
Abstract
Background:
The necessity of iodine supplementation in lactating mothers residing in countries with sustained salt iodization programs for iodine sufficiency of breast-fed infants remains unclear. The aims of this study were to investigate the effect of iodine supplementation on iodine status and growth parameters of lactating mothers and breast-fed infants and to compare these data with that of formula-feeding mothers and their infants during the first year of infancy.
Methods:
In this multicenter, double-blinded, randomized clinical trial conducted in four healthcare centers in Tehran (Iran), healthy lactating mothers and their term newborns aged 3–5 days were randomly assigned to treatment groups: placebo, 150 μg/day iodine, or 300 μg/day iodine. They were followed up for 12 months. Formula-fed infants aged 30–45 days and their mothers were randomly selected from the same centers. The primary outcomes were maternal and infant urinary iodine concentrations (UICs), breast-milk iodine concentrations (BMICs), and infant growth parameters, measured at 1, 2, 4, 6, 9, and 12 months during routine health visits. The formula-fed group was assessed at 2, 4, 6, 9, and 12 months of age. Analysis was by per protocol principle using mixed-effects models.
Results:
Mother–newborn pairs (n = 180) in treatment groups and partially/exclusively formula-feeding mother–infant pairs (n = 60) participated between October 2014 and January 2016. Median baseline UICs in the treatment groups were 84 μg/L (interquartile range [IQR] 41–143 μg/L) in mothers and 208 μg/L (IQR 91–310 μg/L) in their infants. The values in the formula-fed group were 76 μg/L (IQR 40–144 μg/L) in mothers and 121 μg/L (IQR 66–243 μg/L) in infants. The 300 μg/day iodine group showed significantly higher UICs and BMICs than did the other treatment groups; infant UICs in the 150 μg/day iodine, placebo, and formula-fed groups were similar. Infants in all groups showed iodine sufficiency (median UIC ≥100 μg/L) throughout the study period. Anthropometric measurements were similar between the treatment and formula-fed groups over the study period, except at the last follow-up visit at 12 months.
Conclusion:
Supplementation of breast-feeding mothers with either 300 or 150 μg/day iodine improved their iodine status. However, the iodine status of infants in all groups studied indicated iodine sufficiency during the first year of infancy, demonstrating that in countries with effective salt iodization program, iodine supplementation for lactating mothers is unnecessary.
Introduction
B
Salt iodization is a safe, cost-effective, widely accepted, and sustainable strategy for the prevention and control of iodine deficiency (7). Countries with well established universal salt iodization programs report great success in eliminating iodine deficiency among general populations, though this is not reflected in the most susceptible groups, namely pregnant women and lactating mothers (8). Published evidence indicates that iodine sufficiency among schoolchildren was accompanied by suboptimal iodine status among pregnant women or lactating mothers in countries designated as iodine sufficient (8). The Islamic Republic of Iran has been declared iodine sufficient (based on the urinary iodine concentrations [UICs] of school-aged children) and free of iodine deficiency disorders (in 2000), following the implementation of universal salt iodization (at 20–40 ppm) and sustained monitoring of the iodine deficiency disorders program. Three national surveys have shown that iodized salt consumption by >95% of the population provided adequate iodine status among school-age children (9 –11). However, recent studies have indicated an inadequate iodine intake among pregnant women and lactating mothers in Iran (12,13).
The American Thyroid Association (ATA) and the Endocrine Society recommend that pregnant and lactating women take vitamin/mineral supplements containing 150 μg iodine daily (14,15). However, in countries with effective iodized salt programs, the WHO does not recommend iodine supplementation for infants or lactating women (16). Evidence suggests that during iodine sufficiency, an infant's iodine needs are sufficiently met by breast milk via a regulatory mechanism in the mammary gland (17). However, partially breast-fed infants (during the weaning period) may be at risk of suboptimal iodine intake (18). There are limited data and no consensus on the differences in iodine nutrition status between breast-fed and formula-fed infants. Some studies have reported a similar iodine status among exclusively breast-fed, exclusively formula-fed, and mixed-fed infants (19), while others have indicated that formula-fed infants have a better iodine status compared to breast-fed infants due to higher iodine content or lower bioavailability of iodine in formula milk (20,21). In a recent meta-analysis, however, different feeding methods (i.e., breast-feeding vs. formula feeding) had no effect on the iodine status of infants residing in either iodine-sufficient or -deficient areas (22).
A study conducted from March 2004 to October 2005 in New Zealand reported that iodine supplementation at 150 or 75 μg/day was insufficient for iodine sufficiency in lactating mothers and their infants (23). Daily consumption of lipid-based nutrient supplements containing 250 μg of iodine had no effect on the iodine status of pregnant women or lactating mothers in Bangladesh (24). However, in Ethiopia, supplementation with either 225 μg/day iodine or iodized salt containing 30–40 ppm iodine led to iodine sufficiency in mothers and their infants (25). The necessity of iodine supplementation in lactating mothers for iodine sufficiency in breast-fed infants has not been explored in iodine-sufficient countries, and the optimal supplementation dose in conjunction with effective salt iodization programs is yet unclear. Therefore, the aims of the present study were to compare the breast milk and urinary iodine status of iodine-supplemented (two dose levels) breast-feeding mothers and their infants with that of formula-feeding mothers not taking iodine supplements and their infants.
Methods
Study design and participants
Lactating mother–neonate pairs (n = 180) referred to four healthcare centers in the south of Tehran were enrolled during their first visit and within three to five days postpartum. Inclusion criteria were as follows: healthy mothers with no history of thyroid disorders, not currently using iodine-containing supplements and disinfectants, who had a singleton birth, and intended to breast-feed exclusively; healthy infants aged three to five days, born full-term (gestational age 37–42 weeks) and at a normal birth weight (2500–4200 g). Simultaneously, formula-feeding mother–infant pairs (n = 60) were randomly selected from the same healthcare centers as above. Inclusion criteria were the same as above except the infants had to be exclusively or partially formula-fed and aged 30–45 days. Maternal information on the age, education, occupation, date of last pregnancy, gravidity, parity, history of miscarriage in previous pregnancies, iodine-containing supplement usage during pregnancy, and the type of delivery were documented, and demographic information on the newborns, including date of birth, sex, birth weight, height, and head circumference measurements, were obtained using an interviewer-administrated questionnaire. Infants with thyrotropin (TSH) concentrations outside the reference range (>5 mIU/L in heel-prick blood samples) were excluded and referred for treatment.
The study protocol was approved by the Institutional Review Board and the independent ethics committee of the Research Institute for Endocrine Sciences (RIES) at Shahid Beheshti University of Medical Sciences and registered in the Iranian registry of Clinical Trials (identification number: IRCT201303164794N8). Written informed consent was obtained before study enrollment.
Randomization and masking
Following enrollment and baseline measurements, lactating mothers were randomly assigned to treatment groups (i.e., the placebo, 150 μg/day iodine, and 300 μg/day iodine) in a 1:1:1 allocation ratio for 12 months. The study was designed as a double-blind study until all data were collected and analyzed. Participants were given potassium iodate (RIES, Tehran, Iran) or placebo tablets prepared by Iran Hormone Pharmaceutical Co. (Tehran, Iran) in similar packaging. For quality control, 10 tablets per treatment group were randomly chosen and tested by the iodine laboratory of RIES. All tablets were proven to be within 5–10% of target dosage, with an 18-month shelf life.
Procedures
Lactating mothers were instructed to take one tablet each day and to avoid taking any other supplements containing iodine during the study period. Mothers and infants were assessed at enrollment and at subsequent follow-up health visits when the infants were aged about 1, 2, 4, 6, 9, and 12 months. Those in the formula-fed group were also followed at appointment visits on months 2, 4, 6, 9, and 12. Compliance with treatment was assessed by tablet counts at each follow-up visit. A spot urine sample was collected at each visit, along with expressed breast milk from the treatment groups. All samples were labeled and kept at −20°C until analysis. A sample of the household salt was also collected on the same day. In addition, the iodine content of three main formula brands used was tested.
Data on birth anthropometric measurements were obtained from birth records. Anthropometric parameters were determined at each visit, and WHO Anthro v3.2.2 (WHO, Geneva, Switzerland) was used to determine age- and sex-specific Z-score values for weight-for-age, weight-for-length, length-for-age, and head-for-age.
Biochemical analyses
The iodine concentration in urine and milk samples was analyzed using the Sandell–Kolthoff (acid-digestion) reaction. The intra-assay coefficients of variation (CV) in UIC values of 8.5, 17.5, and 36.0 μg/dL were 8.5%, 6.2%, and 8.0%, respectively. The inter-assay CV at concentrations of 8.5, 17.4, and 36.4 μg/dL were 10.3%, 9.7%, and 8.0%, respectively. The intra-assay CV in BMIC values of 3.5, 12.7, and 36.2 μg/dL were 8.6%, 6.7%, and 9.3%, respectively. The inter-assay CV at concentrations of 3.3, 12.9, and 35.7 μg/dL were 9.8%, 8.6%, and 12.3%, respectively. Both the intra- and inter-assay CV of infant formula samples were 9.5%. The iodine concentration of salt samples was determined using the iodometric titration method, with 1 ppm sensitivity and 1% CV.
In lactating mothers and infants, a median UIC <100 denotes iodine insufficiency (7). For BMIC, the 100 μg/L cutoff point was selected in the absence of guidelines (26). An iodine concentration in salt samples in the range 20–40 ppm of iodine is considered adequate (7).
Statistical analysis
The primary outcomes were maternal and infant UICs, BMICs, and infant growth parameters (length, weight, and head circumference). Sample size was calculated based on a previous study (27), with an estimated 40 lactating mothers and infants required in each study group. Considering the long follow-up period and vulnerability of the participants, 60 mother–infant pairs were recruited for each group. Post hoc power analysis was performed based on difference in log-transformed mean for maternal UIC between two independent groups. Considering the effect size of 0.57, an error probability ratio (beta/alpha) of 4, and a sample size of 60 per group, the statistical power of the current study was estimated to be 0.847.
The frequency distribution (percentage), mean (standard deviation [SD]), and median (interquartile range [IQR]) are expressed as categorical and continuous variables. Normality was assessed by the Kolmogorov–Smirnove test and a histogram chart. Non- and normally distributed variables with repeated measurements within groups were compared using Freidman and repeated-measures ANOVA, respectively.
Three skewed outcome variables (i.e., BMIC and maternal and infant UICs) were log-transformed before analysis. The associations between BMIC and maternal UICs or between BMIC and infant UICs were assessed by Pearson's correlation using log-transformed data. To determine significant associations of categorical variables, chi-square analysis, Phi coefficient, and Cramer's V were used. Linear mixed-model analysis was used to assess iodine supplement dose effects on maternal and infant UICs and BMICs and to compare to the formula-fed group. For each continuous outcome variable, a separate mixed model was derived, with the time and group as fixed effects and participants as the random effect. To examine the effect of formula feeding on maternal and infant UIC compared to the iodine-supplement groups, factors included in the maternal UIC analysis were: mothers' age, occupation, education, gravidity, use of iodine-containing supplements during pregnancy, and iodine content of salt. For infant UIC analysis, three additional factors—birth weight, frequency of use of formula, and frequency of use of commercial complementary food—were also considered. Analysis of covariance was used to assess differences in infant anthropometric measurements (weight-for-age, weight-for-length, length-for-age, and head-for-age Z-scores) among the treatment and formula-fed groups.
All analyses were conducted using the per protocol principle. Statistical analyses were completed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY) and the R v3.0.2 statistical programming environment using the nlme package, with p-values of <0.05 considered significant.
Results
Between October 2014 and January 2016, 220 mother–neonate pairs were assessed for eligibility for the treatment group; 40 pairs declined to participate or did not meet the inclusion criteria (Fig. 1). The mean ages of the mothers and infants upon enrollment were 28.2 years (SD = 5.1 years) and 4.1 days (SD = 0.7 days), respectively. For the formula-fed group, of the initial 75 exclusively/partially formula-fed infant–mother pairs recruited, 15 were unwilling to participate (Fig. 2). The mean ages of the mothers and infants in this group upon entry were 29.2 years (SD = 5.0 years) and 36.0 days (SD = 5.7 days), respectively.
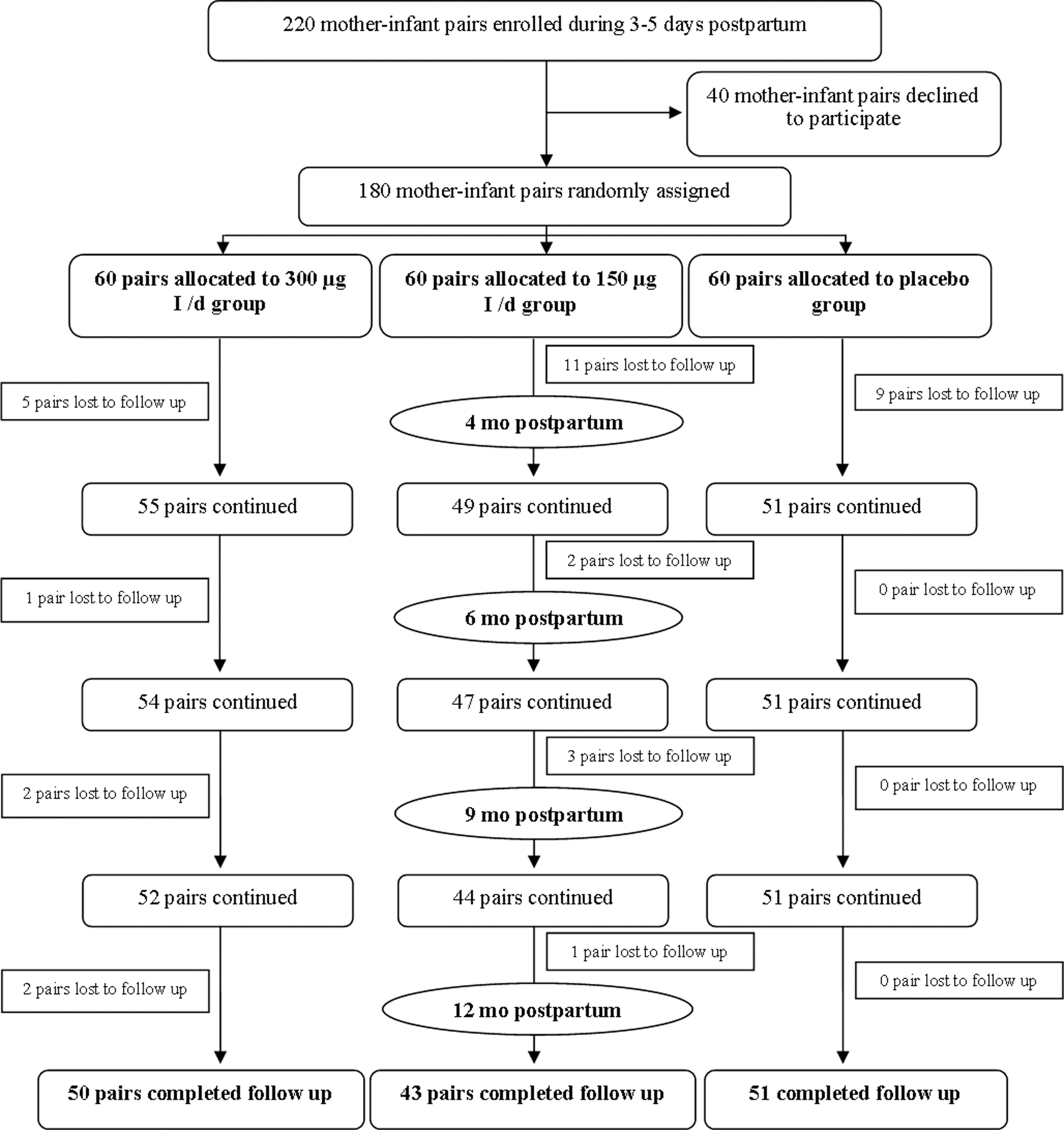
Study profile in the iodine supplementation groups at a glance.
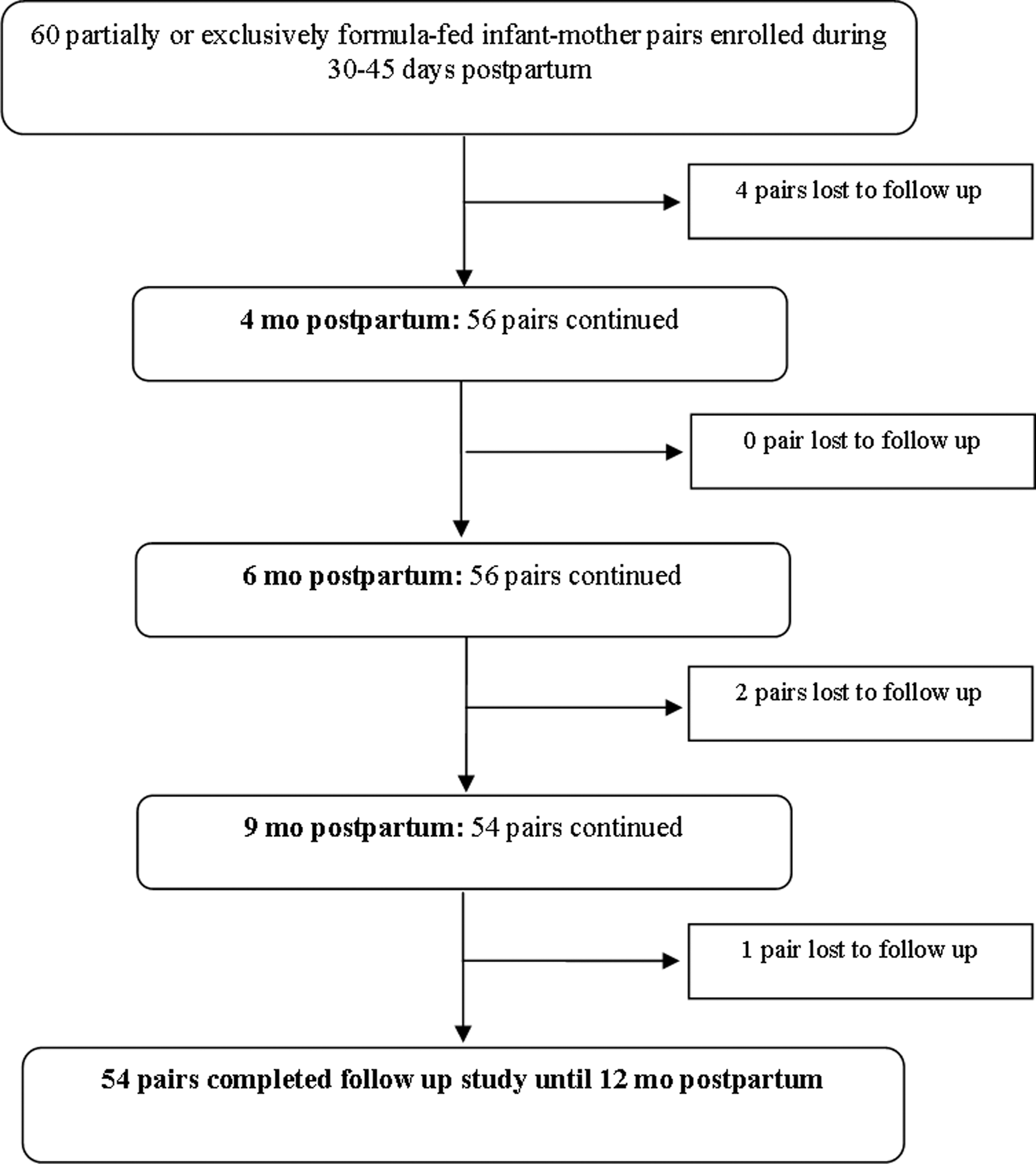
Study profile in the formula-fed group at a glance.
The numbers of participant pairs at the end of the follow-up period were as follows: 300 μg/day iodine group, 50; 150 μg/day iodine group, 43; placebo group, 51; and formula-fed group, 54. Participation withdrawal was mostly attributed to infant reflux, jaundice and hospitalization, mothers' depression, inability to obtain infant urine samples, traveling, and unwillingness to participate. Low compliance (<50%) or exclusive formula-feeding was another reason for exclusion of 17 cases in the treatment group. In the formula-fed group, 22 pairs were excluded due to exclusive breast-feeding. Mean compliance with supplementation was 85% (SD = 12%). Baseline characteristics in the treatment and formula-fed groups are shown in Table 1. Mothers' age, birth weight, head circumference, weight-for-age, and head-for-age Z-score values differed among the formula-fed and treatment groups.
Data are mean ± SD, n (%), median (interquartile range).
NVD, natural vaginal delivery; CS, cesarean section; TSH, thyrotropin.
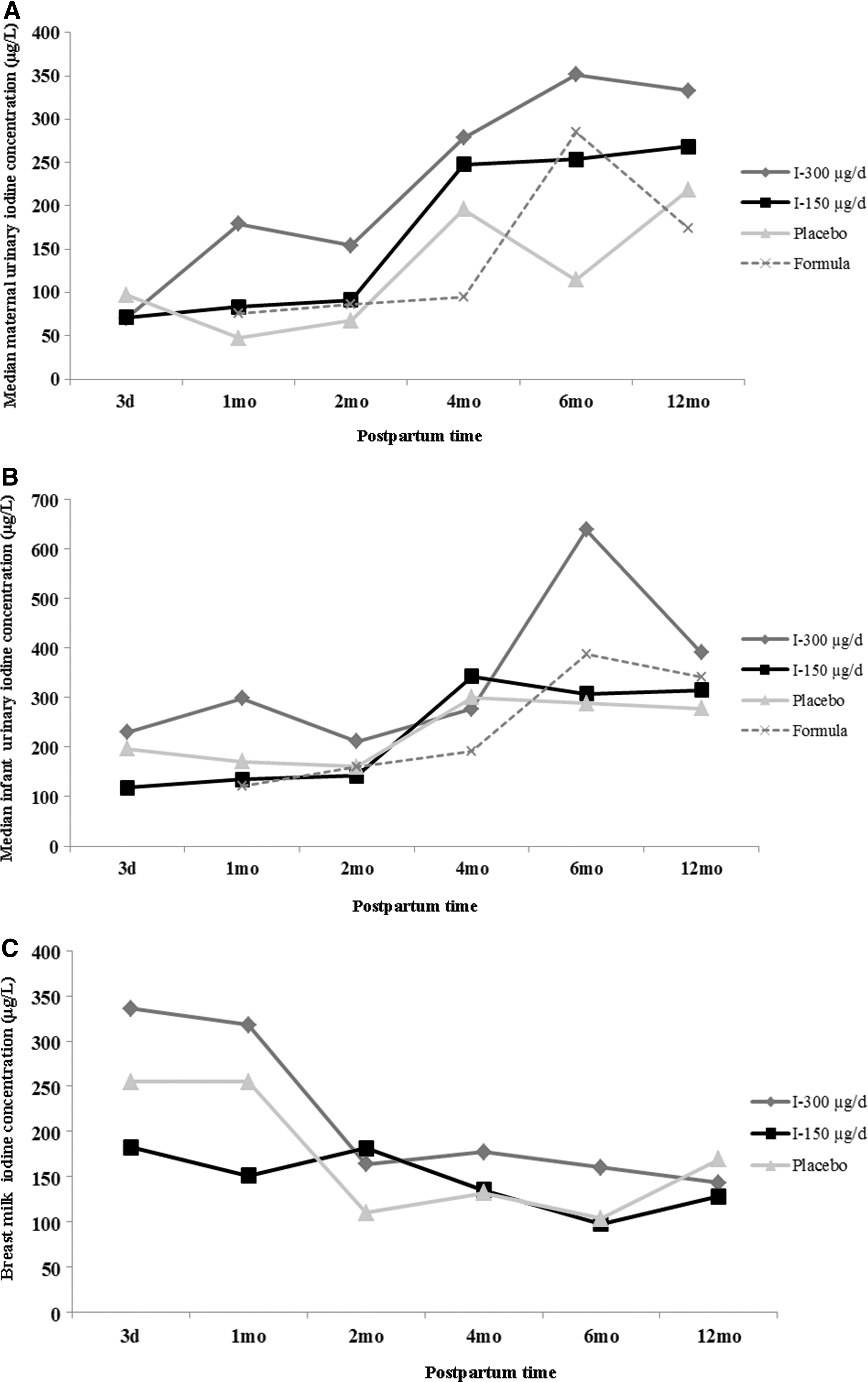
Over the study period, the median (IQR) maternal UIC in the different groups were: 300 μg/day iodine group, 70 μg/L (40–116 μg/L) to 333 μg/L (253–419 μg/L); 150 μg/day iodine group, 71 μg/L (38–111 μg/L) to 269 μg/L (160–528 μg/L); placebo group, 97 μg/L (45–154 μg/L) to 218 μg/L (142–347 μg/L); and formula-fed group: 76 μg/L (40–144 μg/L) to 174 μg/L (92–213 μg/L). The median maternal UIC in the 300 μg/day iodine group was significantly higher than in the other treatment and control groups over the entire study period (p < 0.001; Fig. 3A).
Urinary iodine concentration of mothers (
In all four groups, the infant median UIC at all time points was ≥100 μg/L, and there were no significant differences in infant UICs over the course of the study among all study groups (Fig. 3B).
The median BMICs over the course of the study for treated groups (Fig. 3C) decreased gradually during the 12 months of follow-up. The median BMIC in the 300 μg/day iodine group was significantly higher than in the other treatment groups (p < 0.001).
No significant differences were found in the iodine content of salt among the treatment and formula-fed groups throughout the study period (data not shown).
The effects of different doses of iodine supplements on maternal and infant UIC and BMIC over the intervention period, using mixed-model analysis, are presented in Table 2. Maternal UIC was 1.74 ([confidence interval (CI) 1.63–1.86]; p < 0.001) and 1.31 ([CI 1.23–1.40]; p = 0.001) times higher, respectively, in the 300 and 150 μg/day iodine groups than that in the placebo group; this value increased by 1.32 times ([CI 1.23–1.42]; p < 0.001) in the 300 μg/day iodine group compared to that in the 150 μg/day iodine group. Infant UIC was 1.42 ([CI 1.60–1.77]; p < 0.001) times higher in infants in the 300 μg/day iodine group compared to those in the placebo group. This value in the 300 μg/day iodine group was 1.30 times ([CI 1.24–1.36]; p < 0.001) higher than that of infants in the 150 μg/day iodine group. No significant difference was observed in infant UIC between the 150 μg/day iodine and the placebo groups (p = 0.382). In mothers who received 300 μg/day iodine (p = 0.009) or 150 μg/day iodine (p = 0.001), the BMIC increased significantly compared to that of the placebo group. The BMIC was 1.39 times ([CI 1.34–1.45]; p < 0.001) higher in the 300 μg/day iodine group than that in the 150 μg/day iodine group.
Linear mixed models were used to compare treatment groups.
Ratio of means [CI] with log-transformed data.
CI, confidence interval.
The iodine content of the selected adapted formula brands (0–6 months; n = 9) was 5–18 μg/100 mL, which was often higher than the labeled amount, with differences that ranged from −5 μg/100 mL to +4 μg/100 mL. This value for the selected follow-up formula brands (6–12 months; n = 8) was 8.3–16.0 μg/100 mL. The difference between labeled and measured values ranged from −3.7 μg/100 mL to +3.8 μg/100 mL.
Table 3 presents the effects of formula feeding on maternal and infant UIC over the course of the study. In the mixed-model analysis, maternal UIC was 1.69 ([CI 1.83–2.10]; p < 0.001) and 1.36 ([CI 1.26–1.46]; p = 0.003) times higher in the 300 μg/day iodine and 150 μg/day iodine groups, respectively, compared to the formula-fed group. However, no significant difference was observed in maternal UIC between the placebo and formula-fed groups (p = 0.349), or infant UIC among the formula-fed, 150 μg/day iodine, and the placebo groups. Infant UIC in the 300 μg/day iodine group was 1.58 ([CI 1.49–1.68]; p = 0.003) times higher than that in the formula-fed group.
Linear mixed models were used to compare formula feeding and treatment groups.
Ratio of means [CI] with log-transformed data.
Adjusted for mothers' age, occupation, education, gravidity, use of iodine containing supplements during pregnancy, and iodine content of salt.
Adjusted for mothers' age, occupation, education, gravidity, use of iodine containing supplements during pregnancy, iodine content of salt, birth weight, and frequency use of formula and commercial food.
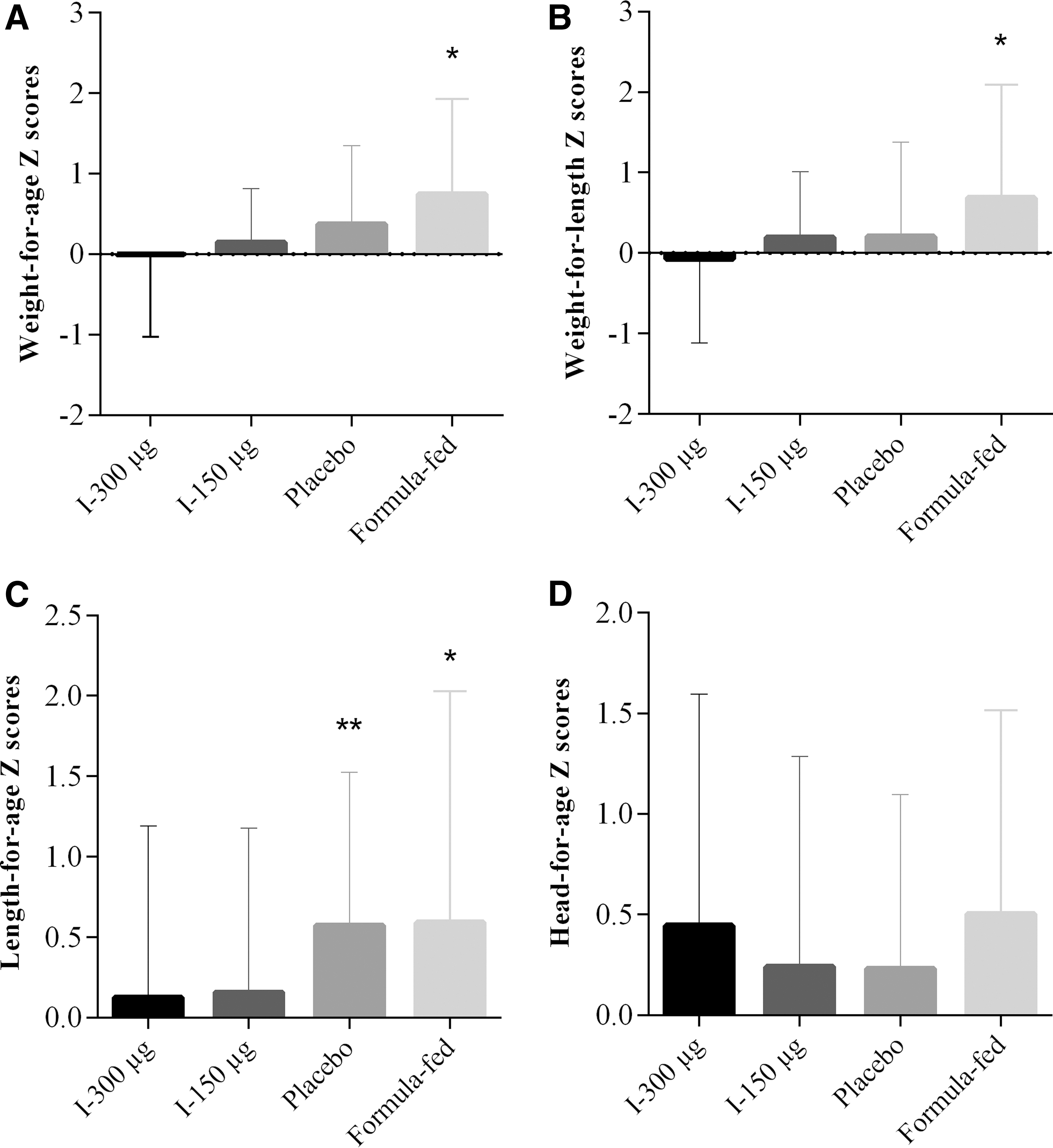
After baseline value adjustment, the infant anthropometric Z-score values did not differ among the groups at any time, except at 12 months where the Z-scores for weight-for-age, weight-for-length, and length-for-age were significantly higher in formula-fed infants than those in any of the treatment groups. The length-for-age Z-scores were significantly higher in infants of the placebo group compared to those in the other treatment groups (Fig. 4A–D).
(
Discussion
To the best of the authors' knowledge, this study is the first multicenter randomized, double-blind, placebo-controlled trial to assess the effect of different doses of iodine supplements on the iodine status of lactating mothers and infants and to compare the iodine status of supplemented breast-feeding and formula-feeding mothers and infants during the first year of life in a country designated as iodine sufficient. The findings indicate that supplementation with 300 μg/day iodine resulted in significantly higher maternal and infant UICs and BMICs than for those supplemented with 150 μg/day iodine or placebo. The iodine status of formula-feeding mothers and of those receiving the placebo was not different. However, UICs in mothers who received iodine supplementation (300 μg/day iodine or 150 μg/day iodine) were significantly higher compared to those of the formula-feeding group. Although infants in the 300 μg/day iodine group had significantly higher UICs, the iodine status of formula-fed infants was similar to those in the 150 μg/day iodine or placebo groups.
Previous studies have suggested that due to the compensatory mechanism in the mammary glands and upregulation of the sodium–iodide symporter, higher levels of BMIC may correspond with lower UICs and suboptimal iodine status among lactating mothers (28 –30). Hence, measuring UIC without BMIC is not the best criterion for diagnosing iodine deficiency during lactation (17). It was found that inadequate UIC persisted until four months postpartum in formula-feeding mothers, showing that excretion of iodine into breast milk may not be the only reason for the lower median UICs in the early postpartum period. In Bangladesh, supplementation with lipid-based nutrient supplements containing 250 μg/day iodine during pregnancy and the postpartum period did not increase maternal UIC at 36 weeks of gestation or at six months postpartum. This observation has been attributed to the clearance of a greater fraction of circulating iodide by the thyroid gland to restore depleted thyroidal iodine contents (24). Iodized salt is the main dietary iodine source for all age groups, including pregnant and lactating women in Iran (9,10). Hence, the amount of salt intake and its iodine content are two major determinants of iodine nutritional adequacy (27). Iranian pregnant women are advised to reduce salt intake to prevent hypertensive disorders (undocumented observation), and in most cases continue to do so through the postpartum period, which may be another reason for iodine deficiency among lactating mothers.
The analysis of mineral content over the course of lactation has revealed that the BMIC tends to be higher in the first few days postpartum and then decreases through lactation (31,32). Chierici et al. reported a decline in BMIC in both un-supplemented and iodine-supplemented mothers (116 μg potassium iodide over 90 days postpartum) (33). Similarly, a study from New Zealand showed that the BMIC decreased by 40% in the placebo group during the first six months postpartum (23). In another study, median BMIC decreased at six months of lactation in mothers, despite receiving weekly iodine supplement or well iodized salt (25). In agreement with the above, BMIC decreased gradually over the course of the present study in the treatment groups.
There is no consensus about the cutoff values for BMIC that will ensure iodine sufficiency in full-term breast-fed infants (34 –37). A recent meta-analysis has shown that iodine concentrations of 152 and 71 μg/L in colostrum and mature breast milk, respectively, can ensure iodine sufficiency among breast-fed infants residing in countries with iodine sufficiency (22). In agreement, Dold et al. proposed a BMIC reference range of 60–465 μg/kg for iodine adequacy in lactating mothers and breast-fed infants in iodine-sufficient populations (17). In the current study, BMICs in all groups were within acceptable limits at all study time points based on the median BMIC cutoff value of 100 μg/L, despite being higher in the 300 μg/day iodine group. Mulrine et al. reported that in New Zealand, prior to mandatory fortification of bread in 2009, the BMIC in those supplemented with either 75 or 150 μg/day iodine was 1.3 and 1.7 times higher, respectively, than it was in those who received the placebo. However, this value remained <100 μg/L over six months of lactation (23). The present findings are compatible with a previous study indicating that lactating mothers with higher iodine intakes had greater fractional iodine excretion in their breast milk compared to that in their urine. However, with inadequate iodine intake, a relatively constant proportion (approximately 33%) of total iodine was excreted in breast milk (17).
The WHO recommends a cutoff of 100 μg/L for assessing the iodine status of children aged <2 years (7). However, there is no definitive evidence to support this cutoff in infancy. Though there is no consensus on the favorable intake level and the tolerable upper intake level, Zimmermann et al. demonstrated that the current WHO median UIC cutoff for iodine sufficiency in infancy may be too high for the first week after birth (38), while Dold et al. proposed a minimum UIC threshold of 125 μg/L and speculated that the current median UIC cutoff may be too low for infants aged two to five months (39). The current study indicates that infant UICs in the 300 μg/day iodine group were significantly higher than those in all the other study groups, though no significant differences were found among the 150 μg/day iodine, placebo, and formula-fed groups. This may be because the iodine content of infant formulas was comparable to the BMICs in the 150 μg/day iodine and placebo groups. In industrialized countries with effective iodized salt programs, such as Switzerland, it has been demonstrated that weaning infants not receiving iodine-containing commercial foods may be a risk for inadequate iodine intake (18), possibly because mothers are discouraged from adding extra salt to home-prepared complementary foods or from feeding cow's milk to infants during the first year (18). However, the present study observed that the iodine status of infants in all treatment and formula-fed groups was within optimal range at all time points, and this status persisted during the weaning period when the contribution of complementary foods increased markedly. The findings reaffirm the WHO recommendation that in areas with sustained and effective salt iodization programs (at 20–40 ppm of iodine), iodine requirements of lactating mothers and infants younger than two years of age are met by iodized salt (16). Hence, caution should be taken in young children, who are vulnerable to excessive iodine exposure, since their thyroid gland is more susceptible to the inhibitory effect of high iodine doses than the adult gland. For instance, in Japan and China, a transient elevation of TSH was reported in some neonates born to mothers chronically exposed to high doses of iodine, mainly from food and drinking water (40,41). Also, in Nepal, a prevalence of 7.4% subclinical hypothyroidism and <1% overt hypothyroidism was reported among infants aged 6–24 months after exposure to excessive iodine intake (42).
Prospective studies conducted in Spain (43), China (44), India (45), and Bangladesh (46) have indicated that higher maternal UICs during pregnancy correlated with more advantageous anthropometric birth outcomes. However, the relationship between postnatal iodine status and growth parameters is less clear. Studies on the effect of iodine supplementation through either iodized salt or iodized oil on growth showed controversial results. In cross-sectional studies, modest positive correlations were found between iodine intake and child growth. However, controlled intervention studies did not indicate any beneficial effects on somatic growth rates (2). For instance, in Morocco, although the UIC was higher in infants whose mothers received supplements compared to infants supplemented directly, no differences in anthropometric parameters were observed (47). Consistent with the above, in the current study, infants in the treatment groups did not differ in anthropomorphic measures, except that the length-for-age Z-score was greater in the placebo group at 12 months of age.
This study has a few limitations. First, using a single urine and breast milk sample is a poor indicator of the iodine status due to significant day-to-day variations (48). Second, the limited number of mothers who selected formula feeding during early postpartum days may increase the risk of selection bias, since these mothers might have differed in general health and provided different levels of care for their infant than mothers who chose to breast-feed. Third, it was not possible to estimate dietary iodine intake through the assessment of iodized salt consumption. Fourth, although none of the participants reported thyroid disorders during the study period, maternal and infant thyroid function was not assessed by thyroid parameters. Last, caution should be taken in interpreting these results, as creatinine levels in the collected urine samples were not measured, in order to ensure misclassification due to urinary dilution effect has not occurred.
In conclusion, the findings reveal that supplementation of breast-feeding mothers with either 300 or 150 μg/day iodine improved maternal UIC compared to the placebo and the formula-feeding groups. Except in the first few months postpartum, the iodine status of mothers in supplemented and un-supplemented groups indicated iodine sufficiency over the study period. Although the UICs in infants of the 300 μg/day iodine group increased significantly, the iodine status of infants in all groups studied was within the optimal range during the first year of life. The findings are compatible with the WHO recommendation and contrast with those of the ATA (14) and the Endocrine Society (15) that in iodine-sufficient areas with effective salt iodization, lactating mothers and infants have no need for iodine supplements. Further studies are needed to confirm the results in other iodine-sufficient countries.
Footnotes
Acknowledgments
This study was supported by financial grant (no. 480) from the Research Institute of Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Iran Hormone Pharmaceutical Co. (Tehran, Iran) supplied the iodine supplements and placebo tablets free of charge. We would like to thank the mothers and their infants who participated in the study and the laboratory personnel of the Endocrine Research Center at Shahid Beheshti University of Medical Sciences for their assistance.
Author Disclosure Statement
None of the authors has any personal or financial conflicts of interest.