
Abstract
Background:
Thyroid-stimulating hormone (TSH) receptor (TSHR) antibodies (TRAb) can be present in chronic autoimmune thyroiditis. Transplacental TRAb transfer can lead to fetal thyroid dysfunction and serious complications.
Patient Findings:
We report the case of a woman with autoimmune hypothyroidism and extremely high TRAb levels, with blocking and stimulating activities (biological activities characterized with Chinese hamster ovary cells expressing TSHR). At week 22 of her first pregnancy, sonography detected fetal growth retardation and cardiac abnormalities (extreme tachycardia, right ventricular dilatation, pericardial effusion). The mother's TRAb level, assayed later, was 4030 IU/L (n < 10). Delivered via caesarean section gestational week 30, the newborn girl had several malformations, signs of malnutrition, goiter and hyperthyroidism associated with elevated TRAb (1200 IU/L). The newborn died 26 days after delivery. Faced with persistently high TRAb levels and a desire to become pregnant again, the woman was treated with three consecutive 740-MBq activities of iodine-131, which resulted in a decrease in TRAb to 640 IU/L. The patient had two subsequent pregnancies 16 and 72 months after the radioiodine administration. During the close follow-ups, fetal development was normal, and initial TRAb levels during the two pregnancies were 680 and 260 IU/L, respectively, which initially decreased but then increased in late pregnancy. In both cases, labor was induced at 34 weeks. The newborns, mildly hyperthyroid at birth, required carbimazole treatment at days 5 and 2, respectively. The mild hyperthyroidism despite high TRAb levels was likely due to the concomitant presence of stimulating and blocking TRAb. The two girls, now aged 12 and 8 years, are in good health. The mother has no detectable thyroid gland tissue and is euthyroid on levothyroxine (175 μg/d). Her TRAb level gradually decreased to 136 IU/L.
Summary and Conclusions:
This remarkable case illustrates the severe consequences of untreated fetal hyperthyroidism and the need to assay and follow-up TRAb levels in women of reproductive age with autoimmune thyroiditis.
Introduction
The presence of thyrotropin (TSH) receptor antibodies (TRAb) in patients with chronic autoimmune thyroid disease associated with hypothyroidism (Hashimoto's disease) (1) has been documented for decades (2,3) and can combine stimulatory and/or blocking activity (thyroid stimulating antibody and TSH-stimulation blocking antibody) (4). Fetal hypothyroidism due to the presence of maternal blocking TRAb has been reported, representing approximately 1% of congenital hypothyroidism cases (5). Fetal hyperthyroidism may also occur in patients with autoimmune thyroiditis (6 –8). We report an exceptional case of a woman treated for hypothyroidism since adolescence with dramatically high TRAb levels, which were presumably responsible for the neonatal death of her first child. In contrast, the subsequent two pregnancies progressed favorably after radioiodine ablation of thyroid tissue and a significant reduction of the TRAb levels.
Patient
The patient was diagnosed at 14 years of age with Hashimoto's thyroiditis and presented a firm goiter, high TSH (52.4 mIU/L), antithyroperoxidase, and antithyroglobulin antibody levels, and a positive TRAb assay (83%, n < 15%; commercial radio-receptor assay, TRAK-Henning).
Her first pregnancy (at 26 years of age) was considered normal until the 22nd week, when a fetal ultrasound indicated severe growth retardation, tachycardia of >220 bpm, right ventricular dilatation, and pericardial effusion. The mother was then closely monitored in a tertiary center. At 27 weeks, the fetal thyroid gland was enlarged [22 × 17 mm; estimated thyroid perimeter, 6.2 cm; reference range, 2.7–4.4 cm (9)]. The mother's TRAb levels were 2800 and 4030 IU/L (TRAK Human, Thermo Fisher Scientific, Clinical Diagnostics, B.R.A.H.M.S GmbH; reference level <10 IU/L) at 26 and 29 weeks of gestation, respectively. The mother was clinically euthyroid throughout the pregnancy, although the typical initial levothyroxine dosage (125 μg/day) was reduced to 50 μg/day because serum TSH levels decreased from 0.4 to 0.05 mU/L.
At 30 weeks and 2 days, an unplanned caesarian delivery was performed due to full cervical dilation and breech presentation. The newborn girl had the following characteristics: Apgar score, 1/1/8; weight, 1240 g (25th percentile for age); height, 35.5 cm (10th percentile); head circumference, 24.5 cm (10th percentile); markedly reduced anterior fontanelle; microcephaly; dysmorphic facies; abnormal ear folding; microretrognathia; and apparent microphthalmia. The newborn presented markedly underdeveloped subcutaneous adipose tissue, enlarged liver and spleen, jaundice, elevated conjugated bilirubin levels, thrombopenia, anemia and disseminated intravascular coagulation. The infant's thyroid gland was significantly enlarged, and blood glucose was undetectable. Cardiac ultrasonography revealed cardiomyopathy and an interatrial septal aneurysm bulging into the right atria, while a brain magnetic resonance imaging showed a triventricular hydrocephalus related to cortical atrophy. The electroencephalogram showed low voltage and poorly differentiated activity, and thyroid function tests confirmed the newborn's hyperthyroidism (Table 1), with a TRAb level of 1200 IU/L (TRAK Human, B.R.A.H.M.S GmbH). Antithyroid drug treatment was not initiated because the hyperthyroidism did not appear predominant, given the clinical malformation and lack of marked tachycardia. The mother's thyroid parameters were normal (TSH, 2.6 mU/L; free thyroxine [fT4], 12.6 pmol/L; free triiodothyronine [fT3], 5.8 pmol/L), with TRAb unchanged at 2520 IU/L.
Postnatal Thyroid Hormone and Thyrotropin Receptor Antibodies Levels in the Three Children
Reference ranges: Newborn 1, TSH 0.2–4 mIU/L, FT4 10–26 pmol/L, FT3 3–7 pmol/L, and TRAb <10 IU/L. Newborns 2 and 3, TSH 0.27– .2 mIU/L, FT4 12–21.9 pmol/L, FT3 3.08–6.8 pmol/L; and TRAb <2 IU/L.
TRAK Human, (Thermo Fisher Scientific, Clinical Diagnostics, B.R.A.H.M.S GmbH), normal <10 IU/L.
FT3, free triiodothyronine; FT4, free thyroxine; TRAb: thyrotropin receptor antibodies; TSH, thyrotropin.
The newborn's neurological and cardiorespiratory status worsened progressively, with persistent hyperthyroidism (TSH <0.1; fT4, 24 pmol/L; fT3, 13 pmol/L), and she died 26 days after delivery. The autopsy revealed a fibrosing and necrotizing cholestatic liver without inflammation or steatosis. The autopsy also revealed cardiomyopathy, hypertrophy of the visceral brown fat surroundings the kidneys, adrenal glands, pancreas, and in the mediastinum; her subcutaneous white fat was nearly absent. Polymicrogyria affected the entire brain and was associated with astrocyte gliosis within the white matter and atrophy of the pyramidal tract, while the basal ganglia were normal. The thyroid was notably enlarged, very firm and homogeneous.
Five months postpartum, the mother was clinically euthyroid, her goiter was small (30 mL) firm and indolent. However, her levothyroxine dosage was increased from 50 to 100 μg/d (TSH, 20 mIU/L). Her serum TRAb level was >40 IU/L at a 1/100 serum dilution. The TRAb biological activity was assayed as previously described (Table 2) (10,11). Both stimulating and blocking activities were elevated up to a serum dilution of 1/400 (Table 2).
Maternal Anti-TSH Receptor Antibody Biological Activity
TRAb values were quantified using a commercially available radioreceptor assay kit (TRAK human, Thermo Fisher Scientific, Clinical Diagnostics, B.R.A.H.M.S GmbH).
TRAb biological activities assays: thyroid-stimulating hormone receptor–expressing Chines hamster ovary cells (11) were incubated with test serum or control serum. For blocking activity assay, medium was supplemented with bovine TSH (0.1 mIU/mL). After incubation, cAMP released from the cells was measured by radioimmunoassay. Stimulating activity was expressed as a percentage of the cAMP basal production. Blocking activity was calculated as follows: [1 − (a/b)] × 100, with (a) cAMP generated in the presence of the patient's serum + bTSH and (b) cAMP generated in the presence of normal sera + bTSH (10).
cAMP, cyclic adenosine monophosphate; P1, first pregnancy; P2, second pregnancy; P3 third pregnancy.
Given the mother's strong intention to conceive again, her TRAb levels were the main concern. Given the steady elevated TRAb levels over 34 months (Table 2), we elected thyroid tissue ablation (with the patient's informed consent) to lower the TRAb level. We chose to administer radioiodine (12), and the patient agreed to delay the pregnancy for at least one year. At the age of 29 years, the patient was administered three consecutive 740-MBq iodine-131 activities (uptake, 5.77%) at 3-month intervals on an outpatient basis in accordance with French nuclear medicine regulation. Although the patient showed no signs of orbitopathy, she was administered oral prednisone at 1 mg/kg/day for one week, tapered over 1 month, a dosage adapted from Bartalena et al. (13). The subsequent decrease in thyroid volume and serum TRAb levels are shown in Figure 1.
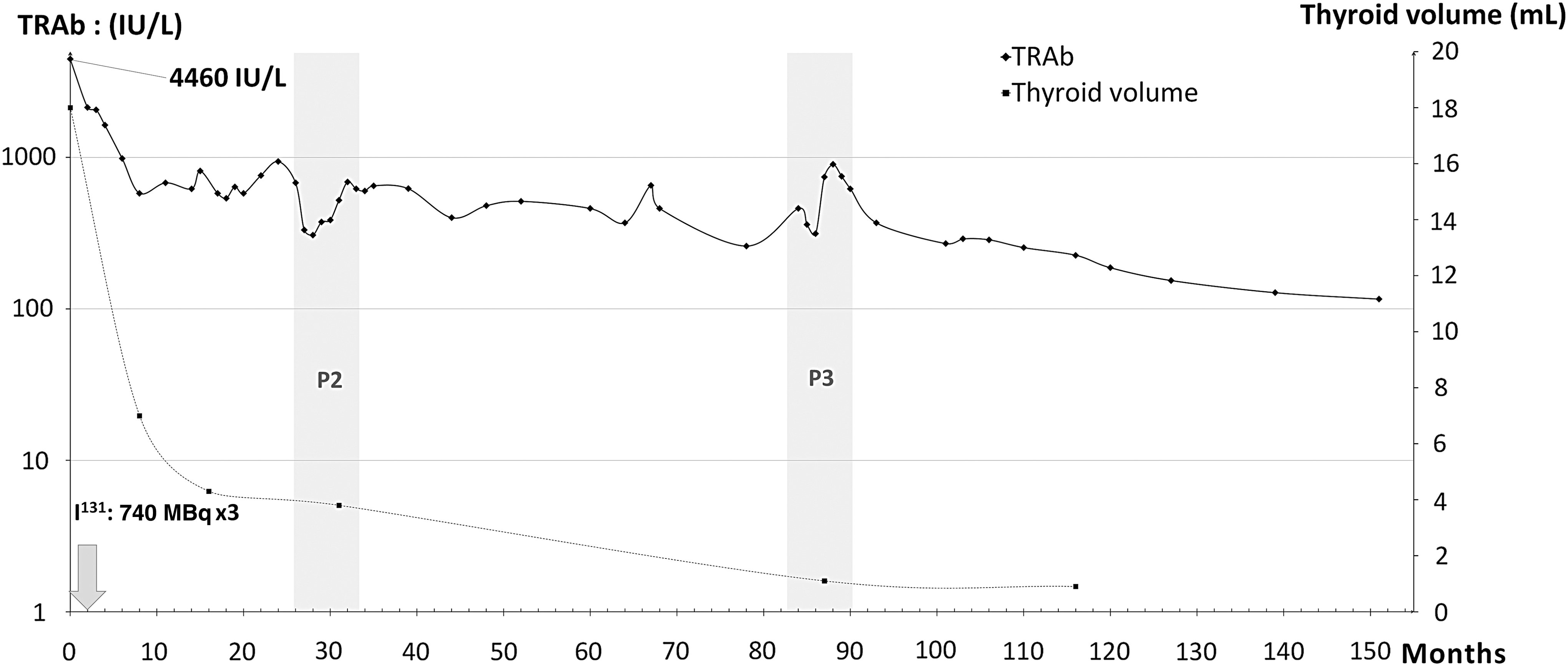
Long-term progression of serum level of thyrotropin receptor antibodies (TRAb; continuous line) and thyroid volume (dotted line) following the administration of three consecutive 740 MBq doses of iodine-131 three months apart. P2 (shaded area): second pregnancy; P3 (shaded area): third pregnancy. Serum TRAb levels: notice the logarithmic scale. Abscissa (x-axis), months since the first radioiodine administration.
The second pregnancy commenced nearly 2 years later, with an initial TSH level of 2.6 mIU/L and TRAb level of 680 IU/L, which decreased to 307 IU/L at 20 weeks and then increased to 620 IU/L in late pregnancy (Figure 1). Biological assays showed both stimulating and blocking activities (Table 2). Fetal development was normal, with no signs (heart, growth, ossification points) of hyperthyroidism, and the cerebral magnetic resonance imaging results were normal. With the mother's consent, labor was induced at 34 weeks and 2 days. The newborn girl was healthy (weight, 2360 kg [+0.5 SD for gestational age]; height, 47 cm [+1 SD]; head circumference, 32 cm [+1 SD]), and her thyroid was moderately enlarged. She initially had mild hyperthyroidism. Due to the increase in fT4 and fT3 (Table 1), the infant was started on carbimazole treatment (3 mg/d) at day 5, resulting in a rapid correction of fT4 and fT3, and the treatment was then tapered off and stopped at 9 weeks; TRAb was then no longer detectable.
Similarly, the third pregnancy 4 years later progressed normally. The mother's initial TRAb level was 260 IU/L, which increased to 621 IU/L (Fig. 1 and Table 2). Labor was once again induced at 34 weeks and 2 days. The newborn girl was healthy, with anthropometric indices at +1 SD for gestational age. At day 2, the infant's fT4 level was markedly elevated (Table 1), and she was treated with carbimazole for 10 weeks. The mother's TRAb levels further decreased to 116 UI/L, and her thyroid was undetectable on ultrasonography. The daily levothyroxine dosage (initially 125 μg/d) was increased to 175 μg to maintain euthyroidism. The two girls (now aged 12 and 8 years) are in good health, have no thyroid abnormality and are doing well in school.
Discussion
This case of fetal hyperthyroidism illustrates the potential damage resulting from the presence of TRAb in a woman with autoimmune thyroiditis and treated hypothyroidism. Although this uncommon association is well known, assaying TRAb in this circumstance—or, as in our case, following-up serum TRAb levels longitudinally—is not the rule. TRAb are therefore likely to be discovered during pregnancy only in the context of fetal hyperthyroidism or during neonatal hypothyroidism screening, depending on the dominant biological TRAb activity. In our case, fetal hyperthyroidism was suspected during the first pregnancy at 22 weeks of gestation, due to the combination of severe manifestations likely related to the extremely high serum TRAb concentration. These manifestations included extreme tachycardia, growth retardation, and thyroid gland enlargement, confirmed at birth by craniosynostosis-related microcephaly, extreme thinness, and the presence of a goiter. Cardiomyopathy, hepatosplenomegaly, jaundice, thrombocytopenia, and intravascular disseminated coagulation could also be related to a severe form of fetal hyperthyroidism (7,14 –16). Unfortunately, no antithyroid drug treatment was administered to the levothyroxine-treated mother to treat the fetus (17). The mother was clinically euthyroid on levothyroxine despite a drop in TSH levels during pregnancy in the absence of hyperemesis gravidarum, which resulted in a decrease in the usual levothyroxine dosage. Unfortunately, (F)T4 readings were not performed; hence, it cannot be determined whether the dose reduction was indeed appropriate. It should be noted that the usual levothyroxine dosage had to be restored five months postpartum (18). Whether the newborn's facial malformation and cerebral abnormalities observed at autopsy were related to the fetal hyperthyroidism remains uncertain (19).
Given the mother's and neonate's very high serum TRAb levels, it is surprising that the neonate's fT4 and fT3 levels on day 1 were only in the upper reference range and less than twice the upper reference range, respectively. In autoimmune thyroiditis, as well as in Graves' disease, stimulating and blocking TRAb activities may coincide or their relative concentrations may vary over time (20,21). In our patient, TRAb bioassays repeatedly showed the presence of stimulating and blocking activities. While detecting blocking activities is hampered by the presence of a concomitant potent stimulatory activity, the patient's serum still elicited a significant blocking activity (55%) at a 1/200 serum dilution against a 782% stimulatory activity, a level that does not interfere with detecting the blocking activity (22). It could be reasonably suggested that the moderate degree of hyperthyroidism in the second and third child, despite still significant TRAb levels, and the delayed neonatal hyperthyroidism, could be explained by the coexistence of stimulating and blocking TRAb activities (7). The mother's need for a higher levothyroxine dosage after thyroid ablation could be explained by the persistence of functional thyroid tissue.
Given the strong desire for future pregnancies, the other main issue consisted in the presence of persistently elevated TRAb levels of approximately 4000 IU/L for more than two years after the first pregnancy. Thyroid tissue ablation was therefore performed to lower these levels. With informed consent from the patient, a high-school mathematics teacher, we chose radioiodine over thyroidectomy to avoid the risk of surgical complications. Three months after the last treatment, the TRAb level fell below 1000 IU/L and steadily declined thereafter. Consequently, there were no signs of fetal hyperthyroidism and only mild initial biological hyperthyroidism during the two subsequent closely monitored pregnancies, consistent with the decrease of the elevated TRAb levels (range, 260–680 IU/L). In contrast to Graves' disease, the TRAb levels during these two pregnancies presented a biphasic pattern, with a small initial dip followed by a significant rise during the second half of pregnancy. Given the unfortunate outcome of the first pregnancy, labor induction at 34 weeks (with the patient's informed consent) provided a satisfactory balance between the risk of prematurity (23) and the development of fetal hyperthyroidism. The second and third neonates, who had hyperthyroidism on days 1–2, had a similar progression of fT4 and fT3 levels, reaching higher values on days 4–5, and requiring antithyroid drug treatment (7,24).
In conclusion, this case illustrates the usefulness of detecting TRAb in women of reproductive age with autoimmune thyroiditis, regardless of thyroid status, and illustrates the impact of ablative therapy on consistently elevated TRAb levels.
Footnotes
Acknowledgments
We would like to thank José Grulet for his valuable contribution in creating the main figure. We would also like to thank Prof. Sophie Collardeau-Fracon for providing additional autopsy information and Alpha Diallo for his corrections.
Author Disclosure Statement
All authors declare that they have no conflicts of interest.