
Abstract
Background:
The aims of this study were to determine a quantitative index, the initial ablation ratio (IAR), representing the amount of ablation, to predict therapeutic success and to evaluate the correlation between the IAR and volume reduction ratio (VRR).
Methods:
Among the patients who underwent radiofrequency ablation (RFA) for the treatment of benign thyroid nodules at the Withsim Clinic between April 2008 and December 2016, 130 patients with 134 nodules were included. The relationship between the IAR and VRR was analyzed at six months, 12 months, and the final follow-up. The relationship between the IAR and final VRR was also analyzed according to the initial nodule volumes.
Results:
The mean VRR was 78.7 ± 17.5% (range 23.3–100%) at a mean follow-up period of 22.6 ± 20.1 months (range 3–93 months). The mean IAR was 90.0 ± 11.6% (range 39.1–100%). The correlation coefficient between the IAR and final VRR was 0.65, which indicates a positive correlation (p < 0.001). When the IAR exceeded 70%, it tended to achieve 50% VRR in most cases.
Conclusions:
The IAR is a quantitative indicator of how well the RFA procedures are performed, and it is highly correlated with the VRR. If the IAR is >70%, VRR of >50% may be expected after RFA.
Introduction
R
Shortly after the first session of RFA, determining how much ablation has been performed is an important issue. In many previous studies, therapeutic success has been used as an indicator of successful RFA during the follow-up period (2,11,12). However, no index is available to predict the therapeutic success shortly after RFA. Such an index, if available, could serve as an indicator for the operators for management planning. Therefore, an initial ablation ratio (IAR) has been developed to assess how much ablation has been performed immediately after RFA. Using this IAR, the VRR can be predicted.
The purpose of this study was to determine the quantitative index IAR, which represents the amount of ablation, in order to predict therapeutic success and to evaluate the correlation between the IAR and VRR.
Methods
Patients
The national public Institutional Review Board designated by the Korean Ministry of Health and Welfare approved this retrospective study (P01–201802-21–004), and all patients provided written informed consent before undergoing RFA. Among the patients who underwent RFA for the treatment of benign thyroid nodules at the Withsim Clinic between April 2008 and December 2016, 188 patients with 195 nodules were included. The indications for RFA include patients with nodule-related cosmetic and/or compressive symptoms, such as foreign body sensation on swallowing, neck discomfort, or cough, and patients with nodules >2 cm in largest diameter that continue to grow (2). Of these subjects, 48 patients with 49 nodules having a final follow-up of less than six months were excluded from the study because of the lack of time to demonstrate the efficacy of RFA fully. Patients who underwent additional RFA within six months were also excluded for the same reason. Twelve nodules from 10 patients were excluded by this criterion. Finally, 134 nodules from 130 patients were included in the study (Fig. 1). The demographic data of the patients and nodules are summarized in Table 1.

Flow chart illustrating patient enrollment. RFA, radiofrequency ablation.
Preablation assessment and RFA procedure
The preablation assessment protocol suggested by the guidelines of the Korean Society of Thyroid Radiology was followed (2). Three orthogonal nodule diameters, including the largest diameter, were measured by ultrasonography, and nodule volume was calculated using the equation V = πabc/6, where V is the volume, a is the longest diameter, and b and c are the other two perpendicular diameters (2). All nodules were confirmed to be benign by analyzing at least two biopsy results. One radiologist (J.S.S.) with 15 years of ultrasound-guided biopsy and RFA experience performed RFA under the guidance of a high-resolution linear transducer by using RF generators (RF150 and RF 300; Apro-Korea, Gyeonggi, Korea) and 18-gauge straight-type, modified, internally cooled electrodes with active tip lengths of 5, 7, 10, and 15 mm (Well-Point RF Electrode; STARmed, Gyeonggi, Korea; CoATherm electrode, Apro-Korea). Local anesthesia, a transisthmic approach, and a moving-shot technique were used in all patients. After RFA, the patients were observed for four to six hours in the hospital in order to check for possible immediate complications (13 –16). A symptom score was estimated using a 10 cm visual analogue scale (grade 0–10). The cosmetic score was measured by a physician (1, no palpable mass; 2, no cosmetic problem but palpable mass; 3, a cosmetic problem on swallowing only; and 4, a readily detected cosmetic problem) (2).
Calculation of the IAR
After RFA, the total volume (V t) of the treated nodule is divided into centrally located ablated volume (V a) and peripherally located remaining viable volume (V v), as shown in Figure 2, resulting in the equation V v = V a + V v (17). V a is defined by using gray-scale changes compared to the initial nodule and disappearance of the Doppler signal, and it is calculated using a general volume calculation formula: V = π × w × d × l/6, where w is the width, d is the depth, and l is the length. However, in some cases, measuring the length was difficult because the margin of the ablated area was ill defined or irregular. In those cases, the closest approximation was measured to estimate the correct volume, and the mean value was used by repeating measurements more than twice. The presence of a color signal in the viable area was not constant, so the use of color Doppler was not very helpful in measuring V a. Contrast-enhanced ultrasonography, which has been widely used recently, is thought to help clarifying the boundary between the ablated and the viable area. However, it has not been used because it is not approved for use with the contrast agent that can be utilized for thyroid ultrasonography in Korea. For other factors, the suggestions by Choi et al. were followed as much as possible (18).

Follow-up ultrasound images acquired one month after RFA. (
The IAR is the ratio of the ablated volume (V a) to the total volume (V t) of the nodule immediately after RFA. For example, if the V t is 10 mL and the V a is 8 mL, the ablation ratio is 80%. However, the V t and V a cannot be measured immediately after RFA because of edema and hemorrhage. Therefore, the IAR was calculated by using the V a, which was calculated by subtracting the viable volume (V v) measured at the first follow-up from the V t at the time of RFA. Here, the V v is the volume of tissue remaining viable after RFA. The relationship of V a + V v = V t is established as described in the study by Sim et al. (17).
Calculating the final VRR and data analysis
The first follow-up was done between one and three months after RFA. After the first follow-up, the next follow-up was planned on the basis of the V t, V a, V v, and vascularity, usually three to six months later.
The final VRR was measured on the basis of the smallest volume of the nodule during the follow-up period. In the case of multiple sessions of RFA, it was measured on the basis of the smallest volume of the nodules before the second RFA.
The relationship between the IAR and VRR was analyzed at six months, 12 months, and final follow-up. The relationship between the IAR and final VRR was also analyzed according to the initial nodule volumes, and the cases that failed to reach therapeutic success are described. Pearson correlation analysis was used to evaluate the relationship between the IAR and VRR. All of the statistical analyses performed in this study were verified at a significance level of p < 0.001. Statistical analysis was performed using IBM SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY).
Results
The mean VRR was 78.7 ± 17.5% (range 23.3–100%) at a mean follow-up period of 22.6 ± 20.1 months (range 3–93 months). The mean IAR was 90.0 ± 11.6% (range 39.1–100%). The volume and VRR during the follow-up period are summarized in Table 2.
IAR, initial ablation ratio; VRR, volume reduction ratio.
Over time, approximately 70% reduction in volume occurred after six months, and a further 5% reduction occurred at 12 months. The time to reach the maximum volume reduction was 29.2 months in the small nodule group, 15.6 months in the intermediate group, and 11.9 months in the large group. The final VRR was 84.5% in the small nodule group, 74.1% in the intermediate group, and 67.9% in the large group. If the volume of the index nodule was small, the volume decreased for a longer period of time, and a higher VRR was obtained. If the volume was large, the volume reduction period was shorter, and the VRR was also lower.
The correlation coefficient between the IAR and final VRR was 0.65, indicating a positive correlation (p < 0.001). As shown in Figure 3, when the IAR exceeded 70%, it tended to achieve 50% VRR in most cases.
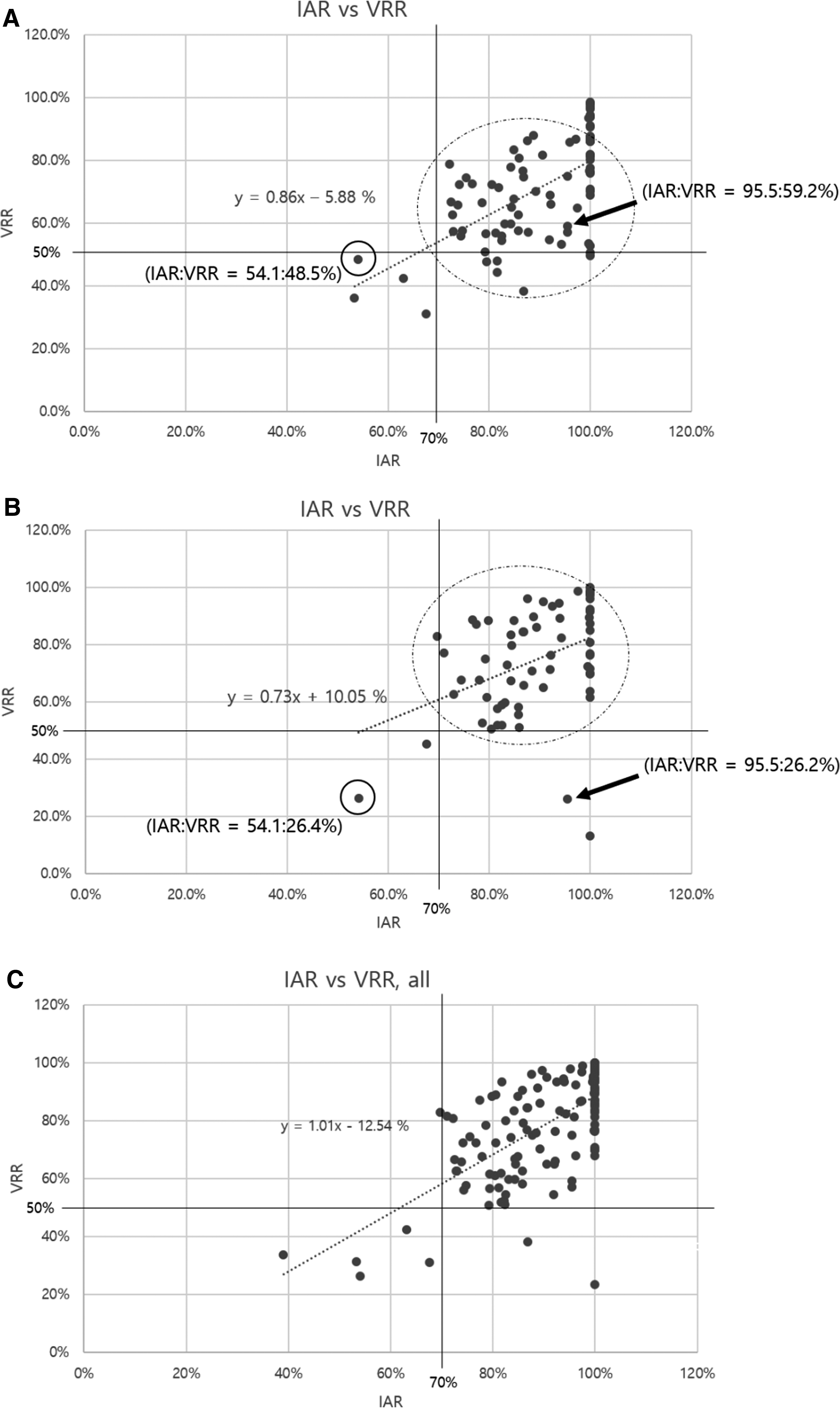
Relationship between initial ablation ratio (IAR) and volume reduction ratio (VRR) at (
Figure 3C, which shows the relationship between the VRR at the final follow-up and the IAR, shows that most of the dots gathered in the upper right corner. The line parallel to the x-axis represents 50% VRR. As described earlier, many researchers have used 50% VRR as a criterion for assessing therapeutic success. In other words, dots above the 50% line indicate cases that met the criteria of therapeutic success. These dots were all to the right of the line parallel to the y-axis. This line corresponds to 70% IAR. These results indicate that therapeutic success can be achieved if the IAR exceeds 70%. No case achieved therapeutic success with an IAR of <70%. However, there were cases wherein the VRR was <50% even though the IAR exceeded 70%. In conclusion, there was a tendency to achieve therapeutic success when the IAR exceeded 70%. Figure 3C shows seven cases of therapeutic failure. The clinical factors of them are summarized in Table 3.
Danger triangle: a triangle around the tracheoesophageal groove containing the recurrent laryngeal nerve. Intrathoracic extension: thyroid nodule extended to the inferior aspect of the clavicle or manubrium. Marginal regrowth: regrowth from the undertreated margin of the thyroid nodule. Slow volume reduction: a case in which the IAR was high, without marginal regrowth. The reason for therapeutic failure is the very slow speed of ablated tissue resorption.
Figure 2 shows the cases with high and low IARs. In case A, the index volume was 15.3 mL, and the IAR was 89%. This nodule showed a VRR of 83% at 13 months after RFA. In case B, the index volume was 45.7 mL, and the IAR was 48%. The VRR at three months was 31%. At six months after RFA, this nodule showed a so-called early sign of regrowth in which only the V v increased, while the V t did not increase (17,19). Therefore, additional ablation was performed later.
Symptom and cosmetic scores were improved after RFA, from 2.6 to 0.7 and from 2.2 to 1.4, respectively.
Discussion
This study demonstrates that the IAR shows a positive correlation with the final VRR (p < 0.001). When the IAR was >70%, it tended to achieve 50% VRR. Therefore, the IAR can be a quantitative index to predict therapeutic success after RFA of benign thyroid nodules. Moreover, the VRR is related to the index nodule size. The final VRR was 84.5% in the small group, 74.1% in the intermediate group, and 67.9% in the large group. Considering these results, they are helpful for the planning of additional RFA sessions and/or the follow-up interval according to the IAR and index nodule size.
Therapeutic success, that is, treatment outcome after RFA, has been used as an index to predict the improvement in a patient's symptoms and cosmetic problems after RFA (2,20). Moreover, an insufficient amount of ablation can cause early marginal regrowth during the follow-up period (21). Therefore, short-term follow-up or immediate repeat RFA is recommended in such cases. To determine the follow-up period or the need for repeat RFA, the IAR will be useful to operators.
The relationship between the index nodule size and VRR is well known. Lim et al. reported that the larger the volume of the index nodule, the more sessions of RFA were required to achieve sufficient volume reduction (3). In factor analysis of the efficacy of thermal ablation, the index nodule size is one of the important factors (19,21). In a single-session laser ablation of large thyroid nodules, the reported recurrence rate (by the definition of an increase in nodule volume over initial volume) was 9% (22). When treating large nodules, the VRR is low, and regrowth occurs more frequently. Therefore, if the initial volume is large and/or if the IAR is <70%, the nodule is likely to regrow. Hence, it is better to plan the additional RFA promptly. These findings were similar to those in the current cases. As summarized in Table 2, the small nodules reached a VRR of 84.9% over 29.2 months, while the large nodules reached a VRR of 67.9% over 11.9 months.
An additional session of RFA is needed if marginal regrowth is seen. In some studies, thermal ablation results did not reach an average of 50% VRR (22,23). It is suggested tjat the reason is that the IAR had not reached 70% because of device limitations or technical factors (24). Recently, the results of RFA of papillary thyroid microcarcinomas or small follicular neoplasms have been reported (25,26). In these cases, it is more important to treat the margin completely. The low IAR indicates the presence of a lot of marginal viable tissue around the central ablated tissue (15,17,27). However, although leaving a large margin is safe from the perspective of complications, leaving too much margin may lead to therapeutic failure. Hence, subjecting the margin to additional treatment is very important. According to the study by Huh et al. using a moving-shot technique, a group with additional treatment achieved a higher VRR than did a group with a single-session RFA (20). In contrast, in a study of multiple-session treatment with laser ablation, use of multiple sessions did not significantly increase the VRR (28). It is assumed that this difference is due to the placement of the thermal energy source. The method of moving the energy source seems to be advantageous in maximizing the ablation zone. In contrast, placing the energy source at the center of the tumor makes it difficult to cover the margin.
Seven nodules failed to achieve therapeutic success in the present study. The reasons were intrathoracic extension, proximity to the danger triangle (21,29), slow volume reduction, and marginal regrowth. Case 3 showed therapeutic success after one additional RFA. Other cases showed symptomatic improvement, even though the VRR was not high. These cases showed no evidence of regrowth, and hence they were followed up without further RFA. These results suggest that exophytically growing nodules (direction of the upper pole or lower pole of the thyroid gland) are often in close proximity to the danger structures, making it difficult to complete ablation. This should be fully explained to patients before performing RFA (30).
Regarding the final goal of RFA of benign thyroid nodules, there are several proposals. In the 2000s, when thermal ablation was first introduced, it was mainly aimed at solving pressure symptoms and cosmetic problems, based on an approximately one-year follow-up (2,4,31 –33). However, after the long-term follow-up results of RFA were published, regrowth was reported after two years (3,22). Regrowth usually occurs in viable tumor tissue that remains in the margin (17). Therefore, several recent studies have suggested complete ablation to prevent marginal regrowth (17,34). Two meaningful long-term follow-up studies have been published. Lim et al. performed a follow-up for four years with a maximum of seven RFA sessions, resulting in a regrowth rate of 5.6% (3). Sim et al. followed up patients for up to seven years after a single-session RFA, with a regrowth rate of 24.1% (17). These findings suggest that long-term stability with symptom improvement can be a realistic goal of RFA treatment. To achieve this goal in nodules not showing regrowth, follow-up without additional RFA will be sufficient. In contrast, for nodules showing regrowth, performing additional ablation aimed at complete ablation is necessary.
Limitations of this study
The first limitation of this study is its retrospective design and irregular follow-up interval. The second limitation is the technical difficulty of measuring the V a. Therefore, the proposal of nodule volume measurement by Choi et al. was followed to minimize the measurement error (35).
Conclusions
The IAR is a quantitative indicator of how well RFA procedures are performed, and it is highly correlated with the VRR. If the IAR is >70%, >50% of VRR, therapeutic success may be expected. By considering the volume of the index nodule and the IAR, repeat RFA can be planned, and the follow-up interval can be determined more systematically.
Footnotes
Author Disclosure Statement
This study received no funding in the form of grants. J.H.B. is the patent holder of the unidirectional ablation electrode. The other authors have no potential conflicts of interest to disclose.