
Abstract
Background:
Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy in children and adolescents. Infrequently, children with PTC may present with or develop disease not amenable to surgery or radioactive iodine (RAI), and systemic therapy may be an option. Lenvatinib is an oral tyrosine kinase inhibitor that is approved by the Food and Drug Administration for the treatment of adults with locally recurrent or metastatic, progressive, RAI-refractory well-differentiated thyroid carcinoma. The effect of lenvatinib in children with PTC has not been reported.
Patient findings:
Three children with metastatic PTC not amenable or refractory to RAI who responded to lenvatinib are reported. All of them developed respiratory distress requiring oxygen caused by extensive bilateral metastatic pulmonary disease. The first patient is a 14-year-old female who was initially treated with sorafenib for extensive PTC not amenable to upfront surgery or RAI. She had progressive pulmonary disease after five months, and was subsequently treated with oral lenvatinib (14 mg/m2/day). She was weaned to room air after eight weeks. The second patient is a 15-year-old male who was treated with lenvatinib (14 mg/m2/day) for iodine non-avid diffuse pulmonary disease after initial total thyroidectomy and cervical lymph node dissection. He was weaned off oxygen in six weeks. The third patient is a five-year-old male who was treated with lenvatinib (14 mg/m2/day) for pulmonary disease progression 24 months after treatment with total thyroidectomy, cervical lymph node dissection, and RAI treatment. He was weaned off oxygen one day after starting lenvatinib. Two of the patients required dose adjustments secondary to proteinuria. Otherwise, all patients tolerated lenvatinib well. The first two patients remained clinically stable on lenvatinib 23 months and 11 months after initiation of therapy, respectively, and the third patient transitioned to a tumor-specific targeted therapy after one month.
Summary:
Three pediatric patients are reported with metastatic PTC not amenable or refractory to RAI who achieved a response on lenvatinib.
Conclusion:
Lenvatinib therapy is well tolerated and demonstrated clinical activity in children with advanced PTC. Lenvatinib should be considered in children with PTC that is refractory or not amenable to conventional management.
Introduction
D
Among other genetic changes, somatic RET/PTC rearrangements, point mutations in BRAF, and NTRK fusion oncogenes have been identified in PTC (9 –13). The RET proto-oncogene encodes a receptor tyrosine kinase, and alterations in the gene can result in activation of the mitogen-activated protein kinase (MAPK) signaling cascade. Alterations of other tyrosine kinase receptors, such as vascular endothelial growth factor receptors (VEGFR) and fibroblast growth factor receptors (FGFR), are also implicated in thyroid cancers and similarly activate the MAPK pathway. The use of targeted therapies including tyrosine kinase inhibitors has been well documented in adults with progressive and radioactive iodine (RAI)-refractory DTC (14,15). Response to sorafenib, a small molecule multi-kinase inhibitor, has been described in pediatric patients with progressive RAI refractory PTC or disease not amenable to upfront RAI (16,17).
Lenvatinib is an oral receptor tyrosine kinase inhibitor with multiple targets that inhibits VEGFR-1-3, FGFR-1-4, platelet-derived growth factors, c-KIT, and RET, resulting in antitumor and antiangiogenic activity (18). Lenvatinib has been approved by the Food and Drug Administration (FDA) for the treatment of adults with locally recurrent or metastatic, progressive, RAI-refractory DTC. The use of lenvatinib is currently being studied in children, and the effect of lenvatinib in children with refractory or progressive thyroid carcinoma has not been reported in the literature. Here, three pediatric patients with metastatic PTC who responded to lenvatinib are presented.
Patient 1
A 14-year-old female with a previous history of asthma presented with respiratory distress and neck swelling. One month prior, she had been treated for a diagnosis of miliary tuberculosis. On presentation, she required 10 L of supplemental oxygen. On examination, she had a large palpable fixed mass in the anterior neck and extensive bilateral lymphadenopathy. A computed tomography (CT) scan of the chest revealed numerous bilateral pulmonary nodules, and an ultrasound scan showed multiple heterogeneous solid masses with microcalcifications replacing the entire thyroid. A neck CT showed a large, irregularly shaped, heterogeneous, rim-enhancing lesion arising from the lower pole of the right thyroid lobe compressing and distorting the anterior border of the trachea, in addition to massive bilateral cervical lymphadenopathy. PTC was diagnosed based on fine-needle aspiration cytology of a thyroid nodule. The tumor-node-metastasis (TNM) staging at diagnosis was T4aN1bM1.
Due to extensive neck disease and respiratory distress with an oxygen requirement, surgical resection was considered high risk for complications. RAI treatment was not feasible due to the extensive pulmonary disease and the risk for pulmonary fibrosis. She was started on oral sorafenib at a dose of 200 mg/m2 twice a day. Her respiratory status quickly improved, and she was weaned off oxygen in one week. After two months of treatment with sorafenib, her thyroglobulin (Tg) decreased from 6594 to 1472 ng/mL. Radiographically, the thyroid mass appeared stable, with a more well defined homogenous central hypodensity, and the lymph nodes and pulmonary nodules appeared stable to slightly smaller, with no evidence of new or progressive disease.
Despite the initial favorable clinical and radiographic response, she presented with respiratory distress and oxygen requirement five months after starting sorafenib. A chest CT showed an increase in the number and size of innumerable, bilateral diffuse pulmonary nodules (Fig. 1A). Her Tg level was 1681 ng/mL. She was subsequently enrolled in a Phase I study with oral lenvatinib at a dose of 20 mg daily (14 mg/m2/day) repeated in four-week cycles. She no longer required continuous oxygen 10 days after starting lenvatinib, and after two cycles, she no longer required supplemental oxygen. Imaging studies performed after four cycles revealed a partial response (Fig. 1B). Her Tg level was 433 ng/mL. Total thyroidectomy and cervical lymph node dissection was attempted after five cycles. However, only partial debulking was possible due to the adherent and infiltrative nature of the tumor. She had progression of pulmonary disease while lenvatinib was held in the perioperative period. She was subsequently taken off protocol and continued on lenvatinib off study.
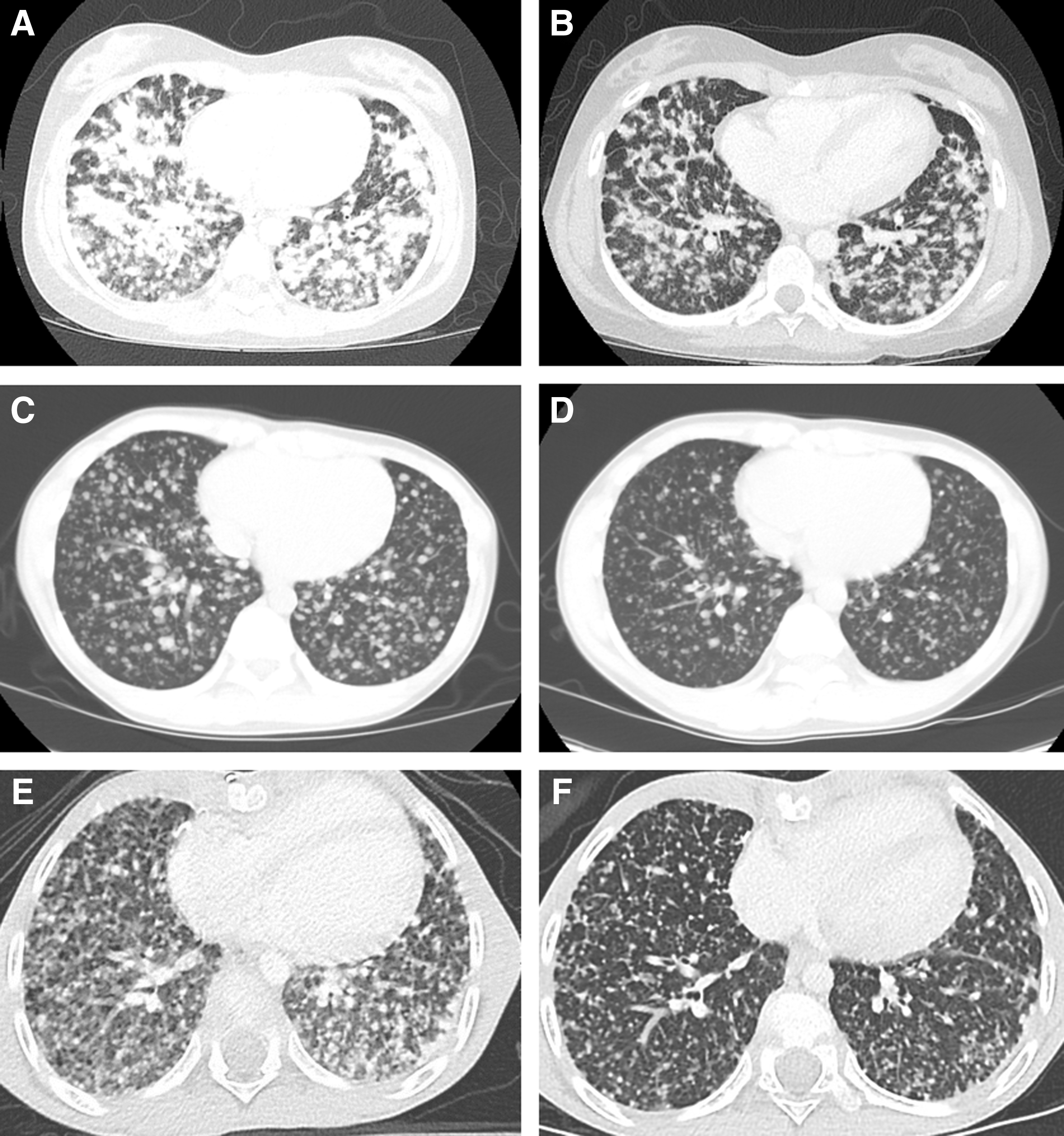
Representative computed tomography images at baseline (left) and after lenvatinib therapy (right) showing decrease in pulmonary disease burden. (
She had multiple episodes of grade 3 proteinuria that required dose interruptions and adjustments to lenvatinib. She has had no other significant side effects. A multi-biomarker next-generation sequencing assay performed on the tumor tissue detected the fusion transcript TRIM24(9)-RET(12). Twenty-three months after starting lenvatinib, she was receiving 10 mg (7.5 mg/m2) of lenvatinib on alternate days with stable disease and a good quality of life.
Patient 2
A 15-year-old male presented with cough, respiratory distress, and hypoxia requiring supplemental oxygen. An initial chest radiograph showed diffuse micronodular opacities, and he was started on a four-drug regimen for empiric tuberculosis treatment. Acid-fast bacilli stain was negative. A neck and chest CT showed a 1.5 cm calcified thyroid nodule in the left thyroid lobe, with extensive cervical and superior mediastinal lymphadenopathy, as well as innumerable bilateral pulmonary lesions (Fig. 1C). Fine-needle aspiration cytology of a left level III cervical lymph node demonstrated PTC. His Tg at diagnosis was 931 ng/mL. He subsequently underwent total thyroidectomy, bilateral central and modified lateral neck dissection, and left parapharyngeal space tumor removal. The surgical pathology demonstrated multifocal PTC with mixed classical and follicular features. Extrathyroidal extension was present, and bilateral lymph nodes were positive for disease. The TNM staging at diagnosis was T4aN1bM1.
Postoperative whole-body nuclear scintigraphy showed no iodine uptake in the neck or lungs. Due to his extensive pulmonary disease burden with no iodine avidity on whole-body scintigraphy, he was not deemed a candidate for RAI therapy. He was started on oral lenvatinib at a dose of 24 mg daily (14 mg/m2/day), which was reduced to 14 mg daily after three weeks due to development of palmar-plantar erythrodysesthesia. A chest CT one month after starting lenvatinib showed overall decreased size of the innumerable pulmonary nodules (Fig. 1D). He was weaned off oxygen six weeks after the initiation of lenvatinib. Three months after starting lenvatinib, a CT of the neck and chest showed no residual thyroid tissue, stable cervical lymph nodes with minimal enhancement, and stable pulmonary nodules. The Tg level decreased from 931 to 416 ng/mL and subsequently ranged from 215 to 344 ng/mL. A CCDC6–RET fusion was identified through a comprehensive genomic panel for solid tumors. Three months after starting lenvatinib, therapy was held briefly due to grade 3 proteinuria, and he was restarted on a lower dose at 10 mg per os once a day (6 mg/m2/day). He has had no other significant side effects secondary to lenvatinib. Eleven months after starting lenvatinib, he was clinically stable on lenvatinib 6 mg/m2/day, with no oxygen requirement or evidence of progression.
Patient 3
A five-year-old male with a history of atrial septal defect and ventricular septal defect repair presented with neck swelling. An initial chest CT showed extensive cervical, supraclavicular, mediastinal, and right hilar lymphadenopathy with innumerable bilateral pulmonary nodules. Fine-needle aspiration cytology of a right supraclavicular lymph node demonstrated PTC. He underwent a near total thyroidectomy with bilateral central and lateral lymph node dissection, and a thoracotomy with resection of the bulky mediastinal component. The TNM staging at diagnosis was T4aN1bM1.
Two months after surgery, he underwent RAI (131I) with 65 mCi after stimulation with recombinant human thyrotropin. Eight months after receiving RAI treatment, the Tg decreased from 16,420 ng/mL at diagnosis to 500 ng/mL. However, one month later, the level increased to 2154 ng/mL. He received an additional 65 mCi of RAI, with a subsequent decrease of his Tg level to 1409 ng/mL two months later. The Tg level gradually increased to 2505 ng/mL, and 15 months following his second RAI treatment, he presented with dyspnea with exertion. He had a new oxygen requirement of 1 L/min. A chest CT showed interval worsening of multiple pulmonary nodules (Fig. 1E). He was started on lenvatinib 14 mg/m2/day once daily per os. He was weaned off oxygen one day after starting lenvatinib. He experienced an improvement in appetite and energy level shortly after starting this therapy. Radiographic improvement was noted one month after starting lenvatinib, and a chest CT showed a decrease in the overall burden of pulmonary nodules (Fig. 1F). He tolerated lenvatinib well, with no side effects. The tumor was BRAF negative, and RNA sequencing of the tumor demonstrated a SQSTM1-NTRK3 fusion. Despite having clinical and radiographic improvement with lenvatinib, therapy was subsequently changed to larotrectinib, an inhibitor of tropomyosin receptor kinases (TRK). Five months after starting targeted therapy, he remained clinically stable, with no evidence of disease progression.
Discussion
Children with PTC have a higher incidence of lymph node and/or pulmonary involvement when compared to adults with PTC. In a retrospective review, 44.5% of children with PTC presented with local or distant metastases (19). Patients with extensive, multifocal PTC with metastases at diagnosis are at greatest risk for recurrence (19). The American Thyroid Association (ATA) Task Force published guidelines for the evaluation and management of thyroid nodules and DTC in children and adolescents (20). Per the ATA risk classification for pediatric thyroid cancer, the patients presented here are at high risk for recurrent and/or persistent disease, given their extensive multifocal disease with pulmonary metastasis, and the ATA recommendations include a total thyroidectomy and surgical resection of involved lymph nodes followed by RAI. Rarely, children present with PTC that is not amenable to surgery or RAI or becomes refractory to RAI. In such cases, systemic therapy may be an option. The patients here presented with extensive and symptomatic disease not amenable or refractory to RAI, and therefore targeted therapy was administered.
The activity of tyrosine kinase inhibitors has been well documented in adults with PTC (14,15,21). In a multicenter, randomized, double-blind, Phase III clinical trial in adults with refractory differentiated thyroid cancer, the median progression-free survival was significantly longer in the sorafenib group (10.8 months) compared to the placebo group (5.8 months) (14). In a similar setting, lenvatinib resulted in a median progression-free survival of 18.3 months compared to 3.6 months for the placebo group (15). In addition, 65% of patients had an objective response to lenvatinib. Both sorafenib and lenvatinib are FDA approved for the treatment of adult patients with locally recurrent or metastatic, progressive, RAI refractory DTC.
There are only a few case reports describing the use of tyrosine kinase inhibitors in children with PTC (16,17). Sorafenib was shown to be beneficial in a pediatric patient with progressive, RAI refractory PTC (16) and in another patient with disease not amenable to upfront RAI therapy (17). The effect of lenvatinib in pediatric patients with PTC has not been described. The first patient in this report was started on lenvatinib after demonstrating clinical worsening with hypoxia and respiratory distress on sorafenib, and showed clinical improvement with overall decreased tumor burden on therapy with lenvatinib. The second and third patients were started on lenvatinib as firs-line therapy, given the efficacy of lenvatinib demonstrated in adults and due to the drug tolerability shown in the Phase I study in children. Similar to the first patient, these two patients showed clinical and radiographic improvement on lenvatinib. Patients had baseline evaluations and routine monitoring for side effects of lenvatinib, with periodic echocardiograms, electrocardiograms, radiographs to assess proximal tibial growth plate, renal and liver functions tests, urinalysis, and frequent blood pressure assessments. Two of the patients experienced proteinuria, and one of them developed palmar-plantar erythrodysesthesia, resulting in dose adjustments. In patients with proteinuria, the creatinine remained normal. The requirement of dose reduction in two of the patients and continued clinical benefit at lower doses suggests that the maximum tolerated dose and clinically active dose may be different for lenvatinib in children. All patients tolerated lenvatinib well, and none of the patients experienced fatigue, diarrhea, or hypertension.
In conclusion, these cases demonstrate that lenvatinib may be a beneficial option for children with advanced PTC that is refractory or not amenable to surgery/RAI treatment. Additionally, lenvatinib may be used as a bridge to surgery or RAI therapy in children whose disease is not amenable to those first-line therapies. The tumors of these patients were negative for BRAF mutations. Furthermore, rearrangement of the RET proto-oncogene was identified in the other two patients, making them potential candidates for alternative targeted therapies should they have progressive disease. Further investigations into the role of molecularly targeted agents in complex, progressive, or refractory pediatric thyroid cancer are warranted.
Footnotes
Acknowledgments
The authors would like to acknowledge the members of our multidisciplinary thyroid cancer program and, above all, our patients.
Author Disclosure Statement
No competing financial interests exist.