
Abstract
Background:
Recent studies have reported improved survival in patients with thyroid cancer. This study evaluated the changes in disease-specific survival (DSS) of patients with differentiated thyroid cancer (DTC) in association with clinicopathologic characteristics from 1996 to 2005 in Korea.
Methods:
This was a retrospective, multicenter cohort study. A total of 4398 DTC patients were included, and they were classified according to the year of initial surgery: 1996–2000 (period 1), 2001–2003 (period 2), and 2004–2005 (period 3).
Results:
During the study period, patient age and the proportion of papillary thyroid cancer increased gradually. Primary tumors became smaller (2.3 ± 1.4 cm at period 1 to 1.5 ± 1.2 cm at period 3; p < 0.001). The proportion of high-volume lymph node metastases decreased significantly (20% at period 1 to 13% at period 3; p for trend <0.001). DSS differed significantly according to period during the median 10 years follow-up (p = 0.002). The 10-year DSS rates were 98.0%, 98.7%, and 99.2% in periods 1, 2, and 3, respectively. After adjusting for various characteristics, the disease-specific mortality risk was significantly lower during period 2 (hazard ratio = 0.49 [confidence interval CI 0.25–0.90], p = 0.021) and period 3 (hazard ratio = 0.40 [confidence interval 0.21–0.77], p = 0.006) compared to that of period 1. This trend was also significant in a subgroup analysis of low (I–II) and high (III–IV) TNM stages.
Conclusions:
The disease-specific mortality of patients with DTC in Korea decreased over time. Earlier detection of small DTCs with less extensive disease and standardization of treatment may be associated with this phenomenon.
Introduction
O
In Korea, the age-standardized rate of thyroid cancer incidence was 43.3 per 100,000 in 2014, and has increased rapidly, with an annual percent change of 22.4% from 1999 to 2011 (9). A recent study analyzing data from Statistics Korea reported an increase in the age-standardized mortality in patients with thyroid cancer from 1985 to 2004 and a subsequent decrease from 2004 to 2015 (10,11). However, that study did not consider information pertaining to the onset of disease or the associations between thyroid cancer mortality and pathological subtypes over time.
This study evaluated changes in the clinical outcomes of differentiated thyroid cancer (DTC), especially disease-specific mortality, in association with changes in the clinical and pathological characteristics using a large multicenter DTC cohort from 1996 to 2005 in Korea.
Methods
Study cohort
This multicenter, retrospective cohort study included DTC patients who had their initial thyroid surgery between 1996 and 2005 at five tertiary referral hospitals in Korea, including Asan Medical Center, Chonnam National University Hwasun Hospital, Pusan National University Hospital, Ulsan University Hospital, and Chungnam National University Hospital. Initially, 4950 patients with DTC, including PTC and follicular thyroid cancer (FTC), were screened. Patients without adequate pathological reports or who were followed up for less than one year were excluded. Finally, 4398 patients were eligible for analysis. This protocol was approved by the Institutional Review Board in each institute (Asan Medical Center: 2016-1301; Chonnam National University Hwasun Hospital: CNUHH-2017-053; Pusan National University Hospital: 1701-014-051; Ulsan University Hospital: 2016-12-031; and Chungnam National University Hospital: CNUH 2017-01-018). Informed consent was waived due to the retrospective design.
Definitions
Patients were classified into three groups according to the year of their initial surgery: between 1996 and 2000 (period 1; n = 969), between 2001 and 2003 (period 2; n = 1337); and between 2004 and 2005 (period 3; n = 2092). This classification was based on the number of DTC cases in each year. The number of DTC patients increased gradually each year and jumped between 2001 and 2004 with a significant increase in tumors ≤1 cm (Fig. 1).
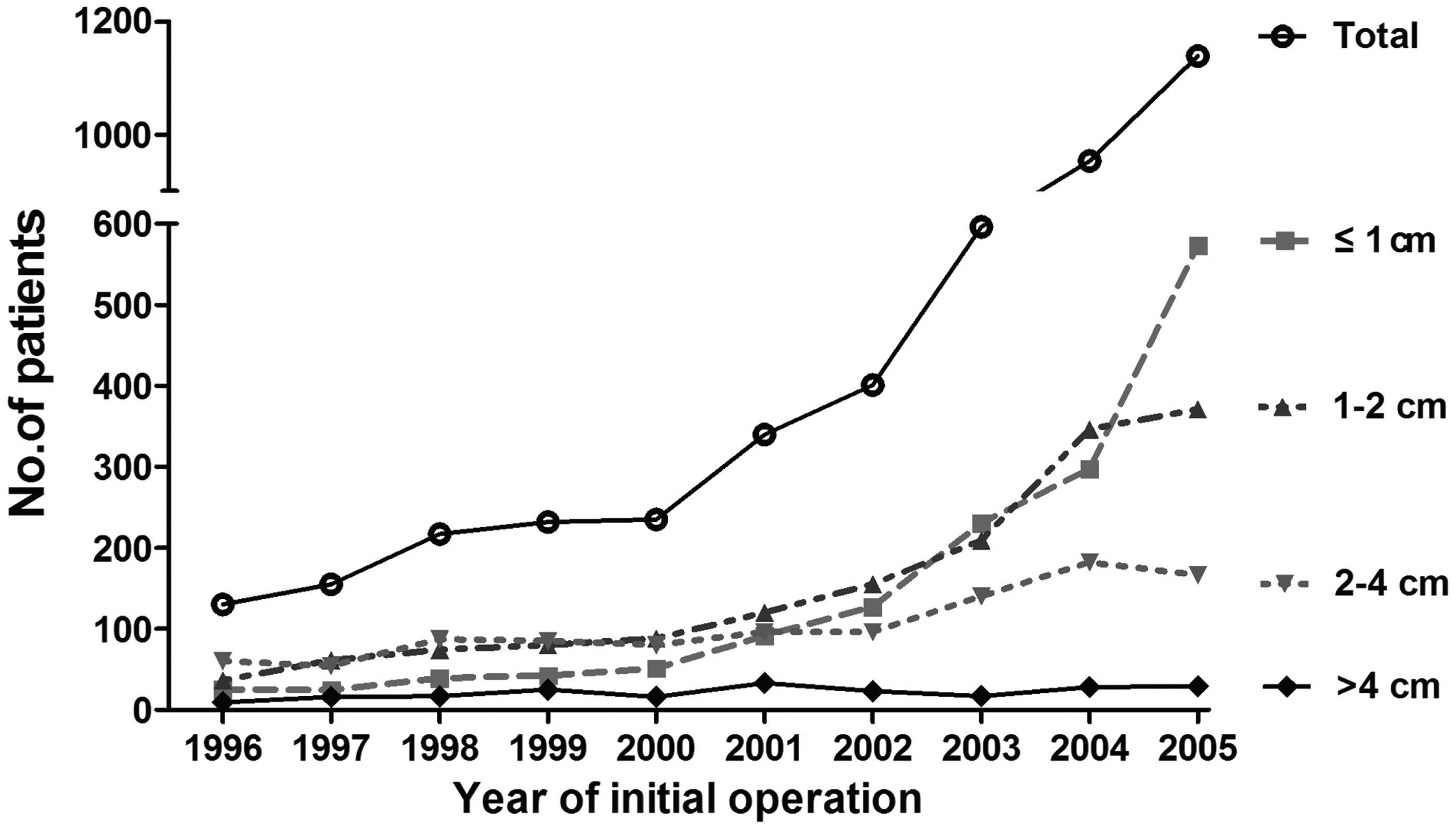
Number of differentiated thyroid cancer (DTC) cases in Korea from 1996 to 2005, according to the initial surgery year and the primary tumor size. The number of DTC cases each year increased gradually and jumped between 2001 and 2004, with a significant increase in tumors ≤1 cm. The number of DTCs ≤4 cm in size increased gradually, while that of DTCs >4 cm did not change significantly.
Cervical LN metastasis was also classified according to the number of metastatic LNs as low-volume LN metastasis (≤5 metastatic LNs) and high-volume LN metastasis (>5 metastatic LNs), as described previously (12).
Disease-specific survival (DSS) was defined as the time interval between the initial surgery and the last censoring or death caused by DTC. Disease-free survival (DFS) was defined as the time interval between the initial surgery and the first detection of structural persistent/recurrent disease.
Management and follow-up
There were no significant changes in the guidelines for managing patients or the treatment strategies of patients with DTC in the tertiary hospitals in Korea (13,14). In general, 3554 (81%) patients underwent total thyroidectomy, and 3020 (69%) patients underwent prophylactic central LN dissection. After the initial surgery, 3024 (69%) patients underwent subsequent radioactive iodine (RAI) therapy. With the increase in early-stage cancers, the proportion of patients who underwent a total thyroidectomy and received RAI therapy decreased over time (p < 0.001 and p < 0.001; Table 1). However, the proportion of patients who underwent prophylactic central LN dissection remained unchanged (p = 0.31; data not shown).
p-Values for the categorical variables were calculated by the chi-square test.
TNM stages were determined by the eighth TNM staging system.
RAI, radioactive iodine; PTC, papillary thyroid cancer; FTC, follicular thyroid cancer.
After the initial therapy, patients took levothyroxine to suppress TSH and received regular follow-up with a physical examination, thyroid function test, serum thyroglobulin (Tg), anti-Tg antibody measurement, and neck ultrasonography (USG) (13 –16).
Variables
Various clinicopathologic characteristics of the patients were collected for analysis from electronic medical records: age at diagnosis, sex, extent of surgery, use of RAI, pathology, size, or the presence of extrathyroidal extension (ETE) of the tumor, the presence of cervical LN metastasis, the number of metastatic LNs, the presence of distant metastasis, and the initial tumor-node-metastasis (TNM) stage according to the eighth edition of the American Joint Committee on Cancer/Union for International Cancer Control TNM staging system (17,18).
Statistics
R studio v3.4.0 and the R libraries xlsx, lubridate, survival, car, and gdata were used to analyze the data in the present study (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline clinical and pathological characteristics
The baseline clinical and pathological characteristics of the 4398 patients with DTC are described in Table 1. Mean patient age was 45.7 ± 12.1 years, and 87% were female. The majority had PTC (n = 4326; 96%), including its variants, and mean primary tumor size was 1.8 ± 1.3 cm. Cervical LN metastases were present in 2084 (47%) patients, and initial distant metastases were found in 65 (1%) patients. According to the eighth TNM staging system, 85%, 12%, 2%, and 0.6% of the patients were stage I, II, III, and IV, respectively.
The clinical and pathological characteristics of the patients were compared according to the year of the initial surgery (Table 1). Mean patient age increased from period 1 (44.3 ± 12.4) to period 3 (46.3 ± 11.9; p < 0.001). However, no significant differences in the proportion of patients aged ≥55 years or that of females were observed according to period. The proportion of patients with PTC increased significantly (95% at period 1 to 97% at period 3; p for trend <0.001), and primary tumor size decreased significantly (2.3 ± 1.4 cm at period 1 to 1.5 ± 1.2 cm at period 3; p < 0.001). The number of DTCs ≤4 cm increased gradually annually, while that of DTCs >4 cm did not change significantly (Fig. 1). The proportion of patients without cervical LN metastasis (N0) increased significantly by 43% in period 1 and by 55% in period 3 (p for trend <0.001). The proportion of patients with high-volume LN metastases decreased significantly by 20% in period 1 and by 13% in period 3 (p for trend <0.001). There were no significant changes in the presence of synchronous distant metastasis of DTC or the TNM stages over time.
Changes in DFS according to the period of the initial surgery
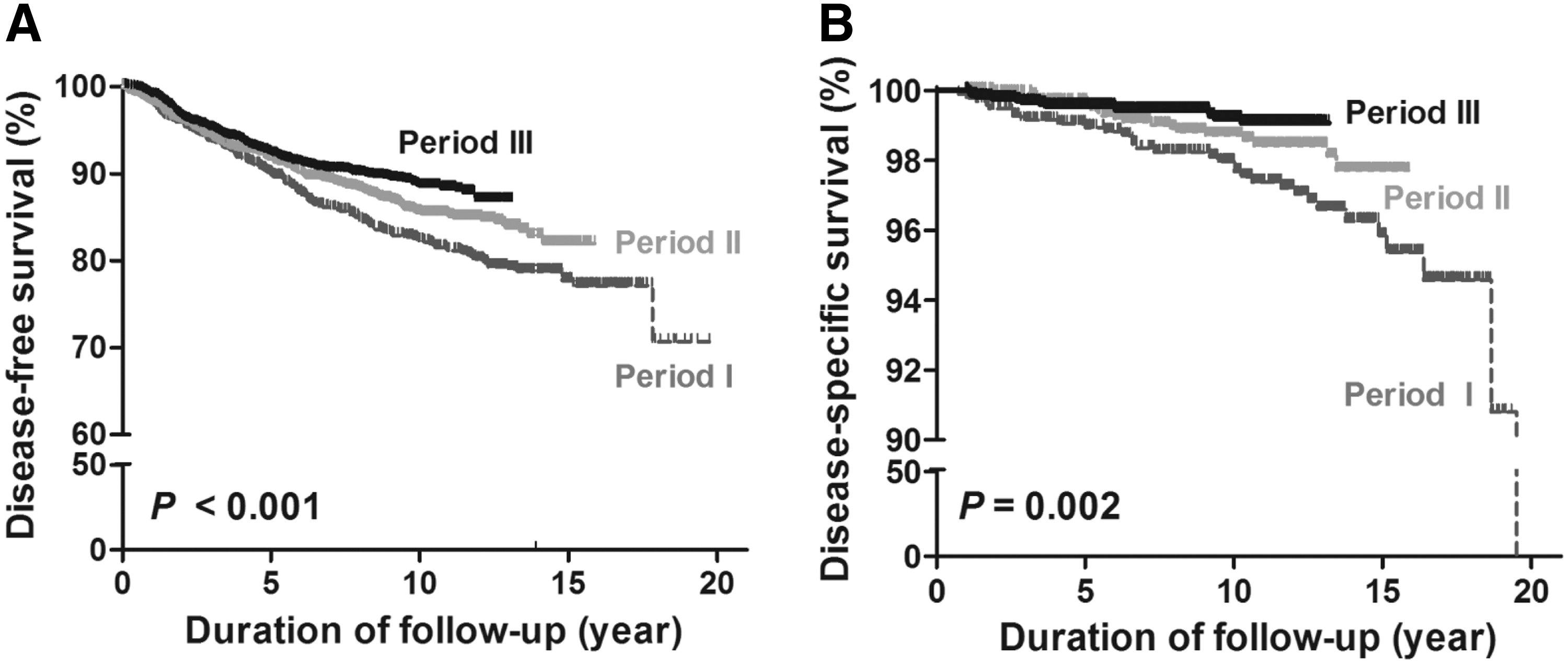
The incidence of structural persistent/recurrent disease and DFS was evaluated according to the year of the initial surgery during a median of 10.4 years (interquartile range 8.2–21.2 years) of follow-up. The median follow-up duration was 12.4, 10.5, and 9.7 years in periods 1, 2, and 3, respectively (Table 2). Structural persistent/recurrent disease was detected in 171 (18%) patients, 178 (13%) patients, and 216 (10%) patients in periods 1, 2, and 3, respectively (p for trend <0.001). The DFS curves differed significantly according to period (p < 0.001; Fig. 2A). The five-year DFS rates were 90.9%, 91.7%, and 92.3% in periods 1, 2, and 3, respectively. The 10-year DFS rates were 82.3%, 85.5%, and 88.5% in periods 1, 2, and 3, respectively. The risk of structural persistent/recurrent disease in period 3 was significantly lower compared to that in period 1 (hazard ratio [HR] = 0.79 [confidence interval [CI] 0.65–0.97], p = 0.033) after adjusting for age, sex, treatment variables, pathological subtype, primary tumor size, the presence of ETE, cervical LN metastases, number of metastatic LNs, and the presence of distant metastasis (Table 3).
(
p-Value was estimated by the Cochran–Armitage trend test.
Age (≥55 years)and sex of patient, extent of surgery (total thyroidectomy), use of radioactive iodine, tumor pathology, primary tumor size (>4 cm), the presence of extrathyroidal extension, nodal stage by eighth TNM staging system, number of metastatic lymph nodes (>5), and the presence of distant metastasis were adjusted.
HR, hazard ratio; CI, confidence interval; Ref, reference.
Changes in DSS according to the period of the initial surgery
Disease-specific mortality and DSS were evaluated according to the year of the initial surgery. Disease-specific mortality decreased significantly from period 1 to period 3 (p for trend <0.001; Table 2). The DSS curves differed significantly according to period (p = 0.002; Fig. 2B). The 10-year DSS rates were 98.0%, 98.7%, and 99.6% in periods 1, 2, and 3, respectively. The risk of disease-specific mortality was also evaluated according to the period after adjusting for age, sex, treatment variables, pathological subtype, primary tumor size, the presence of ETE, cervical LN metastases, number of metastatic LNs, and the presence of distant metastasis. The risk of disease-specific mortality in period 2 (HR = 0.49 [CI 0.26–0.92], p = 0.027) and period 3 (HR = 0.41 [CI 0.21–0.79], p = 0.008) was significantly lower compared to that in period 1 (Table 3).
DSS was also evaluated in patients with low TNM stages (I–II) and high TNM stages (III–IV). DSS differed significantly according to period in the low TNM stage subgroup (p = 0.031; Fig. 3A). The 10-year DSS of patients with low TNM stages was 99.1% in period 1, 99.4% in period 2, and 99.6% in period 3. The risk of disease-specific mortality in period 3 (HR = 0.36 [CI 0.15–0.86], p = 0.021) was significantly lower compared to that of period 1 in this subgroup. DSS also differed significantly according to period in the high TNM stage subgroup (p = 0.011; Fig. 3B). The 10-year DSS was 50.3% in period 1, 75.5% in period 2, and 82.8% in period 3. The risk of disease-specific mortality in period 2 (HR = 0.41 [CI 0.17–0.99], p = 0.050) and period 3 (HR = 0.27 [CI 0.10–0.70], p = 0.007) was also lower compared to that in period 1.
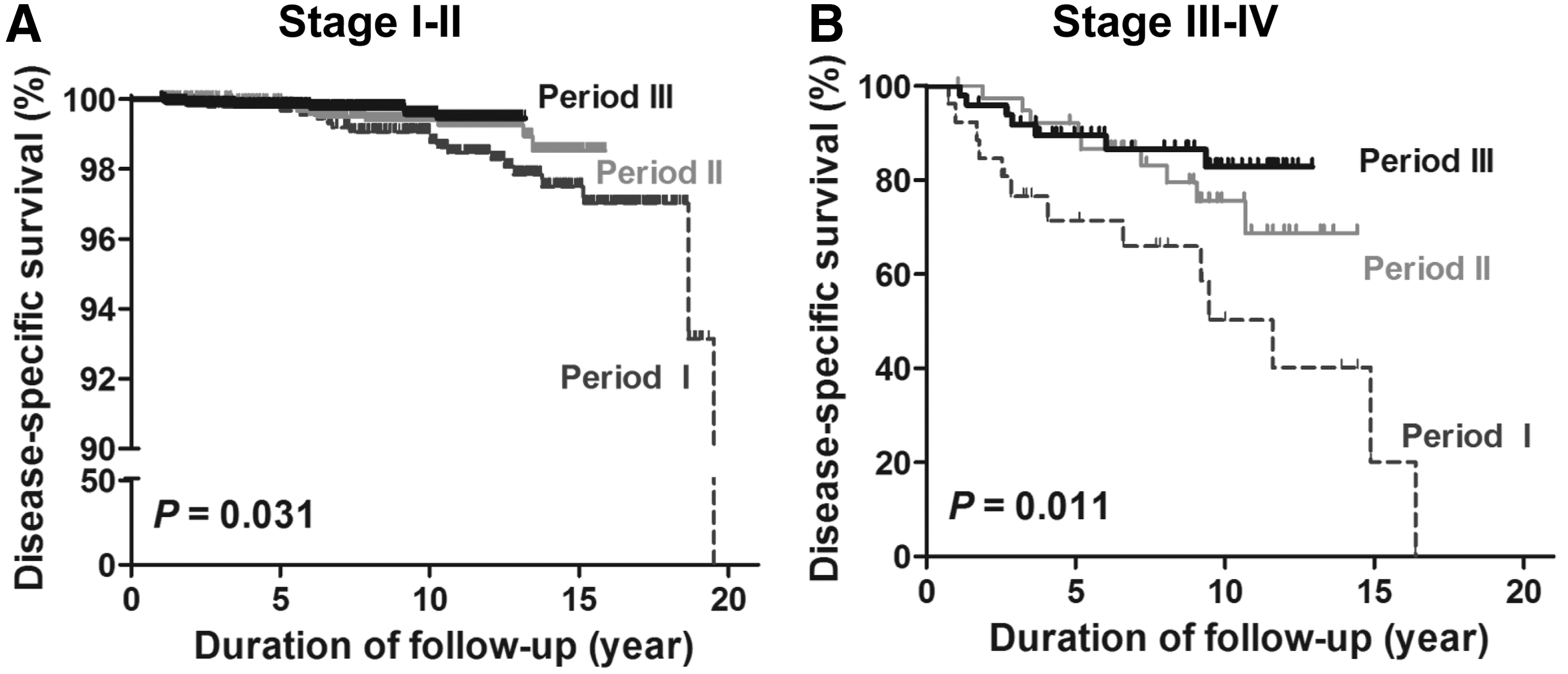
DSS curves of patients with DTC in Korea from 1996 to 2005 according to the eighth tumor-node-metastasis (TNM) staging system. DSS curves of patients with DTC were significantly different according to the year of the initial surgery in (
When DSS was evaluated in patients with microscopic tumors (≤1 cm), DSS also differed significantly according to period (p = 0.003; Supplementary Fig. S1; Supplementary Data are available online at
Discussion
This study confirms the increase in the incidence of small PTCs with less extensive LN metastasis from 1996 to 2005. Primary tumor size decreased significantly with a significant increase in tumors without cervical LN metastases. The proportion of high-volume LN metastases also decreased significantly. With the changes in the pathological characteristics of DTC, the disease-specific mortality rate of DTC according to the year of the initial surgery decreased over time, which is consistent with a previous report from Korea (10). This improved survival of DTC was also significant after adjusting for various clinical and pathological characteristics. Compared to patients who were diagnosed between 1996 and 2000 (period 1), patients who were diagnosed from 2004 to 2005 (period 3) had a 60% reduced risk of disease-specific mortality from DTC after adjusting for age, sex, treatment variables, pathology of DTC, primary tumor size, the presence of ETE, the extent of LN metastases, and the presence of distant metastasis, which are well known risk factors for disease-specific mortality of thyroid cancer (19). Furthermore, this trend in improved patient survival was also observed in both subgroups of low (I–II) and high (III–IV) TNM stages.
Given the widespread use of high-resolution thyroid USG in Korea since 1999 (10), detection of small subclinical PTC has increased significantly, resulting in changes in the composition of DTCs with a favorable behavior (8). A significant increase in small PTCs with less extensive disease was observed in the cohort, and this may be why DSS improved in this study. However, the findings suggest that the increased detection of subclinical DTCs with favorable behavior is not the only reason for the improved survival of DTC because the DSS of DTC improved independently of various clinical and pathological characteristics, and it also improved in patients with extensive disease and high TNM stages. Advanced and extensive DTCs can also be detected earlier with the development of high-resolution USG and wide use of USG. Even though the DFS of DTC was not different between period 1 and period 2 after adjusting for various characteristics, the DSS of DTC improved significantly during this period. This finding also suggests that improved postoperative surveillance could lead to earlier detection of structural recurrences, thereby improving DSS. More standardized and multidisciplinary management of DTC by experienced physicians also might be a reason for the decrease in disease-specific mortality from extensive cancers (6,10).
The recent increase in the incidence of thyroid cancer worldwide has been regarded solely as over-diagnosis resulting from the increasing use of thyroid USG because previous studies reported no changes in disease-specific mortality from thyroid cancer (1). Problems associated with over-diagnosis or over-treatment of low-risk, small thyroid cancers has arisen (5), and the U.S. Preventive Services Task Force recommends against screening for thyroid cancer in asymptomatic adults (20). However, the present findings suggest a possible benefit of thyroid cancer screening. Furthermore, a recent study analyzing the SEER data reported an increase in the incidence of advanced stage thyroid cancer and mortality due to thyroid cancer in the United States, suggesting a true increase in the occurrence of thyroid cancer in the United States (4).
This study had some limitations due to its retrospective study design. This was a multicenter cohort study, and patient management may have differed among the institutions. The impact of postoperative management, such as reoperation or repeated RAI treatment, could not be determined in this study. Furthermore, the overall management of thyroid cancer, including the diagnosis, treatment, and follow-up, may have changed during the study and follow-up periods. Nevertheless, the general principles and clinical practice for managing patients with DTC was similar among the five referral hospitals (5,13). An attempt was made to minimize the potential bias by adjusting the treatment variables during the study.
This large DTC cohort accounted for about 10% of all patients with thyroid cancer in Korea when compared to the national cancer registry database of Korea (9). Furthermore, disease-specific mortality was evaluated according to the year of the initial surgery with a relatively long follow-up. The study design differed from that of previous studies that have evaluated disease-specific mortality using the year of death using national statistics data (10,11). Although the age-adjusted mortality rate is considered an objective statistic in cancer, it can blur the impact of intervention because cases from many years contribute to the deaths in a given year (21). The approach of an incidence-based mortality assessment was strong in that it considered various factors associated with cancer onset (22).
In conclusion, the disease-specific mortality of DTC decreased over time in this Korean multicenter cohort. This trend was independent of various risk factors for DTC mortality and was also detected in both subgroups of low (I–II) and high (III–IV) TNM stages. Earlier detection of small DTCs with less extensive disease and treatment standardization may be associated with this phenomenon.
Footnotes
Acknowledgments
This study was supported by the Korean Thyroid Association Young Investigator Award 2015.
The Korean Thyroid Cancer Study Group: Min Ji Jeon, Won Gu Kim, Tae Yong Kim, Young Kee Shong, and Won Bae Kim (Division of Endocrinology and Metabolism, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul); Hosu Kim, Young Nam Kim, Tae Hyuk Kim, Sun Wook Kim, and Jae Hoon Chung (Division of Endocrinology and Metabolism, Department of Medicine, Thyroid Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul); Hee Kyung Kim and Ho-Cheol Kang (Department of Internal Medicine, Chonnam National University Medical School, Gwangju); Eun Heui Kim, Bo Hyun Kim, and In Joo Kim (Division of Endocrinology and Metabolism, Department of Internal Medicine, Biomedical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan); Hyon-Seung Yi, Kun Soon Kim, and Minho Shong (Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon); Eun Sook Kim (Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan); and Eun Kyung Jang and Eui Young Kim (Department of Endocrinology, Dongnam Institute of Radiological and Medical Sciences Cancer Center, Busan, Korea).
Author Disclosure Statement
The authors have nothing to disclose.