
Abstract
Background:
Little is known about annual hazard rates of cancer mortality and recurrence for papillary thyroid cancer (PTC). This study investigated the time-varying pattern of cancer death and recurrence from PTC and independent prognostic factors for cause-specific mortality (CSM) and recurrence of PTC.
Methods:
This retrospective chart review enrolled 466 patients diagnosed with PTC who underwent curative initial surgery between April 1981 and December 1991 with a median follow-up of 18.4 years. Clinical characteristics, cancer mortality (primary endpoint), and recurrence (secondary endpoint) were ascertained. The failure rates of either death or recurrence were estimated using the Kaplan–Meier methods, and annual death/recurrence hazard was depicted using hazard function.
Results:
In this Japanese cohort where only 1.5% of patients received radioactive iodine therapy, the 10-, 20-, and 30-year CSM rates were 2.7%, 6.2%, and 8.6%, respectively. Eleven (44.0%) cases of death occurred within the first 10 years, whereas 10 (40.0%) and 4 (16.0%) cases occurred within 10–20 and 20–30 years after surgery, respectively. The 10-, 20-, and 30-year recurrence rates were 11.3%, 21.8%, and 29.4%, respectively. Forty-six (54.8%) cases of recurrence occurred within the first 10 years, predominantly within the first five years (31 cases; 36.9%), whereas 29 (34.5%), 7 (8.3%), and 2 (2.4%) cases occurred within 10–20, 20–30, and ≥30 years after surgery, respectively. Age ≥55 years was the only independent prognostic factor for CSM. Age ≥55 years, male, tumor size > 4 cm, extranodal extension, and positive pathological lymph node metastasis were independent prognostic factors for recurrence. The annual hazard curve of cancer mortality presented a double-peaked distribution, with a first peak at the 10th year, and the second peak reaching the maximum at the 20th year after surgery for the entire population. The annual hazard curve of recurrence showed a triple-peaked pattern, with surges at about 12, 22, and 29 years after surgery.
Conclusions:
Patients with PTC harboring at least one of the prognostic characteristics may be at persistent risk of cancer mortality and recurrence even 10 or more years after initial treatment. Understanding the hazard rate of PTC is key to creating more tailored treatment and surveillance.
Introduction
Incidence rates of thyroid cancer, especially papillary thyroid cancer (PTC), have been continuously rising worldwide over the last few decades, while mortality rates have remained fairly stable (1 –3). Generally, PTC is an indolent disease, rarely behaving as an aggressive tumor, with an excellent prognosis, as evidenced by the extremely low 30-year disease-specific mortality rate (<10%). However, it may recur several years after initial treatment (4,5). Most recurrences are not fatal, but they can bring great stress and burden for patients. Therefore, in contrast to most other malignancies, more attention has been directed toward recurrence rates rather than cancer deaths as the focus and endpoint of PTC (6). In fact, both death and recurrence from PTC can occur >30 years after initial diagnosis, raising important questions for treatment and follow-up of PTC patients (5). Risk of death or recurrence is generally described by survival curves as outcomes for cancer patients, while their hazard functions have rarely been reported. Survival curves focus on the cumulative time distribution of survival or recurrence-free rate, that is, the percentage of patients who remain survival or recurrence-free at a given time after initial treatment. The hazard function depicts the rate of failure (death or recurrence) at any instant among the remaining “at risk” individuals. It describes not only the magnitude of the failure rate, but also how it changes over time. It has been applied to provide insights into the patterns of death or recurrence of various malignant tumors including breast cancer, gastric cancer, and early-stage (T1a-T2bN0M0) non–small cell lung cancer (NSCLC) (7 –10). However, changes in hazards of the oncologic events for thyroid cancer have never been reported. The present study examined the time-varying pattern of death and recurrence of PTC, along with risk factors associated with the failures.
Methods
Patients
A total of 466 patients with PTC who underwent curative (i.e., macroscopically no residual disease) initial surgery between April 1981 and December 1991 in the Department of Endocrine Surgery at Tokyo Women's Medical University were eligible for inclusion in this study. Patients with one or more of the following conditions were excluded: non-PTC types (follicular/medullary/anaplastic/poorly differentiated), age ≤18 years, a history of previous thyroidectomy, presence of distant metastasis at the time of diagnosis, or never free of disease. Extrathyroidal extension was defined as follows: ExT0, no extension; ExT1 (also called minimal extrathyroidal extension), extension to the sternothyroid muscle or perithyroid soft tissues; ExT2 (also called maximal extrathyroidal extension), extension to subcutaneous soft tissues, larynx, trachea, esophagus, recurrent laryngeal nerve, or prevertebral fascia encasing the carotid artery or mediastinal vessels. Extranodal extension was defined as follows: ExN0, no extension; ExN1, extension to strap muscle, recurrent laryngeal nerve, trachea, or jugular vein. The grading of extrathyroidal or extranodal extension was based on intraoperative surgical findings as well as pathological findings. Patients were categorized in three prognostic subgroups: low-risk (T1N0M0 in TNM classification), intermediate-risk, and high-risk patients (T > 5 cm, extrathyroidal extension to the mucosa of the trachea or esophagus, clinically palpable lymph node metastases, or the presence of distant metastasis). For this study, thyroidectomies were dichotomized into two groups: total thyroidectomy and less than total thyroidectomy (including subtotal, partial, enucleation, and Dunhill). After surgery, high-risk patients took levothyroxine for thyrotropin (TSH) suppression, and low-intermediate risk patients took levothyroxine for substitutive therapy if necessary. At that time, the extent of operation for PTC was conservative, and availability of radioiodine treatment was quite limited. As a result, only seven patients were treated with radioiodine therapy. All patients were regularly followed every 6–12 months by both physical exams and thyroid function tests, including serum thyroglobulin, in conjunction with neck ultrasonography (US) and computed tomography (CT) to identify cancer recurrence if necessary. Median follow-up was 18.4 years (range 0.02–35.96 years). This retrospective study was approved by the Ethical Committee of Tokyo Women's Medical University (no. 4445), and the requirement to obtain informed consent was waived.
Statistical analysis
Recurrence was defined as newly detected tumor or metastatic lymph node revealed by US and/or imaging scans in any patient who had been free of disease, which was confirmed by fine-needle aspiration biopsy and/or histopathology. Recurrence was classified as follows: “local” if only the thyroid bed or residual thyroid gland tissue was involved; “regional” if lymph nodes of central or lateral compartments of the neck were involved; “distant” if disease was located in other sites, including the lungs, liver, bones, and brain. The failure rates of either cancer deaths or recurrence were estimated using the Kaplan–Meier method as the day of surgery being time zero and compared using the log-rank test. Cox proportional hazards regression modeling was used for multivariate analysis to determine independent prognostic factors for death and recurrence. Annual hazard rates were estimated using a kernel smoothing method (8,9,11). Hazard ratios (HRs) are presented with their confidence intervals (CIs). All statistical analyses were performed using Stata v9.0 (StataCorp Ltd., College Station, TX). All statistical tests were two sided, and differences were considered statistically significant if p < 0.05.
Results
A total of 466 patients were included in the analysis. General characteristics of the study population are summarized in Table 1. To date, 25 (5.4%) patients in the study have died of PTC. Contemporary deaths from PTC were related to distant disease in 20 (80.0%) cases (lung metastasis in 19 cases and thoracic vertebra metastasis in one case), regional recurrence in four (16.0%) cases, and postoperative tracheoesophageal stenosis in one (4.0%) case. Recurrence has been identified in 84 (18.0%) patients. Initial recurrence in the majority of cases (n = 57; 67.9%) was regional; among them, concurrent local and distant metastasis occurred in four cases and one case, respectively. Distant metastasis was identified in 16 (19.0%) cases, including to the lungs (14 cases; 87.5%), the liver (1 case; 6.3%), and both the lungs and the liver (1 case; 6.3%). Local recurrence occurred in 17 (3.6%) cases, including in the operated thyroid bed (10 cases; 58.8%) and in contralateral residual thyroid tissue (7 cases; 41.2%), respectively. The mean time to cancer mortality and initial recurrence were 13.50 ± 5.53 years and 9.41 ± 7.69 years (specifically, 10.60 ± 7.80 years for local, 7.86 ± 7.71 years for regional, and 13.49 ± 5.62 years for distant recurrence), respectively. The distributions of oncological events according to the time from surgery were further analyzed. There was a significant difference of recurrence type between the first, second, and third decade, with the percentage of distant metastasis being 6.5%, 34.5%, and 42.9%, respectively (p < 0.01). Fewer patients died from distant metastases in the first decade than in the second decade, although the difference was not statistically significant (72.7% vs. 90.0%; p > 0.05). The 10-, 20-, and 30-year cause-specific mortality (CSM) rates were 2.7 ± 0.8%, 6.2 ± 1.3%, and 8.6 ± 1.8%, respectively. The 10-, 20-, and 30-year recurrence rates were 11.4 ± 1.6%, 21.9 ± 2.4%, and 29.5 ± 3.5%, respectively. There were statistically significant differences in the estimated mortality and recurrence rates between the three risk groups (p < 0.001; Fig. 1).
Summary of Patient Characteristics
ExT0, no extension; ExT1, extension to the sternothyroid muscle or perithyroid soft tissues; ExT2, extension to subcutaneous soft tissues, larynx, trachea, esophagus, recurrent laryngeal nerve, or prevertebral fascia encasing the carotid artery or mediastinal vessels; ExN0, no extension; ExN1, extension to strap muscle, recurrent laryngeal nerve, trachea, or jugular vein; PLNM, pathological lymph node metastasis; RAI, radioactive iodine therapy.
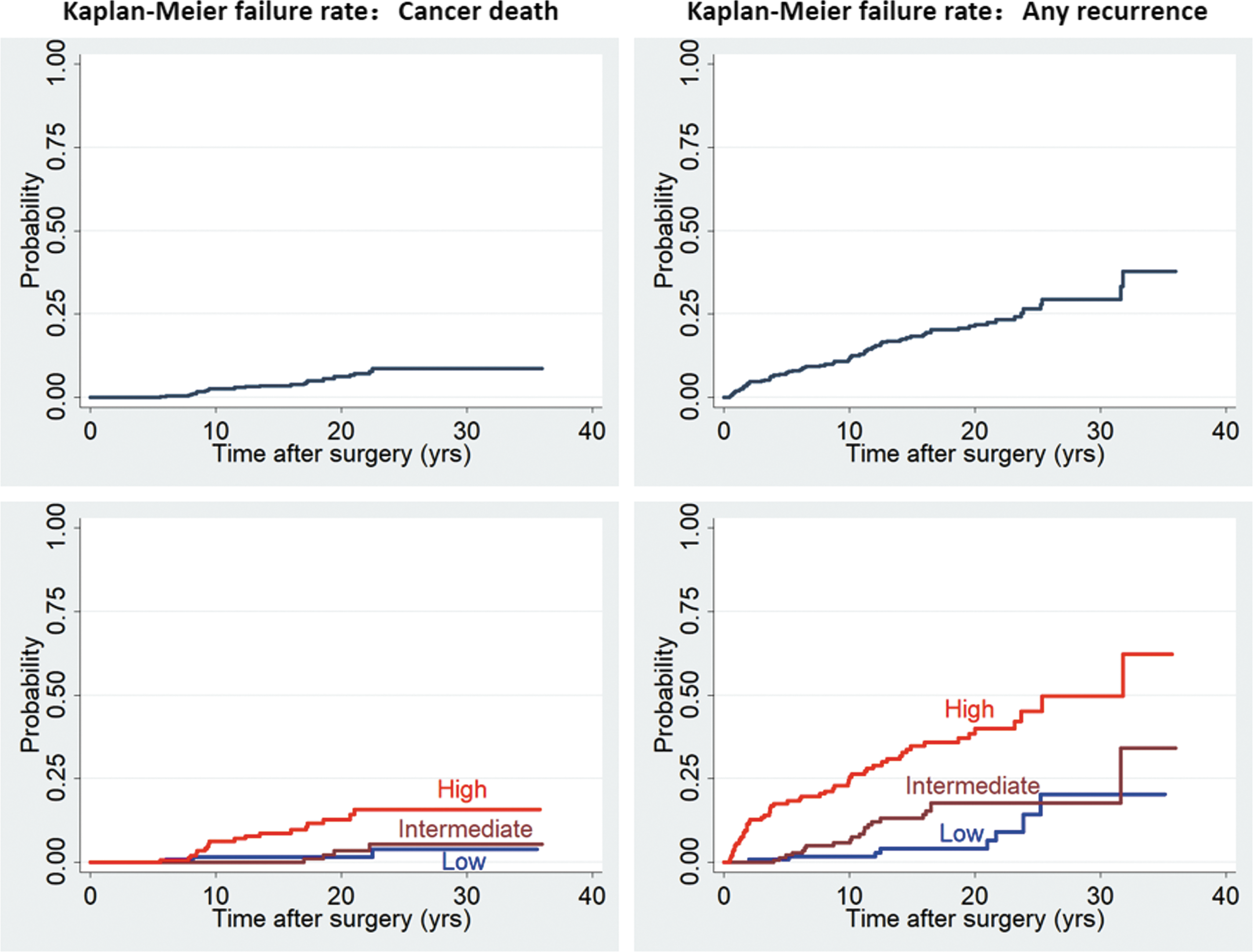
The rate of failure (cancer death or any recurrence) for the entire cohort and different risk classes.
Prognostic factors
Survival analyses stratified by patients' clinicopathologic characteristics showed that age ≥55 years at surgery, male, tumor size >4 cm, extrathyroidal extension, and pathological lymph node metastasis (PLNM) were associated with cancer death (Table 2). A Cox proportional hazards regression model incorporating these variables revealed that age ≥55 years at surgery was the only significant predictor for CSM (Table 2). Factors associated with cancer recurrence included age ≥55 years at surgery, male, tumor size >4 cm, extrathyroidal extension, extranodal extension, and PLNM in the univariate survival analyses (Table 3). All of these were also significant prognostic factors for cancer recurrence in the multivariate survival analysis except extrathyroidal extension (Table 3).
Survival Analysis of Cause-Specific Mortality in 466 Patients with Papillary Thyroid Cancer
p < 0.05.
LT, less than total thyroidectomy; TT, total thyroidectomy; HR, hazard ratio; CI, confidence interval.
Survival Analysis of Cancer Recurrence in 466 Patients with Papillary Thyroid Cancer
p < 0.05.
Death hazard analysis
The annual hazard curve of cancer mortality showed a double-peaked distribution, with a first minor peak at the 10th year, followed by a nadir at the 14th year, and then a rapid rise reaching the major peak at the 20th year after surgery for the entire population (Fig. 2). The death hazard curves formed double- and single-peaked patterns for high- and intermediate-risk patients, respectively, but a relatively flat convex curve without significant surges for low-risk patients. The death hazard rate of high-risk patients was sustained and higher than that of intermediate- or low-risk patients (Fig. 2).
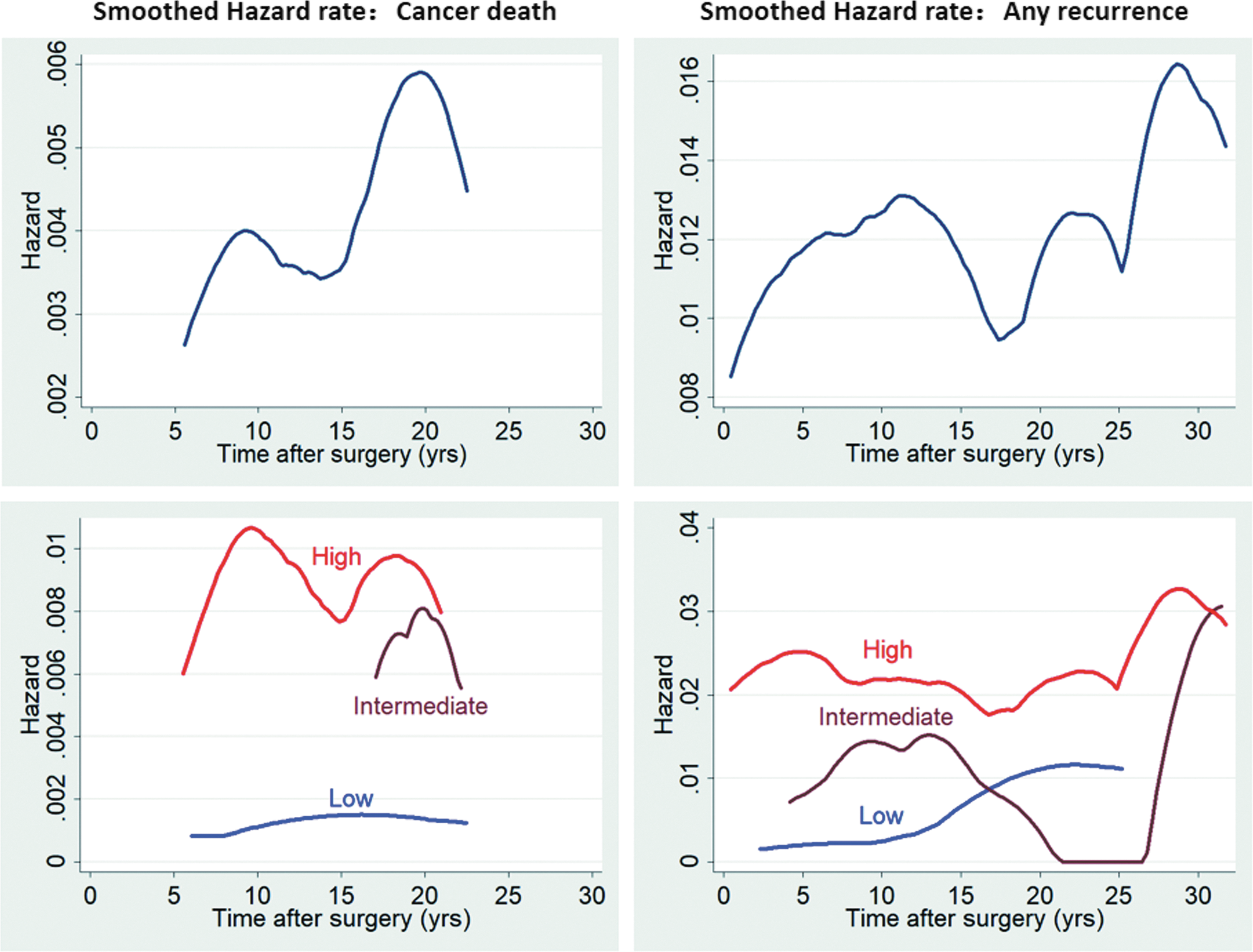
Annual hazard rate of cancer death or any recurrence for the entire cohort and different risk classes.
Recurrence hazard analysis
The annual hazard curve of recurrence for the entire population showed a triple-peaked pattern, with surges at about 12, 22, and 29 years after surgery (Fig. 2). The curves exhibited a triple-, double-, and single-peaked distribution for high-, intermediate-, and low-risk patients, respectively. Likewise, the recurrence peak for high-risk patients emerged earliest, followed by intermediate-risk patients, and was latest for low-risk patients. Therefore, low-risk PTC were less likely to recur early compared to intermediate- and high-risk PTC (Fig. 2).
Discussion
Prognosis and prognostic factors
Patients with PTC show an excellent long-term prognosis after optimized treatment, although it is inevitable that some patients experience adverse oncologic events. The present study demonstrates the validity of the risk-grouping definitions, since they reflect clearly separated clinical courses, that is, high-risk patients do carry a higher risk of cancer mortality and recurrence compared with the low- or intermediate-risk patients. PTC patients have relatively low disease-specific mortality rates even at 20 or 30 years after initial treatment, as demonstrated by previous studies (12). On the other hand, tumor relapse rates are relatively high (4,5,12,13). In fact, nearly one fifth (18.0%) of patients suffered from a relapse in this study cohort. Therefore, much attention has been paid to recurrences, especially regional lymph node metastasis. Patients with recurrent disease are candidates for revision surgery. Yet, the relevant guidelines recommend that some variables should be considered comprehensively to decide whether to operate in this situation (14 –16).
Various factors involved in the outcomes of patients with PTC have been explored, such as age, sex, tumor size, multifocality, extrathyroidal extension, and PLNM. Age has been considered as a powerful independent prognostic factor associated with cancer mortality in PTC (17 –24). The latest edition of the Union for International Cancer Control/American Joint Committee on Cancer (AJCC) staging system (eighth edition) changed the cutoff age for patients with differentiated thyroid cancer from 45 to 55 years (25). Some studies indicated that the cutoff age was also prognostic with regard to recurrence of DTC, although others refuted the association (26,27). The prognostic significance of sex has been controversial. Male sex has been reported to be associated with cause-specific survival and disease-free survival (28) or recurrence (29). A meta-analysis further strengthened the evidence that male sex was significantly correlated with recurrence (27). However, other researchers found that it was not associated with the risk of death or recurrence (5,30). The prognostic significance of large tumor size has been widely recognized, although its cutoff value has been different among various staging systems (e.g., AJCC and AMES) or survival analysis studies. Matsuzu et al. found that tumor size > 4 cm was one of the risk factors of cancer mortality (31). Ito et al. also demonstrated that tumor size > 2 cm was an independent prognostic factor for lymph node and lung recurrences, while tumor size > 4 cm can independently predict bone recurrence and affect both cause-specific survival and disease-free survival of PTC patients (24,32). As for the multifocality of PTC, findings about its prognostic impact have been published in several previous studies (4,33,34). Consistent with the data in the present study, Grogan et al. found that tumor multifocality had no significant relationships with cancer mortality or recurrence (5). The European Society of Endocrine Surgeons recommends that more extensive therapy should be considered for multifocal PTC, even though the authors acknowledge the controversial prognostic significance of multifocality (35). Extrathyroidal extension is recognized as a significant prognostic factor for PTC, but some controversy exists regarding the differential importance of ExT1 and ExT2 (36,37). While ExT2 has been found to be associated with CSM and recurrence (24,36,37), the prognostic value of ExT1 remains controversial (36 –39). As for extranodal extension, two meta-analyses indicated that it is associated with a significantly increased risk of death and recurrence (40,41). The prognostic significance of PLNM continues to evolve. It has been reported that PLNM is significantly correlated with disease recurrence but not cancer mortality (5,27,30).
Hazards of failures
The unique observation in the present study is that high-risk patients carried higher, sustained hazard rates of both cancer mortality and recurrence compared to low- and intermediate-risk patients. The hazard functions for cancer death and recurrence from PTC showed a double- and triple-peaked pattern, respectively. The patterns with multiple peaks are similar to those of other malignancies. Yet, they are quite different in terms of timing and magnitude (7 –10). The peak of cancer mortality in PTC occurs later and is smaller compared to that in breast cancer. The hazard of recurrence also reaches its first and second peak significantly later compared to breast cancer, early-stage NSCLC, or gastric cancer (8 –10). The origin of the multiple-peak hazard curves has not yet been established, although Demicheli et al. proposed the tumor dormancy hypothesis where the growth of micrometastatic or residual foci in various biological steady states could occur differently and suddenly, rather than uniformly, and may be continuously triggered by several biological mechanisms (42,43).
Study limitations and future suggestions
The present study has several potential threats to validity both internally and externally in estimating hazards of failures because of the retrospective nature of the observations. First, some patients were lost to follow-up. Patients should have been followed for at least 25 years because they underwent initial treatments before December 1991, but the shortest observation time was 0.02 years. The failure rates observed in this study might be underestimated because patients who dropped out but experienced failures at a later time point would not be counted. Second, diagnostic tests for postoperative surveillance were not carried out uniformly. Although physical examinations and thyroid function tests (including thyroglobulin) were routinely performed at each visit, other tests such as US or CT were used at the discretion of attending physicians. Since low-risk patients are less likely to undergo detailed examinations, some recurrent lesions might have been missed during the follow-up. Third, because of the relatively small number of patients, particularly those at risk in the later time period, the reproducibility of survival rates and hazard rates might be questionable in this subgroup. Although confidence intervals for the Kaplan–Meier estimates are readily available, reproducibility of corresponding estimates might be unstable. Fourth, the initial management of PTC in the present study was somewhat different from that in current practice worldwide in terms of the extent of surgery, use of radioactive iodine, and TSH suppression. Therefore, the findings may not be directly applicable to patients outside the study.
A prospective study with long-term observations is essential to obtain valid estimates for time distribution of cancer mortality and recurrence risk of PTC, which is largely an indolent tumor. With such information available, individual treatment and surveillance recommendations will be able to be formulated more easily.
Footnotes
Acknowledgments
This article is dedicated to Drs. Yoshihide Fujimoto, Takao Obara, and Yukio Ito who cared for patients and taught us their humane clinical practice at Tokyo Women's Medical University. This study was supported in part by Japan China Sasakawa Medical Fellowship.
Author Disclosure Statement
No competing financial interests exist.