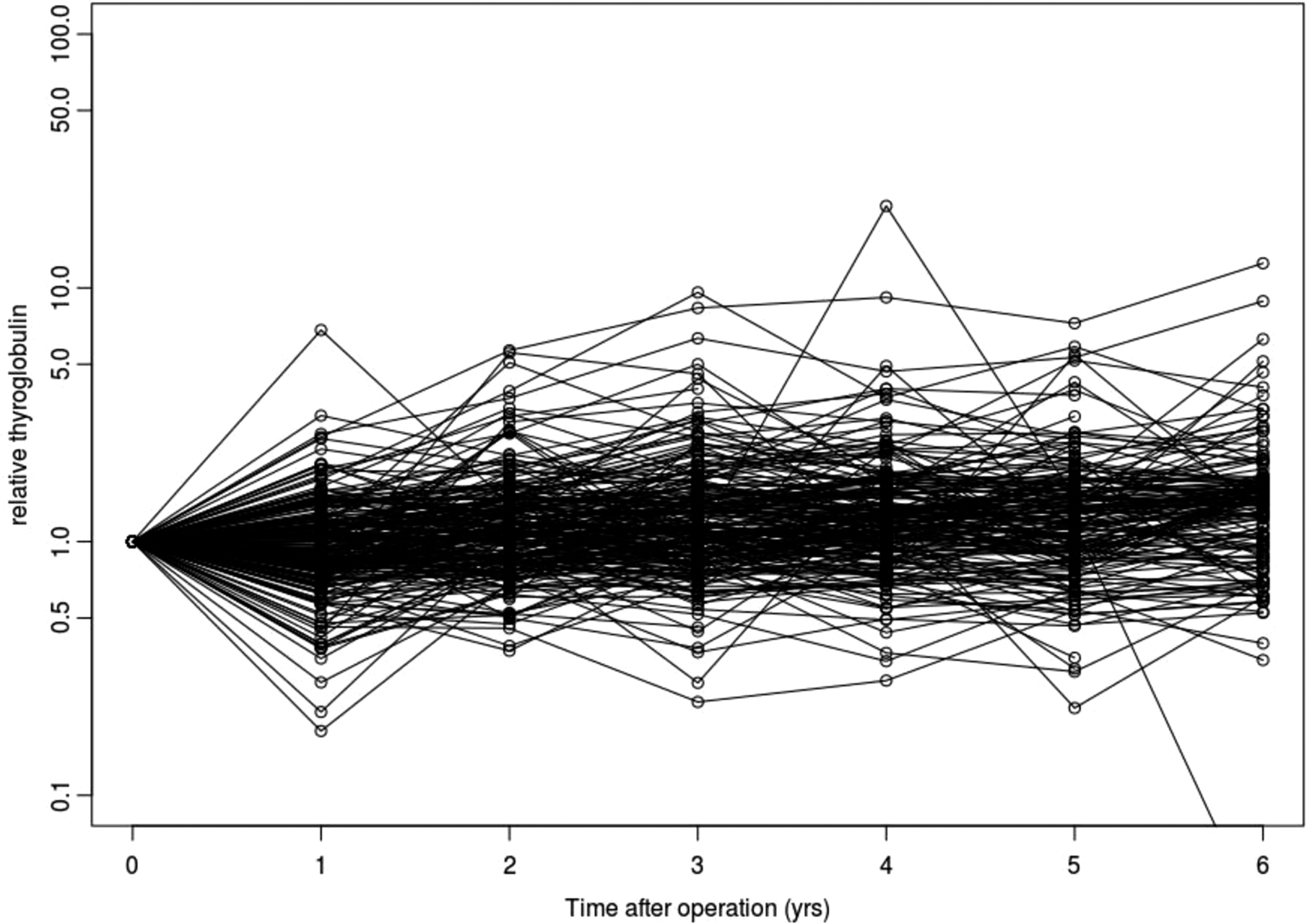
Trend of postoperative relative serum Tg values in PTC patients who underwent lobectomy.
Postoperative serum Tg level changes in patients with recurrent PTC after lobectomy
The serial changes of serum Tg levels were evaluated in 19 patients with recurrent PTC after lobectomy during extended study periods. Thirteen (68.4%) patients had recurrent disease in the contralateral lobe, and six (31.6%) patients had recurrent PTC in the central or lateral cervical LNs. The serum Tg levels during follow-up are described in Table 2. The trends of serum Tg levels increased, but not significantly (β = 0.150; p = 0.090). The changes in serum Tg levels prior to the detection of recurrence are presented in Figure 3. Of 13 patients with contralateral lobe recurrences, the levels increased more than twofold in three (23.1%) patients. However, the remaining 10 (76.9%) patients presented stable or decreasing levels (Fig. 3A). The changes in relative Tg/TSH ratios in these patients were similar to those with relative Tg changes (Fig. 3B).

Trends of relative postoperative serum Tg values and Tg/TSH ratios in patients who had recurrent PTC after lobectomy. (
PTC, papillary thyroid carcinoma; Tg, thyroglobulin.
The study also evaluated the changes in serum Tg levels in six patients who had recurrent disease in cervical LNs. The relative serum Tg levels increased in only one of six (16.7%) patients, whereas the remaining five (83.3%) patients had stable or decreasing serum Tg levels (Fig. 3C). The values of relative Tg/TSH ratios tended to increase in three patients (50%; Fig. 3D).
Maximal increases in serum Tg levels in patients with or without recurrence
Maximal increases in serum Tg levels were compared between patients with and without recurrent PTC after lobectomy. The maximal increases in serum Tg levels were classified as ≥20%, ≥50%, and ≥100% in two consecutive measurements. The serum Tg levels were increased by >20% in 92.2% of patients without recurrence and in 73.7% of patients with recurrence (p = 0.022; Table 3). Patients without recurrent disease were more likely to have serum Tg levels increased by >20%. No significant differences were found in the proportion of patients with serum Tg levels increased by >50% or 100% between the two groups (Table 3).
Discussion
Periodic neck US and serial serum Tg measurements are important in follow-up for patients with DTC who undergo less than total thyroidectomy without RAI remnant ablation. However, the clinical implications of the serum Tg levels are controversial, especially in lobectomy patients. This study tried to characterize the serial serum Tg level changes in low-risk PTC patients who underwent lobectomy. Patients whose serum TSH levels remained within the reference range without the need for thyroid hormone replacement were included. The approach was mainly intended to characterize the natural course of serum Tg levels after lobectomy. The serum Tg levels were found to be slightly increased after lobectomy, and the proportion of patients with levels >10 ng/dL increased significantly over time. About 61.3% of patients with no evidence of disease had serum Tg levels that increased by >50% during follow-up. The study also evaluated the serum Tg level changes in patients who had recurrent disease, and no significant differences were found when compared to the changes seen in patients without recurrence.
Patients with low-risk DTC usually have excellent prognoses (17 –19). Several studies have reported structural disease recurrence to be <1–2% in low-risk DTC (18,20), with a 20-year disease-specific survival rate of 99% (21,22). Therefore, conservative approaches are preferred for the management of patients with low-risk DTC, and active surveillance may be carried out, considering cost-effectiveness and quality of life (3,14). However, recurrent disease does occur in a few patients after lobectomy, and recurrences have been confirmed even after 10 years (23). Therefore, it is difficult to decide how long the follow-up period needs to be and what surveillance intensity is appropriate for patients with low-risk DTC (24). Revised guidelines suggested periodic serum Tg measurements and neck US examination during follow-up of patients with DTC who underwent less than total thyroidectomy without RAI remnant ablation (4). However, it is difficult to decide how frequent follow-up exams should be performed, and a specific cut-off for an increase in serum Tg is not known. Additionally, serum Tg levels are difficult to interpret in patients with remnant normal thyroid tissue after thyroid surgery because detectable levels can originate from both normal and neoplastic thyroid tissues (12). Moreover, the level of serum Tg values depend on the amount of remaining thyroid tissue, especially after lobectomy (3), and studies focusing on serial changes of serum Tg levels are still needed in patients who undergo lobectomy for low-risk DTC.
A recent study of 290 DTC patients who underwent total or near total thyroidectomy without RAI remnant ablation reported that the postoperative Tg levels in most patients (98.7%) decreased spontaneously or remained stable during a median of five years of follow-up (20). This suggested that serum Tg measurements might be useful for patients who underwent total or near-total thyroidectomy, even without RAI remnant ablation. However, this study was found that the serum Tg levels in the lobectomy patients increased gradually without definite evidence of disease recurrence during follow-up, and this suggests a compensatory increase of the remnant thyroid tissue after lobectomy that may contribute to the increases seen in the serum Tg levels. The serum Tg levels vary according to degree of TSH stimulation (25). Previously, disease recurrence and dynamic risk stratification (DRS) were evaluated according to the levels of serum TSH in low-risk DTC patients after lobectomy (26). In that study, 74% of patients treated with TSH suppression therapy and 11% of patients without TSH suppression therapy had serum TSH levels <2 mIU/L (26). Patients without TSH suppression therapy showed a higher frequency of biochemical incomplete response in DRS, but there was no significant difference in disease-free survival compared to patients with a suppressed TSH (26). Thus, a potential effect of TSH suppression cannot be ruled out in previous studies. In this study, 208 patients with serum TSH levels within the reference range and without thyroid hormone replacement after lobectomy were included. Therefore, the results represent the serum Tg changes without TSH effects. The number of metastatic LNs and their total surface or total volume has been reported to be significantly associated with the serum Tg/TSH ratio in patients with DTC (27). Therefore, the Tg/TSH ratio changes were also evaluated to adjust for the influence of serum TSH, even when the level was within the reference range.
In a previous study, serum Tg measurements were found to be useful for detecting structural recurrent disease in 70 low- to intermediate-risk DTC patients who underwent lobectomy (14). In that study, only five patients had recurrent disease, and four of them had increased serum Tg levels. The authors proposed that any increase or decrease in serum Tg levels by >20% in two consecutive measurements was clinically significant, and they suggested that stable or decreased serum Tg levels are associated with a lower probability of recurrence (14). However, that study was relatively small to conclude that there is an association between the serum Tg level changes and clinical outcomes. It appears that the serum Tg levels during follow-up are less specific for recurrence in lobectomy patients compared to their specificity in patients who underwent total thyroidectomy and RAI remnant ablation. In this study, serum Tg levels without TSH suppression were evaluated in lobectomy patients, and the significant changes in serum Tg were defined as those >20%, 50%, or 100%. However, no significant differences were found in serum Tg levels between patients with recurrent disease and those without evidence of recurrence. It was also found that decreased or stable serum Tg levels did not guarantee a lower probability of recurrence.
Periodic neck US examination has excellent sensitivity and specificity for detection of suspicious cervical LN metastases (28). Several studies have shown that neck US is more likely to detect disease recurrence compared with stimulated serum Tg measurements or diagnostic 131I whole-body scintigraphy (28,29). In this study on lobectomy patients, most of the recurrences were initially detected by neck US examination. Therefore, serum Tg measurements should be regarded as complementary to neck US to identify recurrent disease, and neck US should be the primary modality for the surveillance of low-risk DTC patients who undergo lobectomy.
This study has some limitations due to its retrospective design. The number of patients with recurrent disease during follow-up is relatively small because only patients with low-risk PTC were included. However, this approach was inevitable because patients who did not require LT4 replacement were enrolled. In addition, the follow-up period of the study may not have been sufficient to evaluate patients with late recurrences, which can be found up to 10 years after the initial treatment (20). Nevertheless, this study characterizes the natural trends of serum Tg levels after lobectomy in a cohort with a unified protocol of initial treatment and follow-up strategy. The findings provide important insights into the natural course of serum Tg production by remnant thyroid tissue after lobectomy.
In conclusion, this study found that serum Tg levels increased gradually during follow-up in lobectomy patients. There were no significant differences in serum Tg level changes between patients with or without recurrent disease. Periodic measurements of serum Tg levels were not useful for predicting recurrent disease in these patients. The monitoring of patients by postoperative neck US examination plays an important role in the long-term surveillance of low-risk DTC patients after lobectomy.
Footnotes
Acknowledgments
This study was supported by the National Research Foundation (NRF) of Korea Research Grant (NRF-2015R1C1A1A02036597) and a grant from the Korean Health Technology R&D project, Ministry of Health & Welfare, Republic of Korea (HC15C3372).
Author Disclosure Statement
No authors have any conflicts of interest in relation to this manuscript.