
Abstract
Background:
The 2015 American Thyroid Association guidelines recognize active surveillance as an alternative to immediate surgery in patients with papillary microcarcinomas (PMCs). As a way to incorporate active surveillance as one of the management options for patients with PMCs, we developed and tested a tool to support conversations between clinicians and patients with PMCs considering treatment options.
Methods:
Thyroid Cancer Treatment Choice was developed using an iterative process based on the principles of interaction, design, and participatory action research. To evaluate the impact of the tool on treatment choice, a prospective study was conducted in two thyroid cancer clinics in Seongnam-si and Seoul, South Korea. Both clinics had the expertise to offer active surveillance as well as immediate surgery. One clinic was trained in the use of the conversation aid, while the other clinic continued to care for patients without access to the conversation aid.
Results:
Between May 2016 and April 2017, 278 patients, mostly women (n = 220, 79%), were included in the study; 152 (53%) received care at the clinic using the conversation aid. Age, sex, and mean (±SD) tumor size (6.6 ± 1.6 mm and 6.5 ± 1.9 mm) distributions were similar across clinics. Overall, 233 (84%) patients opted for active surveillance and 53 (16%) for thyroid surgery. Patients in the conversation aid group were more likely to choose active surveillance than the patients seen in the usual care clinic (relative risk = 1.16 [confidence interval 1.04–1.29]). Of all patients opting for active surveillance, more patients in the conversation aid group had thyroid cancer nodules >5 mm than in the usual care group (81% vs. 67%; p = 0.013).
Conclusions:
Thyroid Cancer Treatment Choice is an evidence-based tool that supports the presentation of treatment options for PMCs. Pilot testing suggests that this conversation tool increases acceptance of active surveillance, suggesting that this option is an acceptable and preferable alternative for informed patients. Further studies are warranted to confirm this finding.
Introduction
O
Surgical treatment has been the standard of care for biopsy-proven PMCs. Over the last decade, however, an alternative management approach, “active surveillance,” has emerged. Some have named this approach “deferred or delayed surgery” for the minority of patients with PMC that progress during surveillance requiring rescue surgery (9). This delayed surgery is not associated with higher risk of structural recurrent/persistent disease compared to immediate surgery nor does it translate into mortality (10,11). Most of the published data regarding active surveillance comes from the pioneering studies performed in Japan by Miyauchi and Ito et al., who have demonstrated that this alternative approach constitutes a safe and possibly less damaging alternative in properly selected patients with low-risk PMC (10,12 –17). Moreover, Brito et al. have created a clinical framework to facilitate risk stratification when considering an active surveillance alternative to immediate biopsy and surgery in PMC patients and have classified PMC into three categories: ideal, appropriate, and inappropriate as candidates for active surveillance (18). Most recently, the active surveillance approach has being studied in different populations with distinct cultural backgrounds (19 –21). In the United States, the first experience with this approach was published recently, finding that the rates of tumor growth during active surveillance in a U.S. cohort with PTCs measuring ≤1.5 cm were low (22).
The 2015 American Thyroid Association guidelines recognize active surveillance as an alternative to immediate surgery in patients with very low-risk thyroid cancer (23). This technical remark highlights the importance of incorporating the option of active surveillance during the decision making process with patients who have low-risk thyroid cancer. Yet, the implementation of active surveillance as an option in practice has not occurred, as the majority of patients with PMCs undergo thyroid surgery (24). Limited implementation of active surveillance into practice may reflect clinician skepticism about the value of active surveillance, limited trust in the guidelines, or insufficient evidence-based guidance to select patients in whom this approach is appropriate. Furthermore, clinicians may have some difficulty communicating the comparative benefits and downsides of the treatment options. For example, two qualitative studies in patients with PMC demonstrated that they chose surgery unaware of the potential value of active surveillance (25,26). These findings suggest that insufficient clinician–patient communication may be driving the continued use of thyroid surgery as the treatment of choice for PMC. There is a need for tools to implement the recommendation into practice. In particular, there is a paucity of evidence-based conversation tools to support patient-centered conversations about treatment of PMCs between clinicians and patients with PMCs. Conversation aids are tools that can facilitate these conversations and improve the decision-making process (27 –30). Here, the development and initial pilot testing are described of a conversation aid for patients with PMCs and the clinicians caring for them. The goal of this pilot testing is to provide insights about the impact of the tool on the decision process to manage PMCs.
Methods
In collaboration with a multidisciplinary team, participatory action research was applied to design an intervention for use during routine clinical practice. This design-research process is comprised of (i) review and synthesis of the available evidence and analysis of usual practice, (ii) development of an initial prototype, (iii) field testing (i.e., use in real clinical encounters with patients facing the decision of interest and their clinicians) of the prototype in clinical settings under the study team's supervision, and (iv) final refinement through successive iterations and field testing of each emerging prototype.
Synthesis of evidence and real-time observation of clinical encounters
The literature was searched to find evidence regarding the risks and benefits associated with active surveillance and thyroid surgery (lobectomy or total thyroidectomy). Simultaneously, J.P.B. and R.Z. observed 20 usual clinical encounters within the thyroid cancer clinics at Memorial Sloan Kettering Cancer Center (MSKCC) looking for patterns in the patient–clinician conversations regarding the treatment of PMC and the practical concerns patients raised as important (e.g., cost, follow-up, pregnancy). While other study members were passive observers of these consultations, they were permitted to ask clarifying questions once the consultation had concluded. Then, a team of endocrinologists and otorhinolaryngologists was convened to review the summarized evidence and reach agreement on its validity and applicability. The outcome of the process was an evidence table. This table included: (i) an estimate of the frequency of thyroid cancer in the population; (ii) the management options, active surveillance, and thyroid surgery (lobectomy and total thyroidectomy), (iii) the risk of death, metastases, tumor growth, and adverse effects with each option (e.g., permanent and temporary risk of hypoparathyroidism or voice concerns related to surgery); (iv) the planned type and frequency of follow-up; (v) the out-of-pocket costs with each choice; and (vi) the interaction of pregnancy and each management option.
Development of an initial prototype
The summary of evidence was then discussed with a human-centered interaction designer with expertise in shared decision making and decision-aid development (30). The goal of the design process went beyond presenting pros and cons of each management option. The goal was to design a tool that supports patients and clinicians in the process of thinking, talking, and feeling through how to manage the threat of cancer in a person's life. In order to design a tool that promotes shared decision making, several designs principles were followed (Table 1).
The first paper-based decision aid prototype was created through a series of discussions with members of the study team, the designer, clinicians, and a patient advisory group. The initial and subsequent prototypes were piloted in real encounters with patients with PMCs. Members of the research team observed these conversations and obtained feedback from patients and clinicians at the end of each encounter. This field-testing strategy allowed input to be gathered about how the tool facilitated conversations and provided insights into what worked and what did not. For instance, information was captured about content, format, ease of use, and usefulness. In particular, it was noted whether the conversations aided by the tool enabled patients to voice their concerns and discuss the interaction between each option and each patient's context, values, and preferences. Twelve versions were developed and pilot tested until the entire team reached a consensus that the last prototype, Thyroid Cancer Treatment Choice (Fig. 1), was successful in engaging patients in meaningful conversations in which the patients were able to “try on” different treatment options and, with their clinician, find the one that best fit their situation.
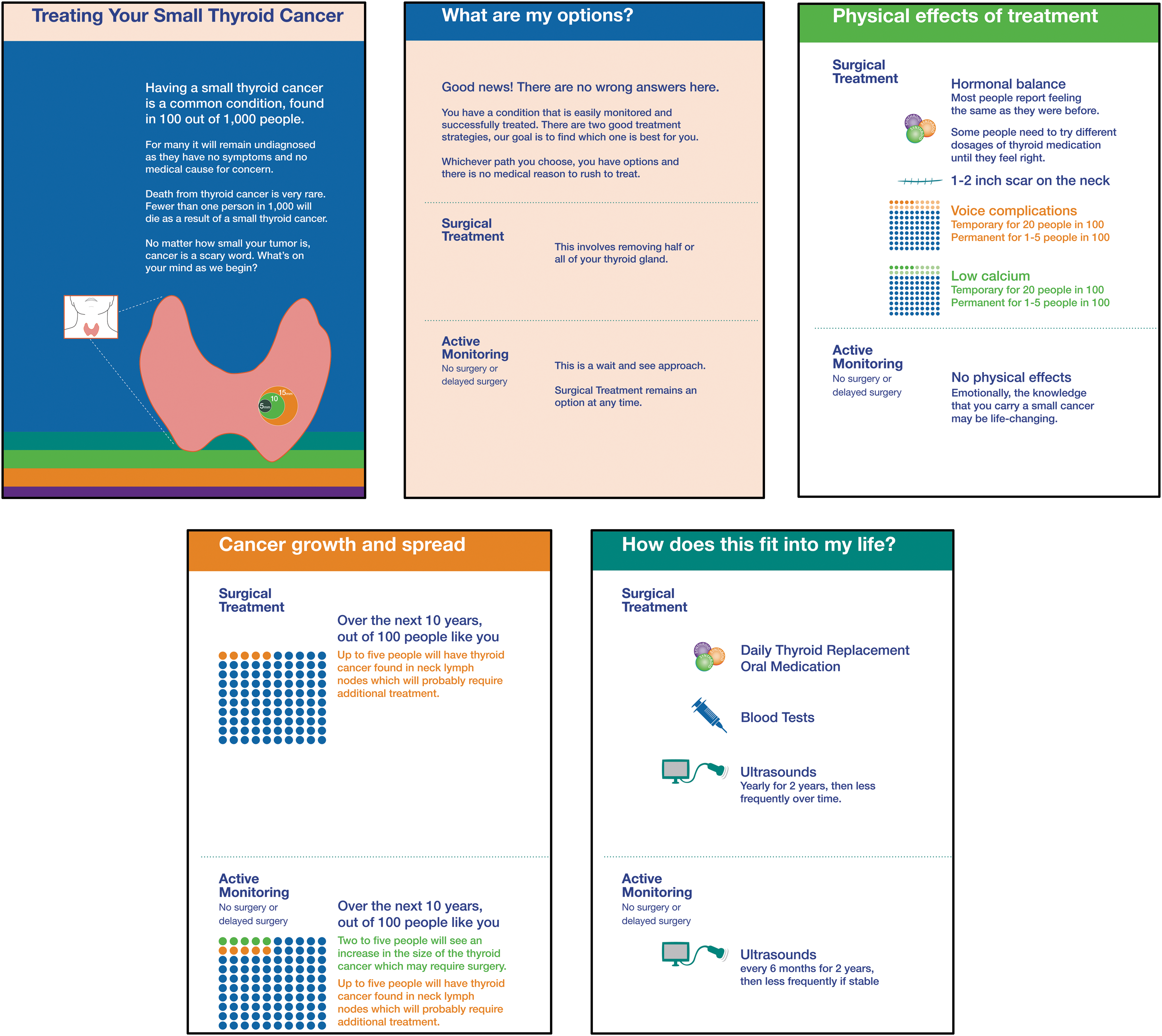
Screen shots of representative cards of Thyroid Cancer Treatment Choice.
Pilot testing: setting and participants
Partnering with colleagues at Seoul National University Hospital and Seoul National University Bundang Hospital, a Korean adaptation (in language and context) of the Thyroid Cancer Treatment Choice was pilot tested in two endocrine clinics. The most important changes to the tool during the adaptation process were a numeric description of the frequency of thyroid cancer in a population based on autopsy studies, and the rates of surgical adverse events and in placing greater emphasis on the thyroidectomy scar (i.e., size description; Fig. 2). Each endocrine clinic has an endocrinologist, rotating students and residents, and allied health staff. Both clinics have expertise in thyroid cancer and have the capacity to offer and follow up patients who choose active surveillance. One clinic was trained in the use of the conversation aid, while the other clinic was told to continue care as usual without the tool.
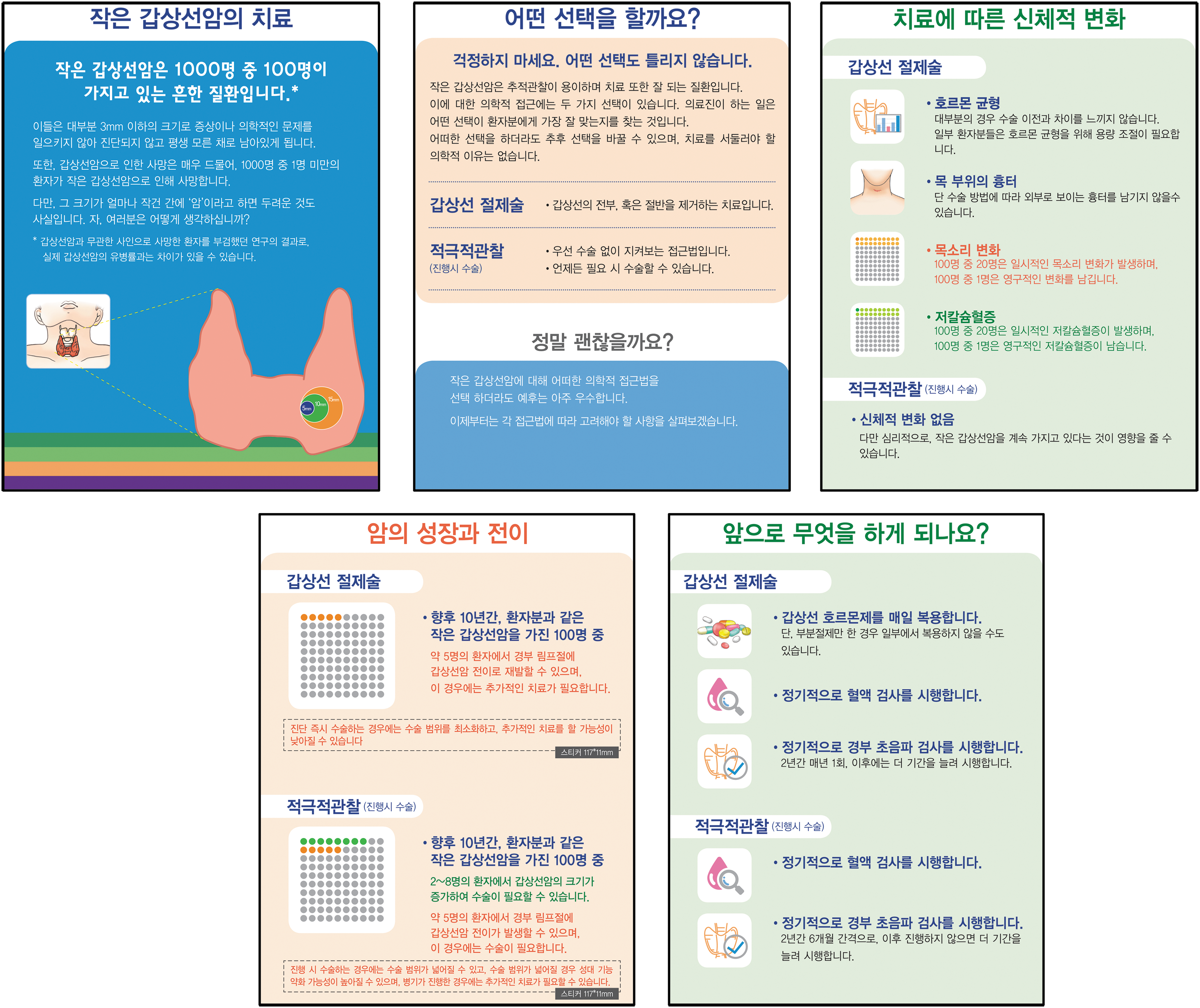
Screen shots of representative cards of Thyroid Cancer Treatment Choice Korean version.
Detailed patient eligibility criteria are described in the Supplementary Data (Supplementary Data are available online at
Statistical analysis
Patient characteristics were described by frequencies and percent for categorical variables and by means and standard deviations for continuous variables. Differences in estimates between two groups were evaluated using either the chi-square test (linear by linear test) or Fisher's exact test for categorical variables and Student's t-test or Wilcoxon rank sum for continuous variables, as appropriate. All p-values presented are two-sided.
Results
Between May 2016 and April 2017, 278 patients were included in the study, 220 (79%) of whom were female. Of these, 152 (53%) were seen in the conversation aid clinic. Age, sex, and mean (±SD) tumor size (6.6 ± 1.6 mm and 6.5 ± 1.9 mm) distributions were similar across clinics. Overall, 233 (84%) patients opted for active surveillance and 53 (16%) for thyroid surgery (Table 2). Patients in the conversation aid group were more likely to choose active surveillance than the patients seen in the usual care clinic (88.9% vs. 77.0%, respectively; (relative risk = 1.16 [confidence interval 1.04–1.29]). Patients who chose active surveillance supported by the conversation aid had more thyroid cancer nodules measuring >5 mm than usual care patients who chose active surveillance (81% vs. 67%; p = 0.013; Table 3). Five patients who initially opted for active surveillance in a usual care clinic changed their decision for thyroid surgery during follow-up.
Derived by Fisher's exact test.
Derived by Student's t-test.
Derived by linear-by-linear test.
Of 97 patients, five changed their decision for thyroid surgery during follow-up.
M, male; F, female; AS, active surveillance; OP, operation/surgery.
Derived by Fisher's exact test.
Derived by linear-by-linear test.
Discussion
The Thyroid Cancer Treatment Choice decision aid was developed for patients facing treatment decisions related to PMCs. This tool attempts to convey the best available evidence about the management options, as well as the aspects of those alternatives that matter to patients. This tool, developed by means of user-centered design principles, promotes conversations between clinicians and patients about both active surveillance and surgery as available management options. The pilot testing of the tool demonstrated that its use is associated with increased acceptance of active surveillance.
The most likely explanation for the increased acceptance of active surveillance is its underuse at baseline. Some but not all studies have shown that patient decision aids promote the uptake of less invasive treatments (31). The tool was designed to be a balanced presentation of options and was not intended to nudge toward a specific management. A formal clinical trial is now necessary to determine the extent of its impact on shared decision making, but also, through careful examination of the difference between the conversations it promotes and those emerging in usual care, of how patients come to realize which treatment makes intellectual, emotional, and practical sense to them. It is possible that clinician behaviors and patient population, independent from the use of the tool, may have contributed to management decisions. A future trial that includes randomization of a larger number of clinicians should address these limitations.
Thyroid Cancer Treatment Choice was designed to facilitate conversations about management options for subcentimeter papillary thyroid carcinomas, and in doing so, this tool supports the implementation of active surveillance as a treatment option, as suggested by the 2015 American Thyroid Association guidelines (23). These guidelines also released a recommendation against fine-needle aspiration biopsy of tumors <1 cm, noting that for high-risk sonographic subcentimeter nodules, that is, high suspicions pattern in the absence of extrathyroidal extension, metastatic cervical lymph nodes, or distant metastases, “close sonographic follow-up” or immediate biopsy are an option, depending on patient age and preferences. Thyroid Cancer Treatment Choice could be further developed to support this recommendation and to help clinicians assess which approach (active surveillance or biopsy) best fits the patient context and needs.
Thyroid Cancer Treatment Choice, tested as a paper tool, has since been developed as an electronic tool. This enables individualization of risk of cancer and of cancer progression based on age, and facilitates its implementation into electronic health records. The new version of this tool has also incorporated the option of ultrasound-guided percutaneous ethanol ablation for institutions that offer this treatment option. Given that the original tool was validated in the South Korean context only, this tool is currently being testing in two healthcare systems in the United States with the goal of understanding how the tool supports shared decision making and affects treatment decisions.
Conclusion
Thyroid Cancer Treatment Choice is an evidence-based tool that supports the presentation of treatment options for PMCs. Pilot testing suggests that this conversation tool increases acceptance of active surveillance, implying that this option is an acceptable and preferable alternative for informed patients. Further studies are warranted to confirm this finding to include testing in countries with varying cultures.
Footnotes
Acknowledgments
Juan P. Brito is supported by the Karl-Erivan Haub Family Career Development Award in Cancer Research at Mayo Clinic in Rochester, honoring Richard F. Emslander, MD.
Author Disclosure Statement
The authors have no disclosures.