
Abstract
Background:
The serum thyrotropin receptor antibody (TRAb) titers of Graves' disease (GD) patients are known to increase after radioiodine (RAI) therapy, and they can remain high for years. The incidence of neonatal hyperthyroidism (NH) among newborns of mothers with GD who conceived after RAI therapy has not been previously reported. The aims of this study were to investigate the incidence of NH among newborns of mothers who conceived within two years after RAI therapy, and to identify predictors of NH.
Methods:
GD patients (n = 145) who conceived within two years after RAI therapy were retrospectively reviewed, and information regarding their newborns was collected.
Results:
Of the 145 pregnant women, 54 (37%) were treated with antithyroid drugs or potassium iodide for maternal hyperthyroidism during the first trimester. There were eight newborns with NH, resulting in an incidence of 5.5%. Seven of the eight mothers whose newborns had NH were treated with antithyroid drugs or potassium iodide during their pregnancy. The incidence of NH among the newborns of mothers who conceived within 6–12 months after RAI therapy was 8.8%, within 12–18 months was 5.5%, and within 18–24 months was 3.6%. Multivariate analysis revealed that the TRAb values in the third trimester were the only risk factor for NH. The cutoff TRAb value in the third trimester for predicting NH was 9.7 IU/L (reference value <2.0 IU/L).
Conclusions:
The incidence of NH among newborns of mothers who conceived within two years after RAI therapy was 5.5%. The fetuses of pregnant GD patients whose TRAb value is high in the third trimester should be carefully followed by an obstetrician during pregnancy, and the newborns should be carefully followed by a pediatrician after birth.
Introduction
R
The fetal thyroid gland begins to synthesize thyroid hormones between weeks 10 and 12 of gestation. Maternal TRAbs transferred to the fetus through the placenta may stimulate the fetal thyroid gland starting as early as 18 weeks of pregnancy (5 –10). The incidence of fetal and neonatal hyperthyroidism (NH) was reported to be between 1% and 5% in women with active or a past history of GD (8,11). TRAb values of GD patients who underwent RAI tend to be high. Thus, there is a need to measure TRAbs during pregnancy in women who undergo RAI before conception and to follow the fetus carefully for fetal hyperthyroidism and NH if TRAb values are still present during pregnancy.
The incidence of NH among newborns of mothers with GD who conceived after RAI therapy has not been previously reported. This study investigated the incidence of NH among newborns of mothers who conceived within two years after RAI therapy, and it attempted to identify predictors of NH.
Methods
The cases of 145 GD patients who conceived within two years after RAI therapy who and gave birth between April 1, 2004, and December 31, 2015, were retrospectively reviewed. Information regarding their newborns was also collected. The diagnosis of GD was based on the clinical findings, that is, the presence of a goiter and/or ophthalmopathy, elevated free triiodothyronine (fT3) and free thyroxine (fT4) levels, a suppressed thyrotropin (TSH) level, and a positive TRAb test. Every newborn was carefully followed in the hospital for at least five days after birth and was followed longer when necessary. The diagnosis of NH was made based on clinical symptoms and TSH and fT4 levels of cord blood samples or of blood sampled from the neonates within the first week after birth.
The overall incidence of NH was investigated. To investigate whether the incidence of NH becomes lower when the interval between RAI therapy and conception is longer, the incidence of NH was investigated among newborns of mothers who conceived within 6–12, 12–8, and 18–24 months after RAI therapy.
To identify predictors of NH, TRAb values were evaluated at the time of RAI therapy and during pregnancy. Information was also collected on each patient, including age at the time of RAI therapy, thyroid volume at the time of RAI therapy, radioiodine treatment activity, and days between RAI therapy and conception, in order to identify potential predictors of NH. Thyroid volume was evaluated by ultrasonography. This study was approved by the Ethics Committee of Ito Hospital, Tokyo, Japan.
Laboratory methods
TSH, fT3, and fT4 levels were measured by electrochemiluminescence immunoassays (ECLusys TSH, ECLusys fT3, and ECLusys fT4, respectively; Roche Diagnostics GmbH, Basel, Switzerland). The manufacturer's reference limits were: TSH 0.2–4.5 mIU/L, fT3 2.2–4.3 pg/mL, and fT4 0.8–1.6 ng/dL. The reference range for umbilical cord serum TSH was 0.09–18.0 mIU/L, and for fT4 it was 1.04–1.62 ng/dL. TRAb values were determined with an electrochemiluminescence immunoassay kit (ECLusys TRAb; Roche Diagnostics GmbH; reference value <2.0 IU/L).
Statistical analysis
Statistical analysis was performed with JMP v11.0 (SAS Institute, Inc., Cary, NC). Differences between the NH group and the non-NH group were analyzed by the Wilcoxon test. The data of the treatment of GD mothers in the first trimester of pregnancy and at delivery were statistically analyzed by using Fisher's exact test. p-Values of <0.05 were considered significant.
Multiple regression analyses (forward stepwise) were performed to identify possible predictors of NH. Receiver operating characteristic (ROC) curve analysis was performed to assess the optimal cutoff TRAb levels of GD mothers in the third trimester for predicting NH in newborns.
Results
Among the 145 GD patients, the median age at the time of RAI was 28 years (range 19–38 years), and the median thyroid volume was 48.8 mL (range 13.1–203.8 mL). There were eight newborns with NH, resulting in an incidence of 5.5%. Seven of eight mothers whose newborns had NH were treated for maternal hyperthyroidism during their pregnancy. Table 1 shows the characteristics of mothers whose newborns exhibited NH (NH group) and mothers whose newborns did not develop NH (non-NH group). The NH group had higher TRAb value
Characteristics of Mothers Whose Newborns Exhibited NH (NH Group) and of Mothers Whose Newborns Did Not Develop NH (non-NH Group)
NH, neonatal hyperthyroidism; RAI, radioactive iodine; TRAb, thyrotropin receptor antibody; NS, not significant.
Characteristics of the Eight Infants with NH
fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin; TSAb, thyroid-stimulating antibody.
Characteristics of the Eight Mothers of an Infant with NH
Table 4 shows the treatment of GD mothers in the first trimester of pregnancy, in the second and third trimesters of pregnancy, and at delivery, who conceived within 6–12 months, 12–18 months, and 18–24 months after RAI therapy. Treatment with ATD or KI was needed to control maternal hyperthyroidism in 54/145 (37%) patients. The GD patients who could not tolerate any ATDs were treated with KI throughout their pregnancy to control maternal hyperthyroidism. In order to avoid the use of methimazole (MMI) in the first trimester of pregnancy, KI was substituted for MMI in GD patients being treated with MMI who could not tolerate propylthiouracil (PTU) because of adverse effects. When a patient treated with KI remained hyperthyroid in the second trimester, MMI was added to KI, or MMI was substituted for KI. When a patient was being treated with KI and thyroid function was well controlled, the KI dose was continued or tapered. The percentage of GD patients treated with ATD at delivery was significantly lower among patients who conceived within 18–24 months after RAI therapy than it was in GD patients who conceived within 6–12 months after RAI (p < 0.05). The incidence of NH among the newborns of mothers who conceived within 6–12 months after RAI therapy was 8.8% (3/34; Fig. 1), 5.5% after 12–18 months (3/55; Fig. 2), and 3.6% after 18–24 months (2/56; Fig. 3). Although the incidence of NH among the newborns of mothers who conceived within 18–24 months tended to be lower than among mothers who conceived within 6–12 months, comparisons by means of Fisher's exact tests showed no statistically significant differences between any of the three groups.
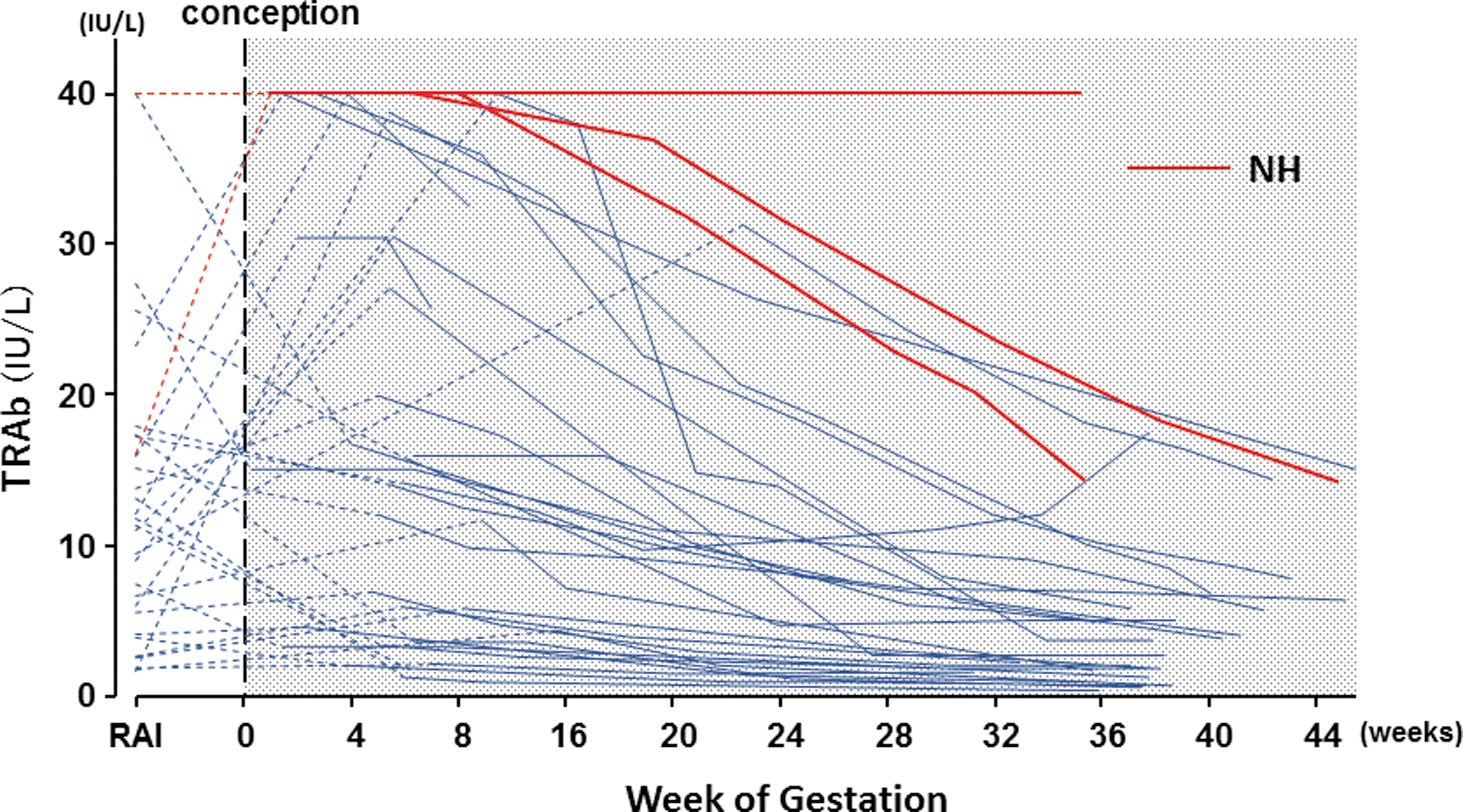
Thyrotropin receptor antibody (TRAb) value when radioactive iodine (RAI) therapy was performed and during pregnancy after conception within 6–12 months after RAI therapy in each patient. Incidence of neonatal hyperthyroidism (NH) was 8.8% (3/34). Solid lines are TRAb values in each patient during pregnancy, and dashed lines connect the TRAb value at RAI therapy and first TRAb value measurement in pregnancy. The red line shows the mother of neonate who presented with NH.
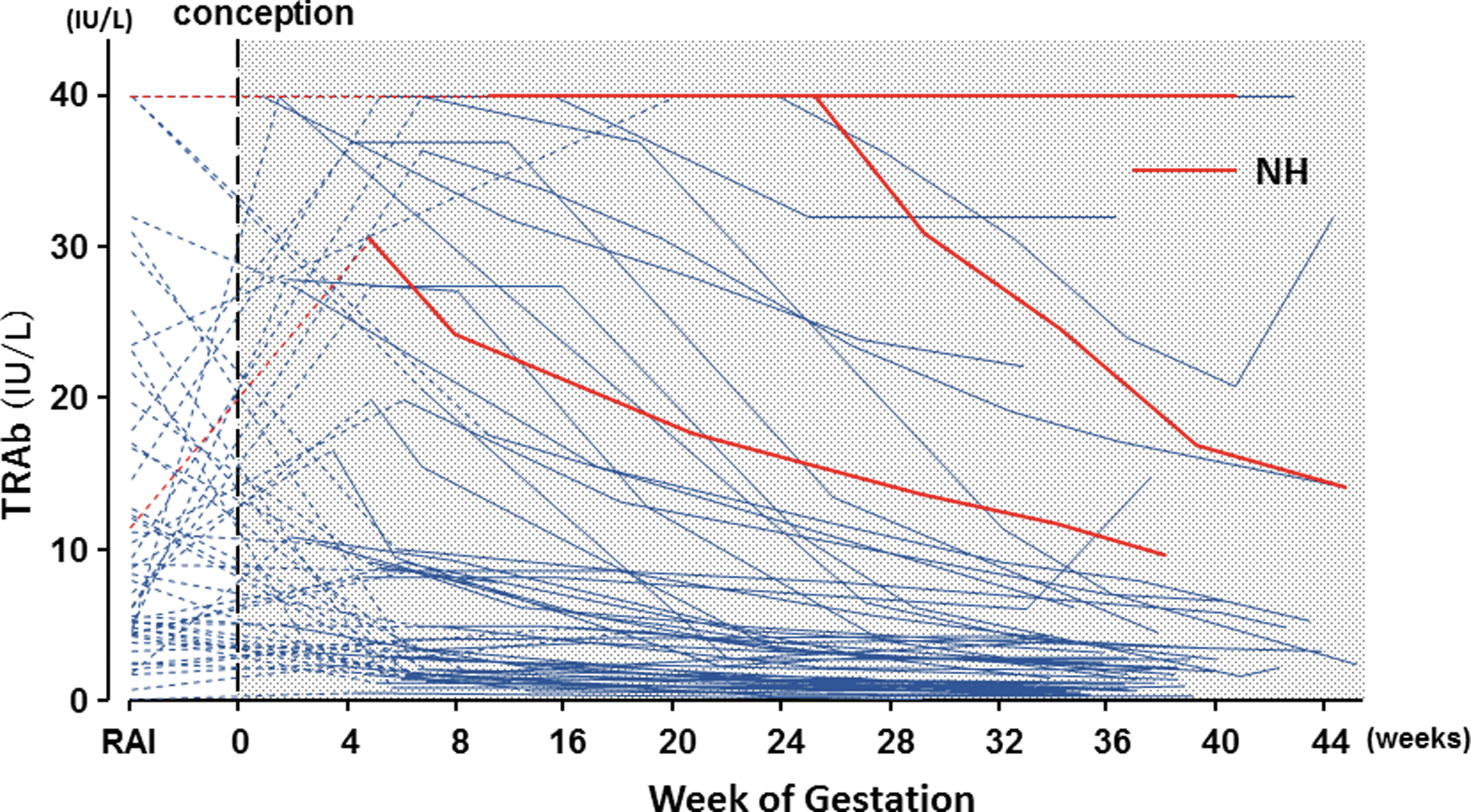
TRAb value when RAI therapy was performed and during pregnancy after conception within 12–18 months after RAI therapy in each patient. Incidence of NH was 5.5% (3/55).
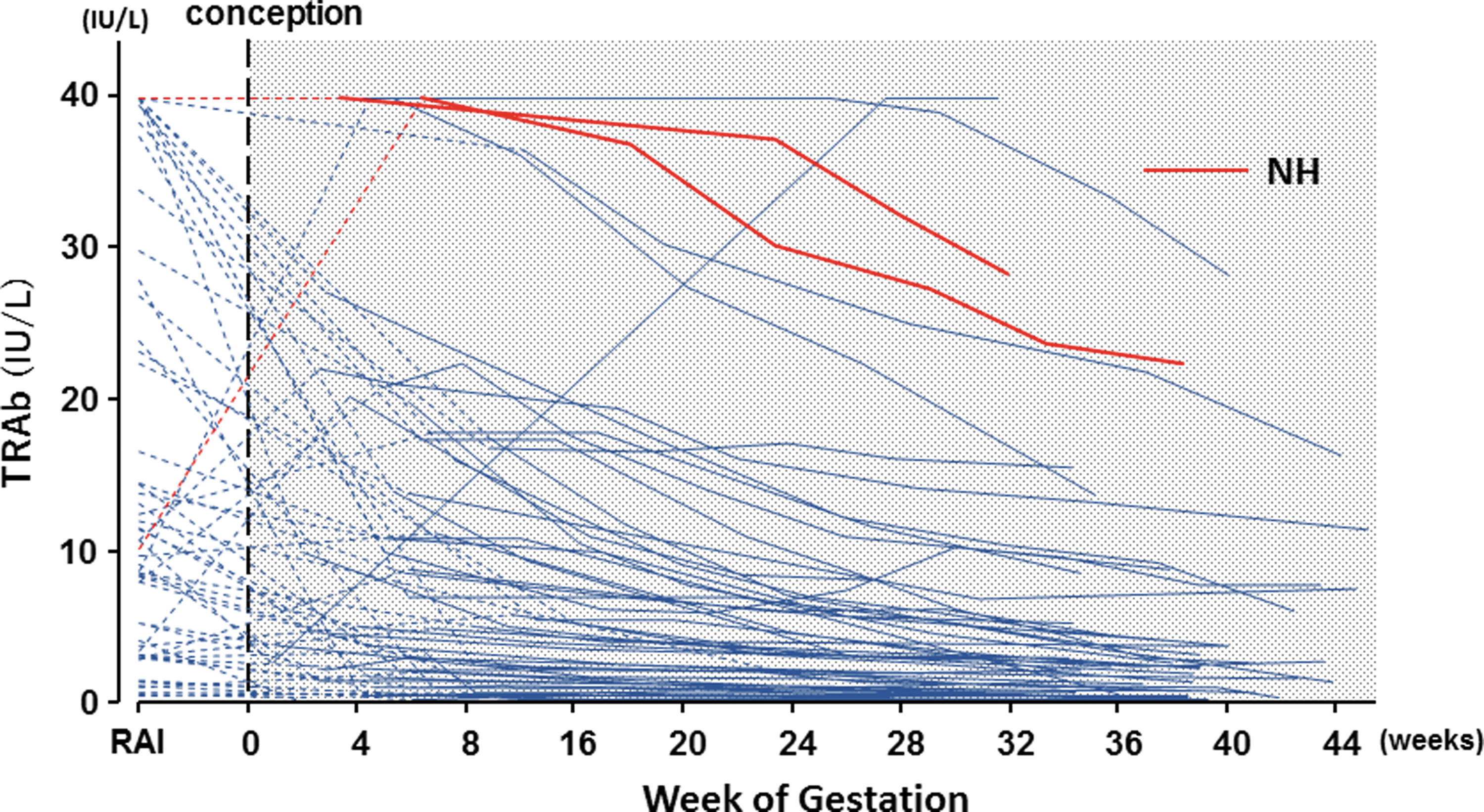
TRAb value when RAI therapy was performed and during pregnancy after conception within 18–24 months after RAI therapy in each patient. Incidence of NH was 3.6% (2/56).
Treatment of the GD Patients in the First Trimester of Pregnancy and at Delivery
The TRAb levels in the first trimester were negatively correlated with the number of days between RAI therapy and conception (p = 0.0011), but the correlation coefficient was low (r 2 = 0.065). There were no significant correlations between the TRAb values in the third trimester and the number of days between RAI therapy and conception.
Multivariate analysis revealed that the TRAb values in the third trimester were the only risk factor for NH. The ROC curve analysis showed that the cutoff TRAb value in the third trimester for predicting NH was 9.7 IU/L. A maternal TRAb value >9.7 IU/L in the third trimester predicted NH with 100% sensitivity and 88.3% specificity. The area under the ROC curve was 0.94 (Fig. 4). Based on these findings, an additional analysis was performed to develop a model to predict a TRAb level in the first trimester that would be expected to decline to <9.7 by the third trimester. The ROC curve analysis showed that the optimal cutoff TRAb value in the first trimester for predicting a TRAb value <9.7 IU/L in the third trimester was 28.0 IU/L. A maternal TRAb value <28.0 IU/L in the first trimester predicted a TRAb value <9.7 IU/L in the third trimester with 93% sensitivity and 76% specificity. The area under the ROC curve was 0.89.
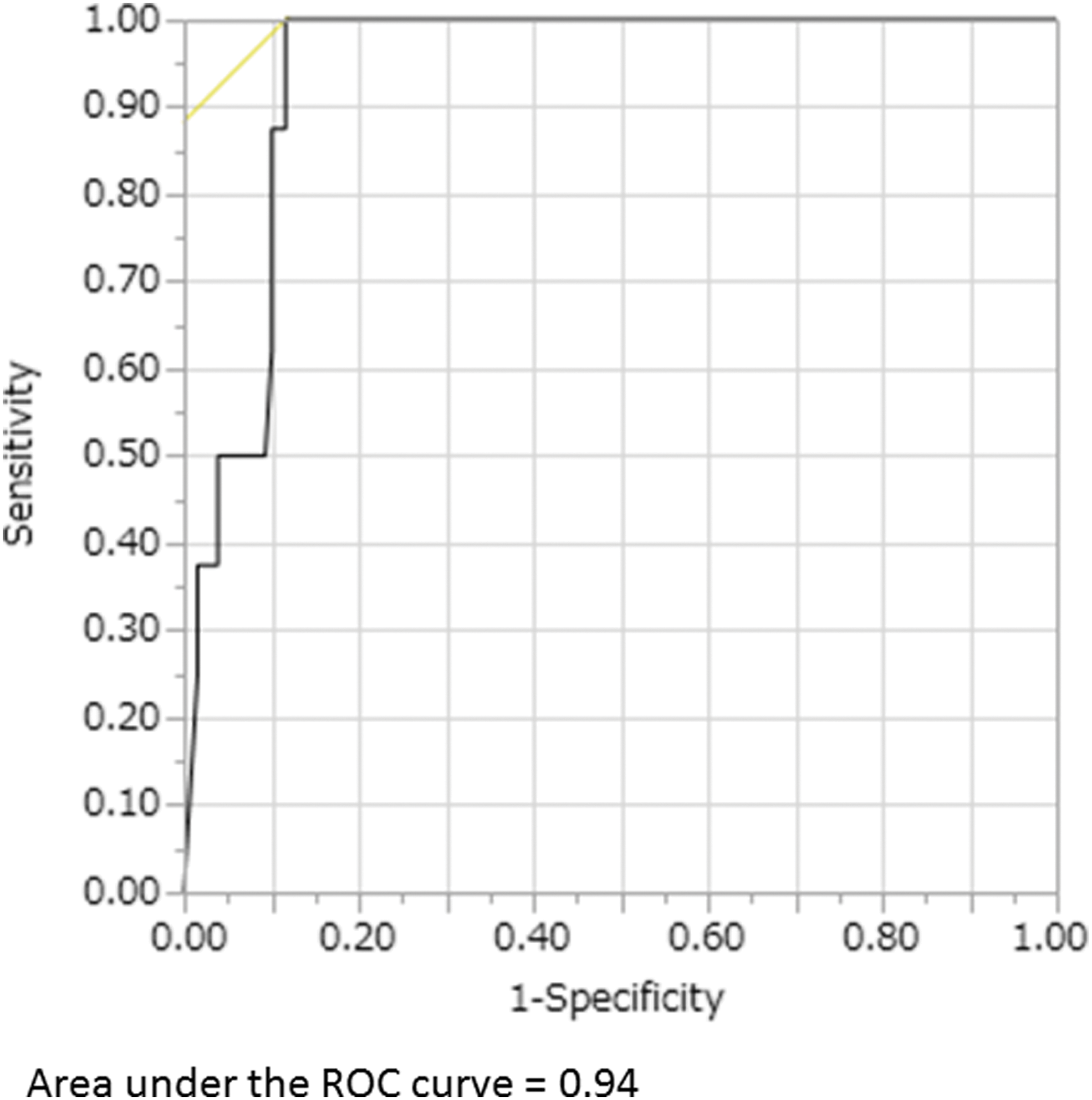
The receiver operating characteristic (ROC) curve analysis showed that the cutoff TRAb value in the third trimester for predicting NH was 9.7 IU/L. A maternal TRAb value >9.7 IU/L in the third trimester predicted NH with 100% sensitivity and 88.3% specificity.
Discussion
Treatment decisions for hyperthyroid women with GD who desire a future pregnancy are sometimes difficult. Therapeutic options for GD include ATDs, RAI therapy, and surgery. ATDs are associated with an increased rate of congenital malformations in newborns when they are used during the first trimester of pregnancy (12 –15). The relapse rate of hyperthyroidism is high among patients treated with ATDs compared to those treated with surgery or RAI (9). Moreover, ATDs can be associated with adverse reactions (16). Surgery can achieve a high rate of remission in patients with GD, but there are potential complications such as recurrent laryngeal nerve damage and hypoparathyroidism, and there is as subsequent need for lifelong substitution therapy with thyroid hormone. RAI therapy can also achieve a high rate of remission in patients with GD. However, in some patients, there are considerable increases in TRAb values after RAI therapy, usually with a peak at three months after treatment. In most patients, TRAb values then gradually decrease and return to pre-RAI therapy values after a year, but average values remain well above the normal reference range throughout a five-year follow-up after treatment (3). During pregnancy, TRAbs transfer to the fetus through the placenta and may stimulate the fetal thyroid gland and cause goiter and hyperthyroidism as early as 18 weeks of pregnancy (5 –10). The American Thyroid Association and the Endocrine Society recommend close follow-up of the fetus of mothers who previously received RAI therapy for GD and who have TRAb values more than two to three times the upper reference limit (17 –23). A recent systematic review reported that intensive fetal monitoring is recommended when maternal TRAb values are >3.7 times above the upper limit of normal (24). Careful follow-up of the fetus and the newborn is needed when high TRAb values are detected in mothers with GD in the second and third trimesters (25 –27).
TRAbs interact with the TSH receptor and they can exert a stimulating action (TSAb) or a blocking action (TSBAb), or they can be neutral (26,28 –30). TRAbs detected in hyperthyroid patients obviously have a predominantly stimulating action. TSBAbs are detected in a small percentage of GD patients who develop hypothyroidism (31). Fetal hypothyroidism sometimes develops when the TSBAb value of the mother is high during pregnancy (32,33). The TSBAb values of some GD patients who were not on ATD medication or who were on low-dose ATD medication during pregnancy have been reported to decrease (34) or to increase, but there were no dramatic changes in the thyroid function of any of the patients (35). It would be ideal to determine the bioactivity of TRAbs in GD patients after RAI therapy because the effect of maternal TRAb on the fetus cannot always be predicted on the basis of maternal thyroid function (36). Since TSAb bioassays were performed in only five patients and TSBAb bioassays in only two patients in this study, they were not included in the analysis. The TRAbs in the mothers with high TRAb values whose neonates did not develop NH may have had an overall neutral effect.
The incidence of NH among the newborns of mothers with GD who conceived after RAI therapy had not been previously reported. Based on the results of this study, the incidence of NH was 8.8% among the newborns of mothers with GD who conceived within 6–12 months after RAI, and 3.6% among those who conceived within 18–24 months. Multivariate analysis revealed that the TRAb values in the third trimester were the only risk factor for NH. The TRAb values in the first trimester were negatively correlated with the number of days between RAI therapy and conception, but the correlation disappeared for TRAb values in the third trimester and the number of days between RAI therapy and conception. It is difficult to predict the risk for NH at the time of RAI therapy. Based on the current data, the TRAb titer of pregnant women with a TRAb value <28 IU/L in the first trimester is likely to decline to <9.7 IU/L by the third trimester.
One of the limitations of this study is its retrospective nature, and some neonates who developed mild hyperthyroidism after discharge from the hospital may have been missed. However, all of the neonates in this study had been seen by a pediatrician at one month after birth, and none of them required additional treatment. Another limitation is that the number of subjects who conceived within two years after RAI therapy is small. The number of cases of NH may have been insufficient to reach statistical levels that would show that the incidence of NH is lower when conception occurred later after RAI.
Conclusion
The incidence of NH among newborns of mothers who conceived within 6–12 months after RAI was 8.8%, 5.5% within 12–18 months, and 3.6% within 18–24 months. The fetuses of pregnant GD patients whose TRAb value is ≥9.7 IU/L (reference value <2.0 IU/L) in the third trimester should be carefully followed by an obstetrician during pregnancy, and the newborns should be carefully followed by a pediatrician after birth.
Footnotes
Acknowledgments
We thank all the physicians, obstetricians, and pediatricians who contributed to this study. Portions of this manuscript were presented at the 87th Annual Meeting of the American Thyroid Association held in Victoria, Canada, in 2017.
Author Disclosure Statement
The authors report no conflicts of interest in this work.