
Abstract
Background:
Thyroid peroxidase antibody (TPOAb) positivity can attenuate gestational thyroid responses to human chorionic gonadotropin (hCG) during pregnancy, whereas the effects of thyroglobulin antibodies (TgAb) remain unknown. The aim of our study was to explore the thyroid response to hCG in women with thyrotropin (TSH) levels within the method-specific reference range under different conditions of thyroid autoimmunity.
Methods:
The study screened 822 women at 7–20 weeks of gestation using the pregnancy-specific reference range for TSH. Serum TSH, free thyroxine (fT4), TPOAb, TgAb, and β-hCG levels were measured using electrochemiluminescence immunoassays.
Results:
The enrolled pregnant women were subdivided into four subgroups based on TPOAb/TgAb positivity: co-positive for TPOAb and TgAb (group 1), isolated TPOAb positive (group 2), isolated TgAb positive (group 3), and co-negative for TPOAb and TgAb (group 4). TSH was negatively associated with hCG in all four groups (p < 0.05). fT4 was positively associated with hCG in groups 3 and 4 (p < 0.01) but not in groups 1 (p = 0.096) and 2 (p = 0.758). Group 2 was further stratified into tertiles according to TPOAb concentrations. No negative TSH/hCG association was observed in the middle- and upper-tertile groups when TPOAb were ≥53 IU/mL (p > 0.05). There was no positive fT4/hCG association in any of the three subgroups (p > 0.05). Similarly, group 3 was further stratified into tertiles according to TgAb levels. TSH was negatively associated with hCG in the lower and middle tertiles (p < 0.01), but the association was not found in the upper tertile when TgAb was ≥356 IU/mL (p = 0.191). fT4 was positively associated with hCG in the lower tertile (p = 0.027) but not in subgroups when TgAb was ≥219 IU/mL (p > 0.05).
Conclusions:
When TSH was within the pregnancy-specific reference range, high concentrations of TPOAb and TgAb attenuated the fT4 stimulation and suppression of TSH by hCG. The results imply that TgAb, in addition to TPOAb, could also interfere with thyroidal responses to hCG during the first half of pregnancy.
Introduction
Human chorionic gonadotropin (hCG) is mainly generated by the placenta. Serum hCG levels are detectable at approximately 10 days after ovulation, peaking at 9–11 weeks of pregnancy, declining from approximately 12 weeks until 20 weeks of pregnancy, and then remaining stable for the rest of the pregnancy. Due to the high degree of β-subunit homology between the hCG receptor and the thyrotropin receptor (TSHR), hCG can bind to the TSHR and stimulate the secretion of thyroxine (T4) and triiodothyronine (T3) (1).
During normal pregnancy, large amounts of hCG may have a thyrotropin (TSH)-like effect, promoting the production of free T4 (fT4). Subsequently, such an hCG-mediated increase in serum fT4 is responsible for a decrease in serum TSH concentrations through negative feedback (2). However, it has been reported that thyroidal responses to hCG are impaired in thyroid peroxidase antibody (TPOAb)-positive women (3). A recent study from Unuane et al. found that women with isolated thyroglobulin antibody (TgAb) positivity had a significantly higher TSH level than euthyroid women with euthyroidism (ET) (4). Additionally, Williams et al. found that infants of TgAb-positive mothers scored poorly in perception and motor performance tests (5). However, their study had a small sample size and did not address information on isolated TPOAb positivity versus TgAb positivity. Furthermore, Quinn et al. reported that TSH values were significantly higher in TgAb-positive pregnant women than in women with ET (6). Similarly, Bliddal et al. found a significantly higher proportion of thyroid dysfunction in women with thyroid autoimmunity (TAI) than in women with ET (7). Moreover, according to Liu et al., during pregnancy, the percentage of women co-positive for TPOAb and TgAb in China was markedly higher than that of isolated TPOAb- or TgAb-positive women (6.1% vs. 3.2% and 3.7%; p < 0.05) (8). A previous study found that after mandatory universal salt iodization in China, the prevalence rates of TPOAb positivity (11.5% vs. 9.81%) and TgAb positivity (12.6% vs. 9.09%) were higher than they were 16 years prior (9).
The above studies indicate that the effects of TgAb on pregnant women should not be neglected. Additionally, the latest guidelines published in 2017 recommend screening for TPOAbs and call for studies of TgAbs (10). Therefore, this study aimed to explore thyroidal responses to hCG under different conditions of TAI during the first half of pregnancy in Chinese women.
Methods
Subjects
This study was embedded in the Subclinical Hypothyroid in Early Pregnancy (SHEP) project (8,11,12) in three cities in Liaoning Province in China. Subjects volunteered to participate in this study. All subjects signed informed consent forms before joining the project. Participants visited the hospital between 8:00am and 10:00am, and an oral questionnaire was administered to collect personal information and data on background characteristics. Physicians who had received centralized training performed the basic physical examination, including measurement of height, body weight, blood pressure, heart rate (HR), and thyroid palpation. Maternal age was recorded according to each subject's ID card. The inclusion criteria were: residence in the region for at least five years, singleton pregnancy, aged 19–40 years, in weeks 7–20 of pregnancy, and a TSH level below the upper limit according to the pregnancy and method-specific reference range (7–12 weeks of pregnancy: 4.47 μIU/mL; 13–20 weeks of pregnancy: 4.52 μIU/mL) (11). The exclusion criteria were: multiple pregnancies; personal history of thyroid disease; pregnancy by assisted reproductive technology; use of medications that may affect thyroid function, such as steroids, contraceptives, glucocorticoids, dopamine, antithyroid drugs, or levothyroxine; and a personal history of obstetric or gynecological diseases. A total of 822 pregnant women were enrolled in this study. A flow chart of participant selection is shown in Figure 1.

Flow chart of the study population. Women with ET were selected as controls, and their baseline characteristics were matched with women with TAI. The upper limits for TSH were obtained from the pregnancy and method-specific reference range: 7–12 weeks of pregnancy, 4.47 μIU/mL; 13–20 weeks of pregnancy, 4.52 μIU/mL. TAI, thyroid autoimmunity; TSH, thyrotropin; TPOAb, thyroid peroxidase antibody; thyroglobulin antibody, TgAb; ET, euthyroidism; GA, gestational age at blood sampling.
The gestational age (GA) at blood sampling was calculated based on the last menstrual period (LMP). Maternal age, body mass index (BMI), abdominal circumference (AC), systolic blood pressure (SBP), diastolic blood pressure (DBP), HR, parity (0 or 1+), previous miscarriage (0, 1, or 2+), smoking status (nonsmoker, former smoker, smoker, or passive smoker), and drinking status (nondrinker or drinker) before pregnancy were ascertained.
Study samples and laboratory determinations
Fasting blood samples were obtained from all subjects between 8:00am and 10:00am. The blood samples were centrifuged at 3800 rpm for 10 minutes, and the upper layer of serum was collected and stored at −80°C until further analysis. Serum TSH, fT4, β-hCG, TPOAb, and TgAb levels were measured using electrochemiluminescence immunoassays; β-hCG was diluted 100-fold and measured automatically. All analyses were conducted using a Cobas Eless 601 analyzer (Roche Diagnostics, Basel, Switzerland).
The functional sensitivity of serum TSH was 0.002 μIU/mL. The intra-assay coefficients of variation for TSH, fT4, hCG, TPOAb, and TgAb were 1.57–4.12%, 2.24–6.33%, 1.7–2.8%, 2.42–5.63%, and 1.3–4.9%, respectively, and the inter-assay coefficients of variation were 1.26–5.76%, 4.53–8.23%, 3.3–7.4%, 5.23–8.16%, and 2.1–6.9%, respectively. Based on the reference range provided by the manufacturer, TPOAb was defined as clinically positive at >34 IU/mL; TgAb was clinically positive at >115 IU/mL.
Ethics committee approval
The experimental procedure was authorized by China Medical University (Ethics Committee of China Medical University [2012]2011-32-4) and performed in accordance with the Declaration of Helsinki. All subjects understood and signed the written informed consent form before participating in the study.
Categorization
After exclusions, the cross-sectional study included 822 pregnant women. The participants were divided into four subgroups according to thyroid autoantibodies: group 1, co-positive for TPOAb and TgAb (TPOAb+ and TgAb+); group 2, isolated TPOAb-positive (TPOAb+ and TgAb−); group 3, isolated TgAb-positive (TPOAb− and TgAb+); and group 4, co-negative for TPOAb and TgAb (TPOAb− and TgAb−). To ensure clinical significance and to maintain sameness between the two groups, the isolated TPOAb-positive group and the isolated TgAb-positive group were stratified into tertiles (tertile 1, tertile 2, and tertile 3) based on sample size.
Statistical analysis
A one-sample Kolmogorov–Smirnov test was applied to determine the normality of the distribution for continuous variables. Baseline data are presented as medians (interquartile range [IQR]), and categorical data are presented as percentages. For continuous variables, baseline characteristics of three or four groups were compared by one-way analysis of variance or Kruskal–Wallis test, as appropriate, with post hoc Bonferroni correction. The frequencies of categorical variables were compared utilizing chi-square, Pearson's chi-square, or Fisher's exact test as appropriate.
Correlations between hCG and TSH/fT4 were assessed by a linear correlation model, using Pearson's correlation for normally distributed variables and Spearman's correlation for variables that were not normally distributed. Multivariable linear regression models were performed after adjustment for GA at sampling. A p-value of <0.05 indicated statistical significance. All statistical analyses were performed using IBM SPSS Statistics for Windows v21.0 (IBM Corp., Armonk, NY).
Results
This cross-sectional study consisted of 822 participants: group 1, n = 128; group 2, n = 90; group 3, n = 188; and group 4, n = 416. The isolated TPOAb-positive group (group 2) was then stratified into subgroups: tertile 1 (n = 30), 34 IU/mL < TPOAb <53 IU/mL; tertile 2 (n = 30), 53 IU/mL ≤ TPOAb <117 IU/mL; and tertile 3 (n = 30), TPOAb ≥117 IU/mL. Additionally, the isolated TgAb-positive group (group 3) was stratified into subgroups: tertile 1 (n = 63), 115 IU/mL < TgAb <219 IU/mL; tertile 2 (n = 63), 219 IU/mL ≤ TgAb <356 IU/mL; and tertile 3 (n = 62), TgAb ≥356 IU/mL. Details on each subject's characteristics are presented in Tables 1 –3. GAs in groups 1–3 were different from that of group 4 (p < 0.001). TSH levels in groups 1–3 were higher than that of group 4 (p < 0.05). However, fT4 and hCG levels were comparable among the groups (p > 0.05). Baseline data, including maternal age, BMI, AC, SBP, DBP, HR, parity, previous miscarriage, smoking status, and drinking status were also comparable among the different groups (p > 0.05).
Descriptive Statistics of Women Grouped According to TPOAb/TgAb
All variables are presented as the medians with interquartile ranges. The normal reference ranges for TPOAb and TgAb were obtained from the manufacturer: TPOAb, 0–34 IU/mL; TgAb, 0–115 IU/mL. The upper limits for TSH were obtained from the pregnancy and method-specific reference range: 7–12 weeks of pregnancy, 4.47 μIU/mL; 13–20 weeks of pregnancy, 4.52 μIU/mL.
The p-values for continuous variables comparison were obtained through statistical analyses using one-way analysis of variance adjusted by Bonferroni correction or Kruskal–Wallis test, as appropriate.
The p-values for categorical variables were compared utilizing the chi-square test, Pearson's chi-square test, or Fisher's exact test, as appropriate.
Compared to TPOAb− and TgAb−, p < 0.05.
Compared to TPOAb− and TgAb−, p < 0.001.
Compared to TPOAb+ and TgAb+, p < 0.05.
TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody; GA, gestational age at blood sampling; BMI, body mass index; AC, abdominal circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; hCG, human chorionic gonadotropin; fT4, free thyroxine; TSH, thyrotropin.
Descriptive Statistics of Women Stratified for Isolated TPOAb+
All variables are presented as the medians with interquartile ranges.
The normal reference ranges for TPOAb and TgAb were obtained from the manufacturer: TPOAb, 0–34 IU/mL; TgAb, 0–115 IU/mL.
The upper limits for TSH were obtained from the pregnancy and method-specific reference range: 7–12 weeks of pregnancy, 4.47 μIU/mL; 13–20 weeks of pregnancy, 4.52 μIU/mL.
The p-values for continuous variables were obtained through statistical analyses using one-way analysis of variance adjusted by Bonferroni correction or Kruskal–Wallis test, as appropriate.
The p-values for categorical variables were compared utilizing the chi-square test, Pearson's chi-square test, or Fisher's exact test, as appropriate.
Compared to tertile 1, p < 0.05.
Descriptive Statistics of Women Stratified for Isolated TgAb+
All variables are presented as the medians with interquartile ranges.
The normal reference ranges for TPOAb and TgAb were obtained from the manufacturer: TPOAb, 0–34 IU/mL; TgAb, 0–115 IU/mL.
The upper limits for TSH were obtained from the pregnancy and method-specific reference range: 7–12 weeks of pregnancy, 4.47 μIU/mL; 13–20 weeks of pregnancy, 4.52 μIU/mL.
The p-values for continuous variables were obtained through statistical analyses using one-way analysis of variance adjusted by Bonferroni correction or Kruskal–Wallis test, as appropriate.
The p-values for categorical variables were compared utilizing the chi-square test, Pearson's chi-square test, or Fisher's exact test, as appropriate.
Compared to tertile 1, p < 0.01.
Compared to tertile 2, p < 0.05.
Association of hCG with TSH according to TPOAb/TgAb status
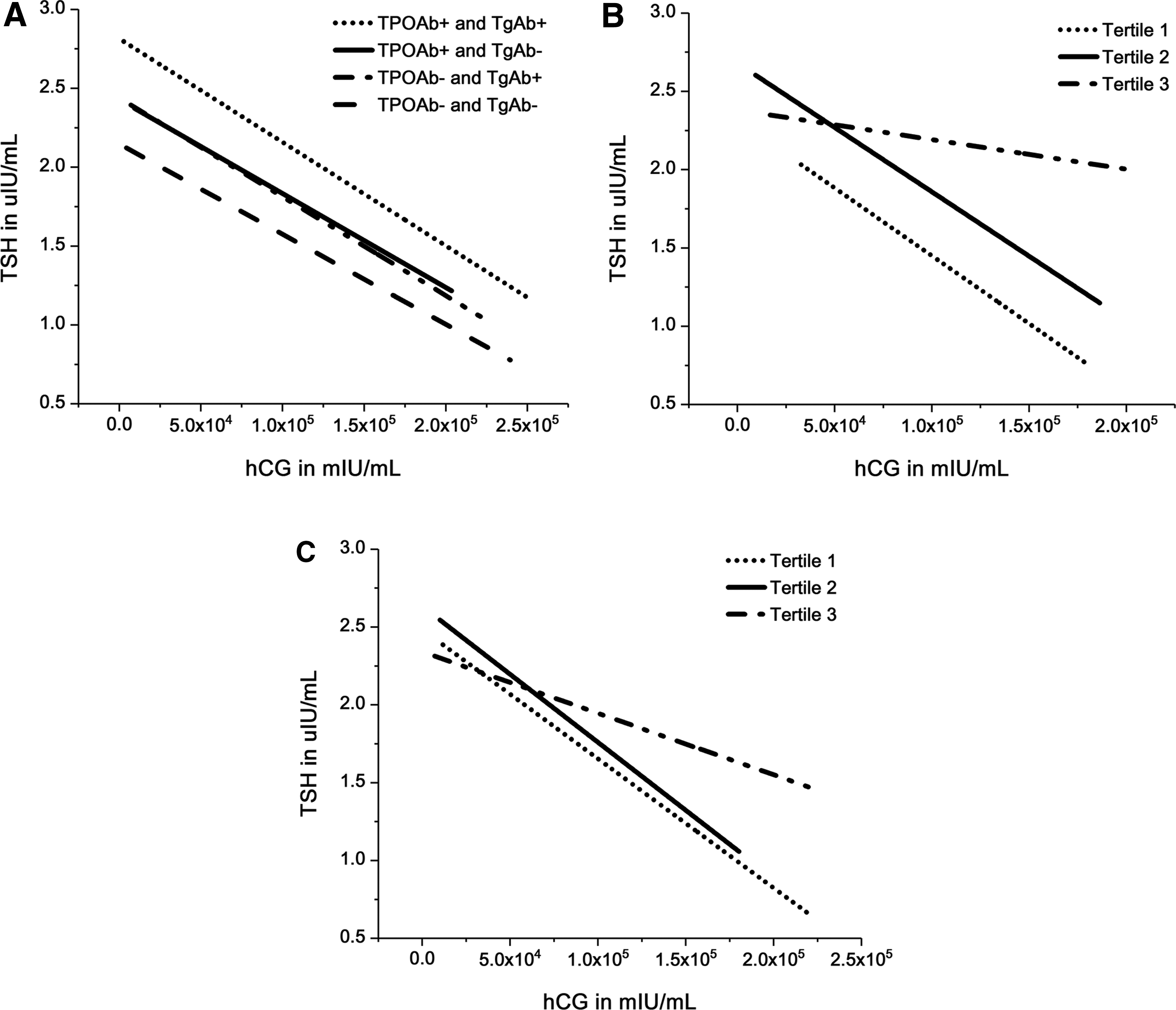
A negative correlation was found between hCG and TSH levels in group 1 (p < 0.0001, r = −0.312), group 2 (p = 0.006, r = −0.275), group 3 (p < 0.0001, r = −0.265), and group 4 (p < 0.0001, r = −0.319). This inverse association remained statistically significant after adjusting for the GA using multivariable linear regression models (Fig. 2A).
Association of hCG with TSH according to TPOAb/TgAb status. (
However, when group 2 was stratified into subgroups, the negative correlation was only present in tertiles 1 (p = 0.03, r = −0.397) and 2 (p = 0.037, r = −0.382) but not tertile 3 (p = 0.679, r = −0.079). Multivariable linear regression analyses confirmed that TSH was negatively associated with hCG in tertile 1 (p = 0.013) but not in tertiles 2 (p = 0.087) and 3 (p = 0.957) when simultaneously adjusting for age (p for trend = 0.004; p for interaction = 0.3873; Fig. 2B). Similarly, group 3 was then subdivided into tertiles for stratification. A negative correlation was observed between TSH and hCG in tertiles 1 (p = 0.001, r = −0.392) and 2 (p = 0.008, r = −0.332) but not in tertile 3 (p = 0.191, r = −0.168). Additionally, multivariable linear regression analyses confirmed similar findings when simultaneously adjusting for GA (p for trend <0.001; p for interaction = 0.4050; Fig. 2C).
Association of hCG with fT4 according to TPOAb/TgAb status
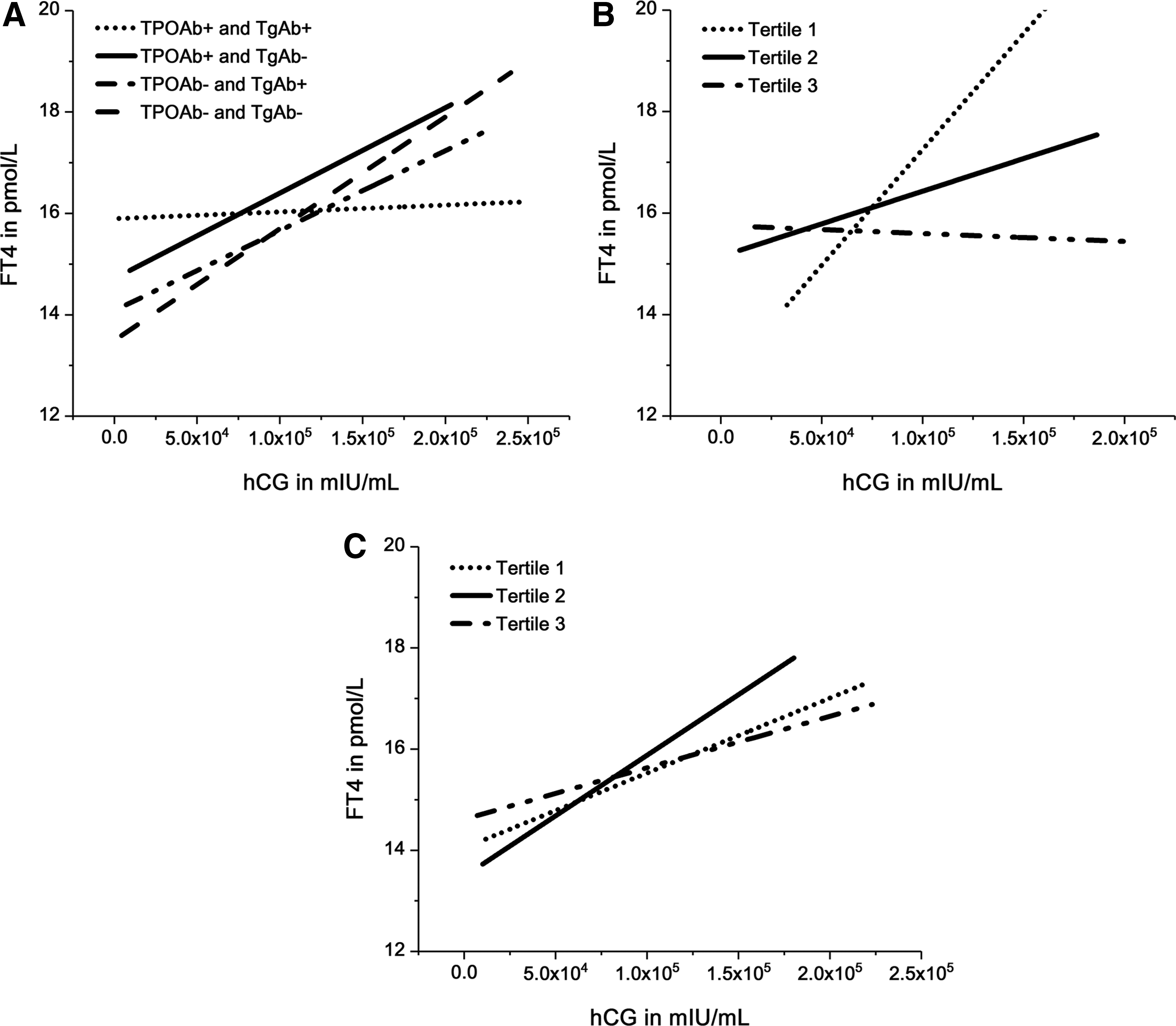
The method of analysis for the fT4/hCG association was the same as that used for TSH. A positive correlation between fT4 and hCG was observed in groups 2 (p = 0.012, r = 0.253), 3 (p < 0.0001, r = 0.313), and 4 (p < 0.0001, r = 0.453) but not in group 1 (p = 0.816, r = 0.021). Nonetheless, the positive association between fT4 and hCG was not statistically significant in group 2 after adjusting for the GA and applying the multivariable linear regression models (p = 0.096; Fig. 3A).
Association of hCG with fT4 according to TPOAb/TgAb status. (
After stratification in group 2, no positive correlation was found between fT4 and hCG in any of the subgroups: tertile 1 (p = 0.055, r = 0.354), tertile 2 (p = 0.349, r = 0.177), and tertile 3 (p = 0.720, r = 0.068). Moreover, multivariable linear regression analyses confirmed the same results after simultaneously adjusting for GA (p for trend = 0.148; p for interaction = 0.1890; Fig. 3B). Additionally, when group 3 was further stratified into tertiles, fT4 was positively associated with hCG in tertiles 1 (p = 0.009, r = 0.325) and 2 (p = 0.005, r = 0.346) but not in tertile 3 (p = 0.098, r = 0.212). Multivariable linear regression analyses confirmed that TSH was negatively associated with hCG in tertile 1 (p = 0.027) but not in tertiles 2 (p = 0.188) and 3 (p = 0.072) when simultaneously adjusting for age (p for trend = 0.003; p for interaction = 0.3431; Fig. 3C).
Discussion
This study shows that similar to TPOAb-positive women, TgAb-positive women could also display an impaired thyroidal response to hCG. When the TSH level was within the pregnancy-specific reference range, only high titers of thyroid antibodies attenuated the suppression of TSH by hCG (TPOAb ≥53 IU/mL or TgAb ≥356 IU/mL). In contrast, women with TPOAb positivity (TPOAb >34 IU/mL) or high concentrations of TgAb (TgAb ≥219 IU/mL) failed to respond adequately to hCG stimulation.
The study measured β-hCG levels, including intact hCG, nicked hCG, the β-core fragment, and the free β-subunit, instead of total hCG. The β-subunits of hCG are reported to be distinct from other hormones and confer receptor and biological specificity (13 –15). Additionally, both intact hCG and β-hCG are reported to have inverse associations with TSH (p < 0.05) (16). Furthermore, in 2001, Yeo et al. found that both total and free β-hCG were negatively correlated with TSH (r = −0.30, p < 0.0001 and r = −0.290, p < 0.0001, respectively) and positively correlated with fT4 (r = 0.283, p < 0.001 and r = 0.253, p < 0.001, respectively) (17). As the free β-hCG assay allows for direct measurements on serum samples from pregnant women, this assay is an attractive alternative to the total β-hCG assay (17). Furthermore, a previous study found that TSH decreases significantly from the seventh week of pregnancy and is negatively correlated with β-hCG (12). Consequently, in this study, women at 7–20 weeks of pregnancy were selected as subjects, and the serum β-hCG levels were measured.
Many studies have focused on the association between hCG and maternal thyroid function during pregnancy. In 1990, Glinoer et al. examined 606 healthy pregnant women and found that there was a clear mirror image between the decrease in individual TSH and the increase in hCG throughout pregnancy (18). They also found that hCG stimulated fT4 release and had a TSH-like effect. The results of this study are in accordance with this previous study. However, the study by Glinoer et al. did not evaluate the effects of thyroid antibodies.
In 2017, Korevaar et al. found that TPOAb impaired the thyroid response to hCG. There was a negative TSH/hCG correlation and a positive fT4/hCG correlation in TPOAb-negative (TPOAb <60 IU/mL) but not in TPOAb-positive (TPOAb >60 IU/mL) women (3). The present findings that pregnant women with high concentrations of TPOAb (TPOAb ≥53 IU/mL) had inadequate thyroidal response to hCG are consistent with the study by Korevaar et al.
Regardless, previous studies have only analyzed the influence of TPOAb, and it remains unknown whether TgAb can affect the maternal thyroid response to hCG during pregnancy. In addition to the TPOAb-positive and -negative groups, this study also analyzed groups co-positive for TPOAb and TgAb, co-negative for TPOAb and TgAb, isolated TPOAb-positive, and isolated TgAb-positive. Furthermore, the isolated TPOAb-positive group and isolated TgAb-positive group were stratified into subgroups. It was found that TSH was not suppressed by hCG when thyroid antibody concentrations were high (TPOAb ≥53 IU/mL or TgAb ≥356 IU/mL). In addition, TPOAb positivity (TPOAb >34 IU/mL) or high levels of TgAb (TgAb ≥219 IU/mL) were responsible for attenuated fT4 stimulation.
A small difference was found in the TPOAb cutoff values between this study and the study by Korevaar et al. (3). Variations in hCG levels and thyroid function by race/ethnicity and residence area may account for the slight diversity (19). O'Brien et al. also reported that Asian women have higher hCG levels than white and Hispanic women (18).
The degree of lymphocytic infiltration has been shown to be positively correlated with TPOAb (20,21) and TgAb concentrations (22). As a result, individuals with higher antibody concentrations tend to suffer from more severe lymphocytic infiltration (20). Impairment of the thyroid response was also related to the TPOAb/TgAb titers. Thus, it was hypothesized that lymphocytes may result in impairment via interference with hCG bioactivity, which is determined by desialylation and half-life of hCG (23). Women with high TPOAb/TgAb titers may have reduced production of desialylated hCG by trophoblast cells or a shorter hCG half-life in plasma, eventually resulting in decreased bioactivity. Moreover, Csaba proposed the immune-endocrine system concept, suggesting that the TRH–TSH–T3 axis could play an important role in regulating immune function (24). hCG can be synthesized and secreted by natural killer cells and monocytes (25). TSH can be produced by lymphocytes (26). Additionally, Alexander et al. reported that interleukin (IL)-1β, IL-4, IL-6, IL-10, tumor necrosis factor alpha, and granulocyte-macrophage colony-stimulating factor can stimulate hCG production by mononuclear cells, while interferon gamma and IL-2 differentially inhibit the inflammatory microenvironment (25). Therefore, higher antibody concentrations are correlated with increases in lymphocytes and cytokines and severe impairment.
This study has several limitations. The GA was calculated using the LMP instead of an ultrasound estimate. A small difference existed in the GA calculations between the two methods. In Asian women, the GA estimated by LMP and ultrasound was moderately concordant (concordance correlation coefficient = 0.63) and correlated (intraclass correlation coefficient = 0.78) (27). Therefore, estimation of the GA using the LMP is valid. Another limitation of this study is that TRAb levels were not measured. Extremely strict inclusion criteria were used, and women with a personal history of thyroid disease were excluded. In addition, the prevalence of Graves' disease is fairly low in China (0.8%) (9). Therefore, the possibility of including pregnant women with Graves' disease was very low. Third, we did not analyze associations between pregnancy outcomes and concentrations of thyroid antibodies in this study. However, a previous study found that compared to euthyroid women, the risk of miscarriage was significantly higher among women with isolated TAI (TPOAb- and/or TgAb-positive; 5.7% vs. 2.2%; odds ratio [OR] = 2.71 [confidence interval (CI) 1.43–5.12], p = 0.003). Additionally, a graded increase in miscarriage risk was observed as maternal TSH concentrations increased. This effect was augmented by the presence of isolated TAI (8). A meta-analysis conducted by Thangaratinam et al. selected 30 articles with 31 studies (19 cohort and 12 case-control) involving 12,126 women that assessed the association between TAI and miscarriage, and five studies with 12,566 women that evaluated the association with preterm birth. They found that the presence of maternal isolated TAI is strongly associated with miscarriage (for cohort studies: OR = 3.90 [CI 2.48–6.12], p < 0.001; for case-control studies: OR = 1.80 [CI 1.25–2.60], p = 0.002) and preterm delivery (OR = 2.07 [CI 1.17–3.68 ], p = 0.01) (28). Therefore, these studies may contribute to the understanding of one of the negative effects of isolated TAI.
Taken together, in addition to TPOAb, high concentrations of TgAb may also impair the thyroidal response to hCG during pregnancy. Thus, with respect to both TPOAb and TgAb, TAI may decrease the functional capacity of the thyroid gland during first half of pregnancy in Chinese women. These findings indicate that TPOAb as well as TgAb should be considered when evaluating thyroid function in pregnant women. Additional studies are needed to replicate these findings and clarify the detailed mechanisms further.
Footnotes
Acknowledgments
We appreciatively acknowledge the invaluable contribution of doctors from the Gynecology and Obstetrics clinics in 13 hospitals and six prenatal clinics in Liaoning Province and are indebted to the pregnant women who participated in this study. The study was supported by Chinese National Natural Science Foundation (81570709, 81170730); the National Science and Technology Support Program (2014BAI06B02); Research Foundation of Key Laboratory of Endocrine Diseases, Department of Education in Liaoning Province China (LZ2014035); Key Platform Foundation of Science and Technology for the Universities in Liaoning Province (16010); and Health and Medicine Research Foundation, Shenyang City (17-230-9-02).
Author Disclosure Statement
The authors have no potential conflicts of interest to declare.