
Abstract
Background:
The natural course of persistent/recurrent differentiated thyroid cancer (DTC) has not been fully elucidated. The purpose of this study was to assess the relative incidence and clinico-radiological characteristics of persistent disease and clinical recurrence based on computed tomography (CT) analysis in patients with persistent/recurrent DTC.
Methods:
From January 2005 to December 2016, this retrospective study included 107 patients (M:F = 28:79; M age = 53.5 years) with surgically proven cervical locoregional recurrence of DTC. Two neck CT examinations (median interval 1.92 years; range 0.17–7.58 years) before the last thyroid cancer surgery within the study period were reevaluated. Based on the presence of the lesion on the first CT and its progression on the second CT, the locoregional recurrence was classified into the following categories: stable persistence (decrease, no change, or increase by <2 mm in short dimension on the second CT), progressive persistence (increase by ≥2 mm), and clinical recurrence (newly appeared on the second CT). Clinical and radiological characteristics of the three groups were compared using univariate and multivariate logistic regression analyses.
Results:
The relative incidences of stable persistence, progressive persistence, and clinical recurrence were 56.1% (60/107), 15.0% (16/107), and 29.0% (31/107), respectively. Multivariate analysis between the clinical recurrence (29.0%) and persistence (71.0%) groups revealed various independent factors for prediction of clinical recurrence. These included longer interval between the two CT examinations (median 2.67 vs. 1.79 years; p = 0.021), a smaller number of thyroid surgeries (1.16 ± 0.45 vs. 1.55 ± 0.81; p = 0.002), and a history of neck dissection at the location of the largest locoregional recurrence (70.0% vs. 31.4%; p < 0.001). There was no significant independent factor for differentiation between the stable persistence (78.9%; 60/76) and progressive persistence (21.1%; 16/76) groups. The results may have been influenced by selection bias because this study included only surgically proven cases.
Conclusions:
With regard to cervical locoregional recurrence of DTC, active surveillance may be favored because more than a half of the cases are structurally persistent and stable. However, meticulous evaluation is necessary to detect progressive persistence and clinical recurrence, considering various clinical factors.
Introduction
A
Traditionally, locoregional recurrence found after thyroid cancer surgery has been described as persistent/recurrent DTC because it may not be easy to differentiate between persistent disease and true recurrence, with many cases tending to be persistent (1,3,9,12). This persistent tendency of locoregional recurrence may provide an important rationale for active surveillance, along with the reported stable tendency of sonographically detected lesions during follow-up after thyroid cancer surgery (13 –15). However, until now, the natural course of surgically proven persistent/recurrent DTC has not been fully elucidated. Therefore, this study aimed to assess the relative incidence and clinico-radiological characteristics of persistent disease and clinical recurrence in patients with surgically proven locoregional recurrence of DTC.
Methods
Subjects
This study was approved by the Institutional Review Board of Seoul National University Hospital, and the requirement for informed consent was waived. Thyroid cancer patients who underwent reoperation between January 2005 and December 2016 were retrospectively reviewed, and 216 patients who were surgically diagnosed with locoregional recurrence of DTC, either lymph node (LN) recurrence or primary thyroid cancer recurrence in the thyroidectomy bed, were identified. One hundred nine patients were excluded from the study for the following reasons: absence of at least two neck computed tomography (CT) examinations before the last thyroid cancer surgery within the study period (n = 69), incomplete surgical record or pathologic report (n = 33), and less than total thyroidectomy as initial surgery (n = 7). Consequently, a total of 107 patients (79 women; age at the time of diagnosis of recurrence: 48.59 ± 14.79 years; 106 papillary thyroid cancers and one follicular thyroid cancer; total number of thyroid cancer operations 2.44 ± 0.74, range 2–5) were enrolled in this study. With regard to the two neck CT examinations, the second CT examination refers to the CT scan performed as a preoperative workup prior to the last thyroid cancer surgery. The first CT examination refers to the CT scan performed during preoperative workup (n = 85) or follow-up (n = 22) of the prior thyroid cancer surgery (initial thyroid cancer surgery [n = 73] or reoperation for locoregional recurrence [n = 34]) performed before the last surgery. The patients' demographic and clinical data, including sex, age, time intervals, treatment history, pathologic findings on initial surgery, and serologic results (e.g., serum thyroglobulin [Tg] level and thyroglobulin antibody (TgAb) level) before reoperation, were collected.
Surgical confirmation of locoregional recurrence
Recurrent/persistent DTC analyzed was surgically confirmed by reoperation as follows. All patients had central, lateral, or central and lateral neck dissection for the removal of recurrent/persistent DTC after assessment of the original tumor location, extent of prior neck dissection, and preoperative images. Compartment-oriented dissections were performed, except in nodal compartments that had been previously dissected. If the repeat compartment dissection could be risky or difficult, a more targeted neck dissection was performed in the area of recurrence.
CT protocol
In the authors' hospital, neck CT has been selectively performed as a preoperative workup or follow-up protocol as an adjunct to ultrasonography (US) in patients with DTC or locoregional recurrence of DTC. Neck CT scans were acquired using multidetector CT scanners (16–256 channels). Unenhanced CT scans were performed in some cases for the detection of calcifications. Subsequently, contrast-enhanced CT scans were performed in the cephalocaudal direction, from the skull base to the aorto-pulmonary window, 45 s after injecting a 90 mL bolus of iodinated nonionic contrast material (300–350 mg I/mL) intravenously into the right arm followed by injection of 20–30 mL of normal saline for flushing at 3 mL/s using an automated injector to avoid artifacts induced by stagnated contrast agents within the subclavian or innominate vein. With 0.625–1.25 mm collimation and a pitch of 0.9–1.3, all CT images were obtained in the axial plane and partly reconstructed into coronal images at every 2.5–3 mm on a 512 × 512 matrix.
CT evaluation and definition of persistent or recurrent disease
All clinical and radiologic data were independently reevaluated by two radiologists (J.H.K. and R.E.Y.; 17 and 7 years of experience, respectively, in head and neck radiology). Any discrepancy was resolved through consensus by the two radiologists.
Referring to US images obtained prior to the last thyroid cancer surgery, as well as surgical and pathologic records of the last surgery, first pathologically confirmed locoregional recurrence of DTC identified on the second CT examination was identified on the basis of known CT features of LN metastasis, including cystic change, calcification, heterogeneous enhancement, and strong enhancement (10). After meticulous review of the images from the first CT scan, surgical and pathologic records of the prior thyroid cancer surgery before the last surgery, the locoregional recurrence was categorized as persistent when it could also be identified on the first CT examination. The presence of persistent disease on the first CT scan was determined by identifying them with similar or same features on the second CT at the same location. In comparison, the locoregional recurrence was categorized as clinical recurrence when it could not be identified on the first CT scan and had newly appeared on the second CT scan. At present, it may be impossible to differentiate between growth from microscopic tumors that were not detected by initial imaging and true recurrence. In cases of locoregional recurrence with multiplicity, they were categorized as persistent if each individual recurrence was classified as persistent without any clinical recurrence, and as clinical recurrence if there was at least one clinical recurrence among the multiple tumors. According to its progression on the second CT scan, persistence was subcategorized as either stable persistence (decrease, no change, or increase by <2 mm in short dimension on the second CT scan) or progressive persistence (increase in short dimension by ≥2 mm). The short dimension of 2 mm was selected as a reference to define tumor growth according to the recommendation for pulmonary nodules on CT by Bankier et al. (16). After measuring both short and long dimensions of locoregional recurrence of DTC in the axial plane as suggested by Bankier et al. (16), the short dimension rather than the long dimension was selected to determine interval size change in accordance with the guidelines of the American Thyroid Association (ATA) (9).
For evaluation of radiologic characteristics, the largest persistence in patients with persistence and the largest clinical recurrence in patients with clinical recurrence was analyzed. Qualitative radiologic characteristics such as the presence of calcification and cystic appearance were reviewed. For evaluation of the degree of enhancement, one radiologist (R.E.Y.) placed regions of interest (ROIs) on the solid area with the strongest enhancement within the locoregional recurrence and on the homogeneous area of the sternocleidomastoid muscle (SCM) to measure Hounsfield units (HU). The enhancement ratio of the locoregional recurrence relative to the SCM was calculated using the following equation: enhancement ratio = HUlocoregional recurrence of DTC/HUSCM.
Statistical analysis
Continuous and categorical variables were compared between the persistence and clinical recurrence groups and between the stable persistence and progressive persistence groups using an unpaired Student's t-test, Mann–Whitney U-test, Pearson's chi-square test, or Fisher's exact test as appropriate. Subsequently, binary logistic regression analyses with a forward stepwise method were performed. This was done to predict clinical recurrence or instability of persistent disease (stable persistence vs. progressive persistence) using their characteristics as input variables in univariate analysis, with a p-value of ≤0.05. To compare serologic quantitative variables before and after the last surgery, a paired t-test was performed. The biochemical remission status was defined as a serum Tg level of <1 ng/mL. Statistical analyses were performed using IBM SPSS Statistics for Windows v23.0.1 (IBM Corp., Armonk, NY). A p-value of ≤0.05 was considered statistically significant.
Results
Characteristics of subjects
The clinical and radiologic characteristics of the 107 patients are summarized in Tables 1 and 2, respectively. Locoregional recurrences of DTC were multiple in 66.4%, with 30.8% found in the central compartment alone, 43.9% in the lateral compartment alone, and 25.2% in both the central and lateral compartments. The largest locoregional recurrence occurred in the central compartment in 41.1% of cases and in the lateral compartment in 58.9% of cases, and developed at previous neck dissection sites in 43.0% of cases (64.1% [25/39] of central and 29.5% [18/61] of lateral compartment recurrences). During the median interval of 1.92 years (range 0.17–7.58 years) between the first and second CT scans, the relative incidences of stable persistence, unstable persistence, and clinical recurrence were 56.0%, 15.0%, and 29.0%, respectively (Figs. 1 –5). The absolute growth and growth rates in the short dimension during the interval between the two CT scans were 0.0001 ± 1.17 mm and 0.22 ± 2.07 mm/year, respectively, for stable persistence; 6.29 ± 3.15 mm and 5.05 ± 7.43 mm/year, respectively, for unstable persistence; and 9.02 ± 4.42 mm and 4.72 ± 3.79 mm/year, respectively, for clinical recurrence (Figs. 1 –5). Distant metastases were found in the lung in six patients. They were found during the postoperative surveillance in five patients and before initial surgery in the remaining patient with clinical recurrence. All of them were found prior to the first CT scans, and none of the cases developed new distant metastasis during follow-up.

Stable persistence with size decrease in a 52-year-old woman. The locoregional recurrence with strong enhancement in the pre-tracheal area (arrows) decreased in size from (
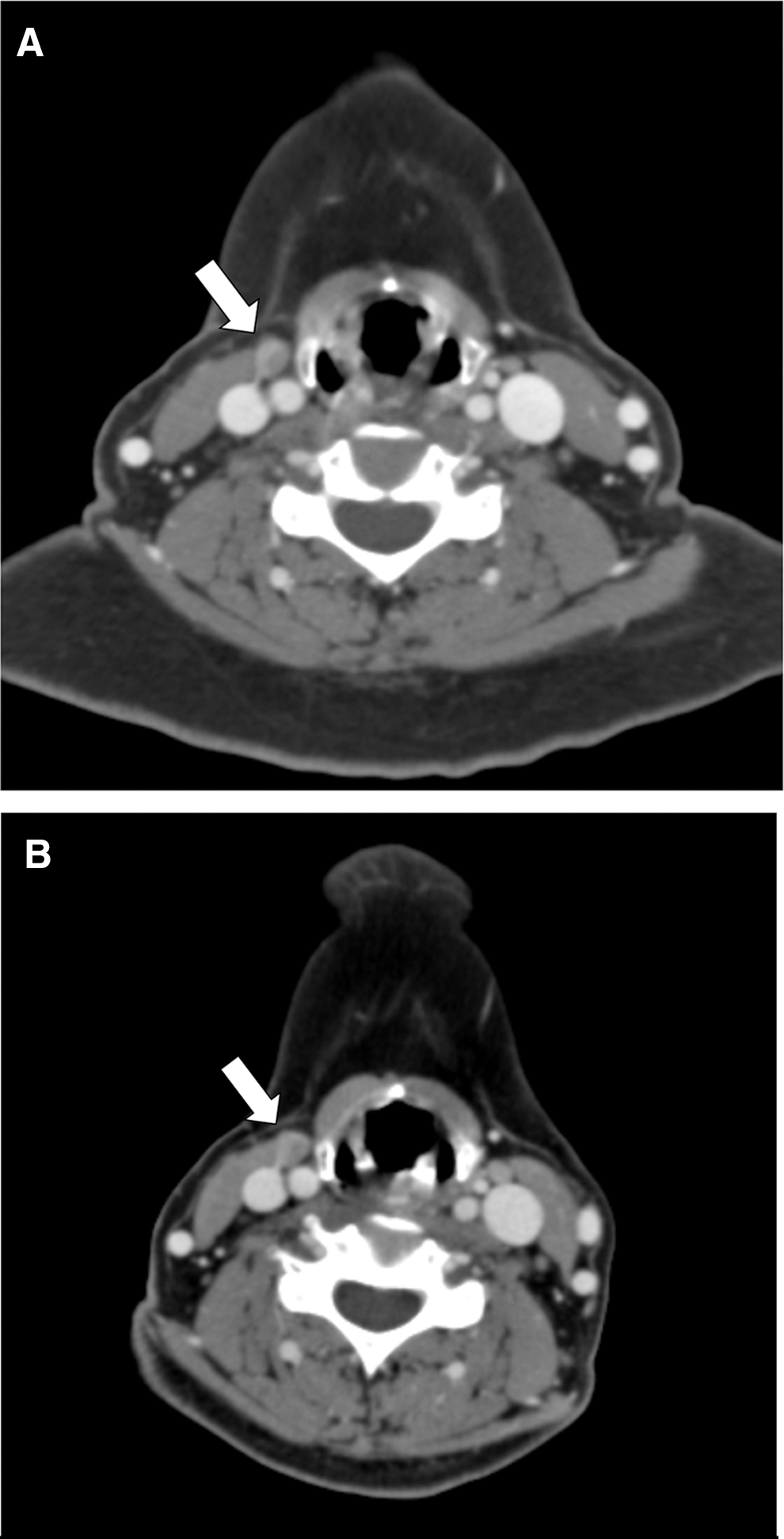
Stable persistence without size change in a 62-year-old woman. The 10.7 mm locoregional recurrence with heterogeneous enhancement (arrows) at right level III did not change between (
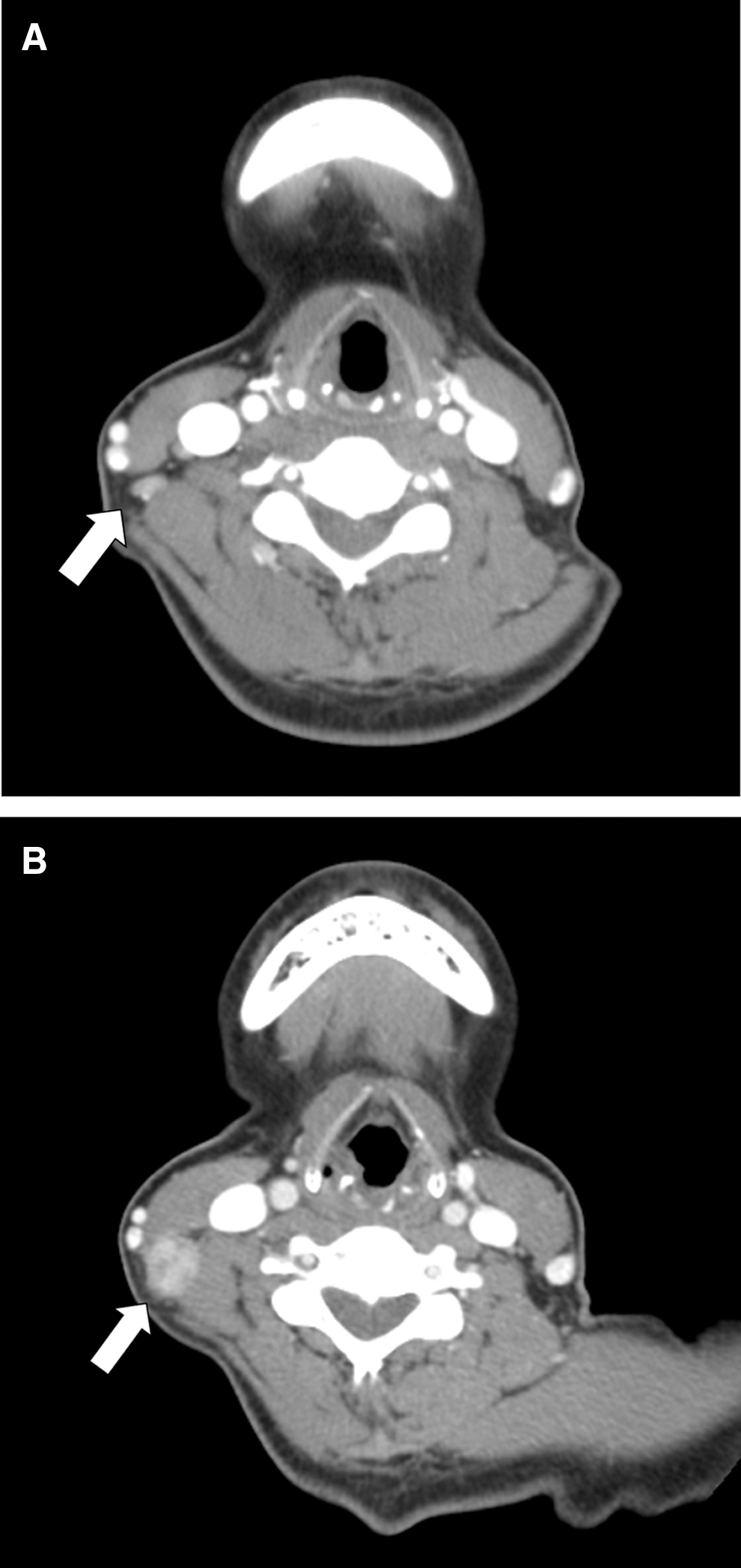
Progressive persistence in a 55-year-old woman. The LN metastasis with strong enhancement (arrows) at right level III increased in size from (
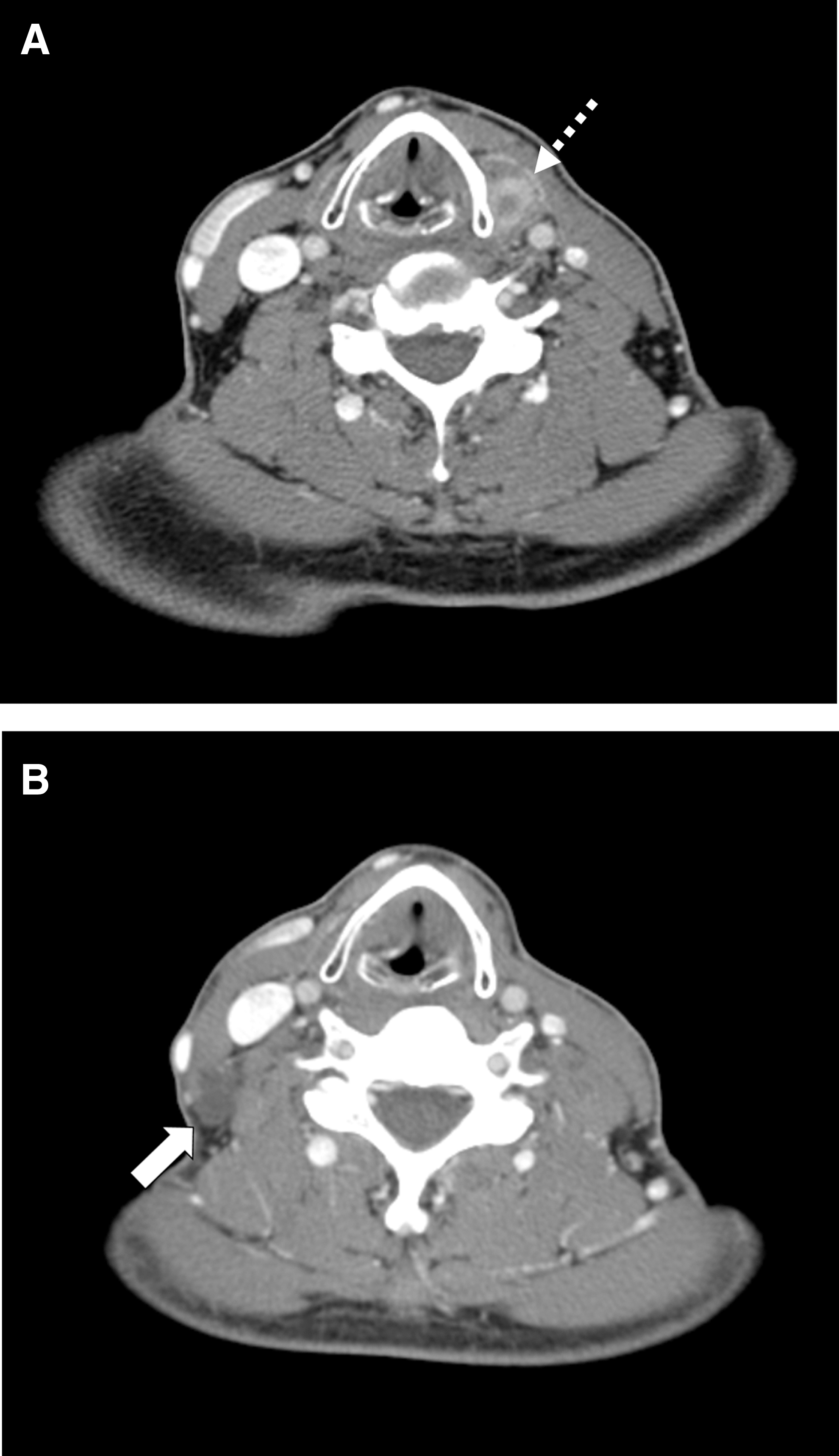
Clinical recurrence at non-dissection bed in a 54-year-old man. The locoregional recurrence with heterogeneous and strong enhancement (dashed arrow) at left level VI depicted on (

Clinical recurrence at the dissection bed in a 77-year-old woman. The multiple LN metastases with strong enhancement (dashed arrows) around the trachea depicted on (
Unless otherwise indicated, data are means ± standard deviation. Data in parentheses are raw data.
Data are medians. Data in parentheses are the interquartile range.
In 94 patients, tumor sizes at initial surgery could be analyzed.
Data were obtained at a mean of 1.55 months before the last operation.
Patients with TgAb level >100 IU/mL were excluded from the analysis.
DTC, differentiated thyroid carcinoma; CT, computed tomography; Tg, thyroglobulin; TgAb, thyroglobulin antibodies.
Unless otherwise indicated, data are means ± standard deviation. Data in parentheses are raw data.
Analyzed at the largest true recurrence on the second CT if there was any true recurrence or analyzed at the largest persistence if there was no true recurrence. Data were obtained at a mean of 1.55 months before reoperation.
In seven patients, history of neck dissection was unclear at location of the largest recurrent/persistent DTC detected on the second CT.
Comparison between persistence and clinical recurrence groups
Table 3 shows the results of univariate and multivariate analyses. In the univariate analysis, the clinical recurrence group (29.0%; 31/107) had a longer time interval between the two CT scans (median 2.67 years [interquartile range (IQR) 1.67–4.25] vs. 1.79 years [IQR 1.08–2.85 years]; p = 0.021), a smaller number of thyroid surgeries (1.16 ± 0.45 vs. 1.55 ± 0.81; p = 0.013), and a higher incidence of history of neck dissection at the location of the largest locoregional recurrence (70.0% vs. 31.4%; p < 0.001) compared to the persistence group (stable and progressive persistence 71.0%; 76/107). Multivariate analysis revealed that all the above-mentioned factors were independent factors for prediction of clinical recurrence, that is, a longer interval between the two CT scans (p = 0.017, odds ratio [OR] = 1.033 [confidence interval (CI) 1.01–1.06]), smaller number of thyroid surgeries (p = 0.002, OR = 5.399 [CI 1.81–16.08]), and a history of neck dissection at the location of the largest locoregional recurrence (p < 0.001, OR = 11.048 [CI 3.50–34.86]). None of the various qualitative and quantitative radiologic features were significant predictors of clinical recurrence.
OR, odds ratio; CI, confidence interval; N.A., not applicable.
Comparison between stable persistence and progressive persistence groups
In univariate analysis, the progressive persistence group (21.1%; 16/76) had a higher age at the time of initial surgery (58.50 ± 11.84 years vs. 44.27 ± 14.21 years; p < 0.001) and at the diagnosis of recurrence (65.31 ± 12.83 years vs. 49.33 ± 14.11 years; p < 0.001) compared to the stable persistence group (78.9%; 60/76). However, multivariate analysis revealed no significant difference in any factor between the two groups. None of the various qualitative and quantitative radiologic features were significant predictors of progressive persistence as well.
Biochemical response comparison after the reoperation
Table 4 shows the change in serum Tg levels after the last surgery. From the analysis of 71 patients who did not have serum TgAb levels >100 IU/mL and who underwent complete resection for locoregional recurrence noted on the second CT, there were significant decreases in postoperative serum Tg compared to preoperative serum Tg in all subgroups. However, there were no significant differences in the decrease in serum Tg levels and biochemical remission rates among the subgroups.
Data are means ± standard deviation. Data in parentheses are raw data.
Laboratory reports were obtained from 71 patients at a mean of 1.54 months before and a mean of 3.85 months after the last operation. Thirty-six patients were excluded; patients with TgAb level >100 IU/mL (21 patients), who did not perform serum Tg level test before or after the last operation within six months (11 patients), or who underwent incomplete resection of recurrent/persistent DTC at the last operation (six patients) were excluded.
p-Values in this row represent the results of a paired t-test between serum Tg levels before and after the last operation.
Discussion
This is the first study to describe the change in the size of surgically confirmed locoregional recurrence of DTC on serial neck CT scans and to stratify them according to their persistence and stability. Although Tomoda et al. presented the size change of recurrent LN metastasis proven by fine-needle aspiration (FNA) or Tg in the washout of the needle, the lesions were not surgically confirmed and were evaluated by US, which is often influenced by operator dependence and subjectivity (11). In contrast, the present study attempted to provide objective data for the size change of persistent/recurrent DTC based on consistent measurement using CT. The size criteria of 2 mm for determination of the instability of the lesion in accordance with the recommendation on chest CT may be a subject of debate, given that a different size threshold (i.e., 3 mm) was used to define the size increase on US in the study by Ito et al. (17). However, more objective and consistent measurements in the short dimension by CT may allow for the use of more strict criteria to define the size increase. In addition, in the present study, most patients (15/16) in the progressive persistence group showed size changes >3 mm, which suggested that even the size criteria of 3 mm might have produced similar results in this study.
This study clarified that >70% of cases were structurally persistent and 78.9% (60/76) of persistent cases were stable in patients with locoregional recurrence. This finding may support active surveillance for the management of patients with locoregional recurrence. These findings are consistent with those of a previous study by Lepoutre-Lussey et al., in which 87.8% (121/138) of cases of local recurrence were persistent (18). They are also in line with the results of studies by Tomoda et al., in which 20.5% (17/83) of FNA-proven LN metastases demonstrated an increase of ≥3 mm on US. The high percentage of structurally persistent disease in locoregional recurrence might in part be due to observer and ascertainment bias in imaging evaluation. This may be related to the different degrees of suspicion for recurrence or LN metastasis at the time of evaluation (i.e., prior to initial operation vs. reoperation), along with the recent widespread use of high-resolution US and recent advancements in US machines and US-guided FNA knowledge (19,20).
However, because no one can easily guarantee whether stable persistent disease during a short-term period will not show aggressive behavior such as distant metastasis at long-term follow-up, it is still controversial whether active surveillance with potential delayed surgery may be the best option compared to other options such as early surgery or other less invasive treatment such as radiofrequency ablation.
Through multivariate analyses, it was found that the various prior treatment histories were predictive factors for clinical recurrence. It is noteworthy that identification of the tumor at the dissection bed was one of independent predictors for clinical recurrence, which is in keeping with the finding that clinical recurrence occurred more frequently in dissection beds (70.0%; 21/30) rather than in non-dissection beds (30.0%; 9/30). In addition, this study revealed that a longer interval between the two CT scans was another independent factor for clinical recurrence. This result might imply that stable conditions during short-term follow-up could not easily guarantee continuous stability. The tumor growth rates in the progressive persistence and true recurrence groups were 5.05 ± 7.43 mm/year and 4.72 ± 3.79 mm/year, respectively, which were larger than those in the studies by Rondeau et al. and Robenstok et al. (13,14). The reason for these high growth rates in the present study compared to previous studies is unclear. However, the current results may have been influenced by selection bias because this study included only surgically proven cases, unlike other studies that also included nonsurgical cases without FNA diagnosis or with only FNA diagnosis, in addition to the differences between CT and US (11,13,14). Meanwhile, the lower number of thyroid surgeries in patients with clinical recurrences may in turn suggest that reoperation in patients with a higher number of past thyroid surgeries is more likely to be targeting persistent disease rather than clinical recurrence. Although it was not significant in multivariate analysis, older age at the time of initial surgery and reoperation were present in aggressive persistence in univariate analysis. These results might be in line with the previous results that patient age may be one of the important poor prognostic factors in patients with clinical papillary thyroid carcinoma (17,21), although they are contrary to those in a previous study where primary papillary thyroid microcarcinomas of older adults tended to be stable (22).
Apart from the intrinsic limitation of a retrospective study performed in a single center, there are several limitations to this study that need to be mentioned. First, this study had a relatively short follow-up period, and only patients who underwent reoperation and had pathologically confirmed locoregional recurrence were included. This might have led to an overestimation of both the growth rate and relative incidence of the structurally progressive group in the whole population of locoregional recurrences. Second, the persistence in this study did not always exclude the possibility of true recurrence in the cases in which the first CT was obtained after the initial surgery. However, it may be an inevitable pitfall for this study, and the results of this study properly reflect persistence. Third, with regard to biochemical remission, there was no difference between the stable persistence and aggressive persistence groups. This result may be attributed to the small sample size and incomplete serologic data. However, it may also suggest that there could have been many undetected microcarcinomas other than macroscopic tumors, which influenced serum Tg levels. Lastly, just as Tomoda et al. failed to find a predictive factor for the growth of FNA-proven LN metastases on US (11), this study also failed to find imaging features predictive of the growth of surgically proven recurrence on CT. A prospective multicenter study with a larger sample size is warranted to confirm the results.
In conclusion, with regard to locoregional recurrence of DTC, active surveillance may be favored because more than a half of the cases are structurally persistent and stable. However, more meticulous evaluation is necessary to detect progressive persistence and clinical recurrence, considering various clinical factors such as follow-up interval, number of thyroid surgeries, and a history of neck dissection.
Footnotes
Acknowledgments
This study was funded by the SNUH Research Fund (05-2015-0050).
Author Disclosure Statement
The authors of this manuscript declare no competing financial interests exist.