
Abstract
Background:
Thyroglobulin (Tg) is an established tumor marker in differentiated thyroid carcinoma (DTC). However, Tg assays can be subject to interference by autoantibodies against Tg (TgAbs). No clinical consensus exists on the cutoff value of TgAb positivity and its relationship to Tg assay interference. The aims of this study were to investigate the most applicable cutoff value for TgAb positivity in clinical practice and to evaluate whether tumor characteristics differ between TgAb+ and TgAb− patients during ablation therapy using the manufacturer's cutoff (MCO) and institutional cutoff (ICO).
Methods:
This single-center cohort study included 230 DTC patients diagnosed between January 2006 and December 2014. Serum Tg and TgAbs were measured with the Tg-IRMA (Thermo Fisher Scientific) and ARCHITECT Anti-Tg (Abbott Laboratories) assays. Patients were divided into TgAb− and TgAb+ based on the limit of detection (LoD; ≥0.07 IU/mL), functional sensitivity (FS; ≥0.31 IU/mL), MCO (≥4.11 IU/mL), and ICO (≥10 IU/mL).
Results:
All patients were TgAb+ based on the LoD; one patient was negative on FS. Fifty-five (23.9%) and 34 (14.8%) patients had TgAbs above the MCO and ICO, respectively. Histology, presence of multifocality, tumor-node-metastasis, and American Thyroid Assocation risk stratification did not differ between TgAb− and TgAb+ patients using MCO and ICO during ablation.
Conclusions:
This study supports the use of a higher cutoff value than that of the FS for TgAb positivity in clinical settings. The LoD and FS are too sensitive to discriminate TgAb positivity and negativity in DTC patients during ablation therapy. The presence of TgAbs during ablation is not related to tumor characteristics and risk profile. This implies that TgAb positivity should not be considered a separate risk factor.
Introduction
Thyroglobulin (Tg) is the established tumor marker during follow-up of patients with differentiated thyroid cancer (DTC) (1 –3). For Tg measurement, a highly reliable Tg assay is crucial. However, Tg assays can be subject to interference by Tg antibodies (TgAbs), which can result in false-negative (e.g., undetectable) or false-positive Tg values, depending on the assay (4 –7). In 18–29% of DTC patients, TgAb values are detectable, the number depending on the cutoff value that is used (8 –11). Because no Tg immunoassay is completely free from interferences, TgAb analysis should be performed parallel to each Tg measurement (4,5). Until now, there is no clinical consensus on the definition of TgAb positivity and its relation to Tg assay interference. The literature proposes several cutoff values for TgAb positivity. The first is the limit of detection (LoD), based on the argument that even very low TgAb values can interfere with the Tg assay (12,13). Second, the limit of quantification (LoQ) has been recommended, since this provides more certainty about the validity of the measured TgAb concentration and the possibility of a potential relevant interference in the patient (5). Some prefer to use functional sensitivity (FS) instead of the LoQ because it is determined over a long clinical time span (6–12 months) (14,15). A third possibility for a cutoff value is the use of the manufacturer's cutoff (MCO). However, as the MCO has often been determined for use in diagnosing patients with thyroid autoimmunity, it is therefore considered to be unsuitable for detecting TgAb interference (5,13). Finally, every reagent manufacturer states in its package insert instructions that each laboratory should establish its own specific TgAb assay reference value for its own patient population (institutional cutoff [ICO]). These different approaches, leading to varying TgAb cutoff values, have contributed to uncertainty regarding the definition of TgAb positivity and consequently to uncertainty regarding the disease status of DTC patients with measured TgAbs (4,5,16). In addition to the discussion about the cutoff value of TgAbs, there is growing evidence for the value of trends in serum TgAb levels and disease activity (9,17,18).
The presence of TgAbs during initial treatment has unequivocal consequences for initial risk stratification and follow-up strategies, depending on the guidelines used. The European Thyroid Association recommends periodic neck ultrasound and 131I scans to monitor TgAb+ Tg undetectable patients (19). The Dutch DTC guideline considers patients with detectable TgAb before/during ablation therapy as intermediate/high risk, as Tg cannot be considered a reliable tumor marker (20). The American Thyroid Association (ATA) and the British Thyroid Association DTC guidelines do not include the presence of TgAbs in their initial risk stratification, but rather they emphasize the value of trends in the TgAb levels in relation to disease activity (21,22). Likewise, the American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) tumor-node-metastasis (TNM) system, used to predict mortality, does not take into account TgAb, but merely focuses on tumor size and lymph node and distant metastases (23).
Therefore, the first aims of this study were to investigate which cutoff value for TgAb positivity is the most applicable for clinical practice, and to evaluate whether tumor characteristics differ between TgAb+ and TgAb− patients during ablation therapy, using different cutoff values. The next aim was to evaluate the value of TgAbs as a risk factor in a low-risk patient group according to the Dutch DTC guidelines.
Methods
Study design and population
In this single-center cohort study, all consecutive patients who were diagnosed with DTC between January 1, 2006, and December 31, 2014, and who received their treatment and/or follow-up at the University Medical Center Groningen (UMCG) were identified from the DTC database in which patients are included prospectively. Patients were treated according to the Dutch DTC guidelines (20). In general, the initial procedure consisted of a (near) total thyroidectomy with or without additional lymph node dissection. After surgery, the patients received 131I ablation therapy after thyroid hormone withdrawal (THW) or recombinant human thyrotropin (rhTSH) upon clinical indication.
Data collection
The patients' medical data were obtained through the database and from their electronic medical records using the hospital information system. According to the Dutch Medical Research Involving Human Subjects Act, no separate approval was needed. Analyses were performed on fully anonymized data sets.
Study definitions
DTC was defined as papillary and follicular thyroid carcinoma (including all subtypes). The date of diagnosis was defined as the date of histological confirmation of DTC. Histological diagnosis, TNM classification, and thyroiditis were confirmed by the pathology department of the UMCG. The original histology of all patients referred to the thyroid cancer center after being operated in another hospital were revised by two experienced pathologists.
Tumors were staged and reclassified according to the seventh edition of the AJCC/UICC TNM system for DTC (23). Hashimoto's thyroiditis (HT) was defined as the presence of a diffuse lymphocytic infiltration in the thyroid gland combined with (i) germinal center formation, (ii) thyroid follicle obliteration, and (iii) epithelium destruction. In some pathological reports, a diffuse lymphocytic infiltration was only mentioned with one or two additional characteristics; these cases were also defined as HT. All the other descriptions of thyroiditis were not considered to be HT. The duration of follow-up was calculated in years from the date of diagnosis until March 1, 2016.
The initial Tg and TgAb levels were determined during THW or after rhTSH stimulation, shortly before the 131I ablation therapy.
To monitor TgAb trends and disease state, the change of TgAbs during follow-up was compared to the disease state after the change. Changes in TgAbs (based on the ICO) were defined as no TgAbs present, TgAbs switch negative to positive, TgAbs switch positive to negative, TgAbs increase ≥50% of a positive value, stable positive value (<50% change), and TgAbs decrease ≥50% of a positive value.
Disease state was classified as in remission, persistent, or recurrent disease. Remission was defined as absence of clinical, scintigraphic, and/or radiological evidence of disease and Tg <1.0 ng/mL during TSH suppressive therapy for at least one year after the initial 131I therapy. Persistent disease was defined as presence of disease, radiologically and/or biochemically proven (Tg ≥1.0 ng/mL under TSH suppressive therapy) within one year after the initial 131I therapy. Recurrent disease was defined as presence of disease, radiologically and/or biochemically proven (Tg ≥1.0 ng/mL under TSH suppressive therapy), after remission following the initial 131I therapy.
The cumulative administrative 131I dose was calculated using the administered ablation and subsequent therapeutic dosages.
Laboratory measurements and definitions
The lower LoD of the assay is defined as the value corresponding to a signal 2 standard deviations (SD) above the mean of 10 replicates of the zero calibrator. FS is the level of the analyte at which the assay is able to reproduce the results with an interassay coefficient of variation of 20% over a 6- to 12-month time span. The Tg immunoradiometric assay (Tg-IRMA) by Thermo Fisher Scientific (Henningsdorf, Germany) was used for the detection of Tg. This assay is calibrated indirectly against the Certified Reference Material (CRM) 457 standard by using an adjustment factor. However, since there is some discussion concerning the exact value of the adjustment factor as stated in the kit insert, this study used the uncorrected results of the Tg assay (24). The Tg-IRMA has a LoD of 0.1 ng/mL and FS of 0.3 ng/mL. Tg-IRMA levels <0.1 ng/mL were defined as analytically undetectable. TgAbs were determined with a chemoluminescence immunoassay (ARCHITECT Anti-Tg assay; Abbott Laboratories, Chicago, IL). This assay is calibrated against the World Health Organization 1st International Reference Preparation (IRP) 65/093. The LoD and FS of this assay are 0.07 IU/mL and 0.31 IU/mL, respectively, and the MCO is 4.11 IU/mL. The ICO of this assay is ≥10 IU/mL, determined by the authors' own laboratory by remeasuring sera of 120 controls free of thyroid disease. Subject selection of these controls was performed according to guideline 33 of the National Academy of Clinical Biochemistry guidelines, with the adaptation that the controls consisted of both men and women (25). Between 2006 and 2014, two TgAb assays were used: the ARCHITECT Anti-Tg assay and the Brahms anti-Tg assay (Thermo Fisher Scientific). However, the use of the anti-Tg assay from Brahms turned out to have no added value, which resulted, since 2014, in the use of only the ARCHITECT Anti-Tg assay (unpublished data).
Risk stratification
The study population was classified according to the seventh edition of the AJCC/UICC TNM system (23), the initial ATA classification (2015) (21), and the Dutch DTC risk stratification (2014) (20). In short, according to the Dutch DTC risk stratification, low-risk patients were defined as those with a T1 or T2 minimal invasive follicular, or a classic papillary carcinoma with N0 or N1a (level VI) lymph node involvement without extranodal extension, detectable Tg with negative TgAbs shortly before surgery or during ablation therapy, and no radioiodine uptake outside the thyroid bed on the post-ablation scan. Patients not meeting low-risk criteria were classified as intermediate or high risk (20).
Study method
For the first aim, the study population was divided into TgAb− and TgAb+ patients based on cutoff levels according to LoD (≥0.07 IU/mL), FS (≥0.31 IU/mL), MCO (≥4.11 IU/mL), and ICO (≥10 IU/mL). Furthermore, each patient was classified according to the AJCC/UICC TNM system and the initial ATA and Dutch DTC risk-stratification criteria. Following the first aim, the study evaluated whether tumor characteristics differed between TgAb+ and TgAb− patients during ablation therapy using the different cutoff levels mentioned above. The second aim of the study was to evaluate the patients with low-risk histopathological tumor characteristics according to the Dutch guidelines, and to subclassify them as TgAb+ or TgAb−.
Statistical analysis
Normally distributed data are expressed as the mean ± SD, and nonparametric distributed data as the median with interquartile range (IQR). For comparison of normally distributed data, Student's t-test was performed. Nonparametric continuous data were compared using the Mann–Whitney U-test. Categorical data were compared using Pearson's chi-square test or Fisher's exact test. p-Values <0.05 were considered significant. IBM SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY) was used for statistical analysis of the data.
Results
General patient characteristics
The study population consisted of 230 patients. Of these, 155 (67%) were female, and 180 (78%) were diagnosed with papillary thyroid carcinoma (PTC). The mean age at diagnosis was 48 ± 18 years, and the median follow-up was 6 years (IQR 2–8 years). The characteristics of the study population are summarized in Table 1.
Characteristics of TgAb− and TgAb+ Patients (TgAbs+ ≥4.11 IU/mL and ≥10 IU/mL)
Data shown are median (IQR) or n (%). Serum Tg and TgAbs measured during THW shortly before 131I ablation therapy; TgAb levels ≥4.11 IU/mL (MCO) and ≥10.0 IU/mL (ICO) were considered positive.
p < 0.001, TgAbs <4.11 vs. ≥4.11 IU/mL and TgAbs <10.0 vs. ≥10 IU/mL.
p = 0.003, TgAbs <4.11 vs. ≥4.11 IU/mL and TgAbs <10.0 vs. ≥10 IU/mL.
TgAb, thyroglobulin autoantibodies; MCO, manufacturer's cutoff; ICO, institutional cutoff; TNM, tumor-node-metastasis; AJCC, American Joint Committee on Cancer; ATA, American Thyroid Association; IQR, interquartile range; THW, thyroid hormone withdrawal.
Patient characteristics according to different TgAb cutoff levels during ablation therapy
Applying the LoD (0.07 IU/mL) as the cutoff value for TgAb positivity, all 230 patients would be classified as TgAb+. Therefore, no comparison could be made for tumor characteristics using this cutoff value. The same was true for FS (0.31 IU/mL), as 229 patients would be considered to be TgAb+. One female patient had a TgAb value <0.31 IU/mL during ablation therapy. She was diagnosed with a T2N1aM0 PTC at 37 years of age, and during follow-up she was clinically in remission with stable TgAb levels around 0.5 IU/mL. Out of 230 patients, 55 (23.9%) had TgAbs above the MCO of 4.11 IU/mL, and 34 (14.8%) had a TgAb value above the cutoff value of 10 IU/mL. Table 1 shows the clinical characteristics of TgAb− and TgAb+ patients using the MCO and ICO. There were no differences in sex, age at diagnosis, presence of multifocality, TNM, ATA risk stratification, or disease state after initial treatment. The median cumulative administrative 131I dose was significantly higher in the TgAb+ group compared to the TgAb− group when using both the MCO (11.1 GBq [11.1–16.7 GBq] and 11.1 GBq [5.6–11.1 GBq]; p = 0.001) and the ICO (11.1 GBq [11.1–15.3 GBq] and 11.1 GBq [5.6–11.1 GBq]; p = 0.003). Using the MCO and ICO as the cutoff value, HT was significantly more present in TgAb+ patients compared to TgAb− patients: 26 (47.3%) and 10 (5.7%), respectively, using the MCO (p < 0.001) and 18 (52.9%) and 18 (9.2%), respectively, using the ICO cutoff (p < 0.001). The median Tg value of the TgAb+ patients was significantly lower compared to the Tg value in the TgAb− group (MCO: 1.0 ng/mL [0.1–5.7 ng/mL] and 3.7 ng/mL [1.3–16.0 ng/mL], p < 0.001; ICO: 0.5 ng/mL [0.1–2.9 ng/mL] and 3.7 ng/mL [1.2–16.0 ng/mL], p < 0.001). The percentage of patients with undetectable Tg was significant higher in the TgAb+ group compared to the percentage in the TgAb− group (MCO: 25.5% and 9.7%, p < 0.003; ICO: 38.2% and 9.2%, p < 0.001).
Trends in TgAbs and disease activity
Persistent/recurrent disease was observed in five out of six patients after the TgAb conversion from negative to positive and in two out of three patients with an increase of ≥50% of a positive value. Remission was observed in six out of six patients after the TgAb conversion from positive to negative, and in 21/24 patients with a decrease of ≥50% of a positive TgAb value (Table 2; p = 0.008).
Trends in TgAbs Based on the ICO and Disease Activity
191 patients were TgAb− upon diagnosis and did not become positive during follow-up.
p = 0.008.
Dutch DTC risk stratification
Out of the cohort of 230 patients, 192 were classified as high risk according to the Dutch risk-stratification criteria. Focusing on these 192 patients, 186 were classified as high risk based on tumor characteristics with or without a TgAb values above the ICO of 10 IU/mL. The remaining six patients were classified as high risk, not due to tumor characteristics but due to TgAb levels above the ICO of 10 IU/mL. Thirty-eight patients were classified as low risk based on their tumor characteristics and the TgAb values. Table 3 shows the characteristics, treatment, and outcomes of the 44 patients classified as low risk solely based on tumor characteristics. During follow-up, all six patients with initial TgAb positivity were in remission with declining TgAb levels (Fig. 1). Of the remaining 38 low-risk patients, 89.5% were in remission one year after initial therapy; four patients showed persistent disease.
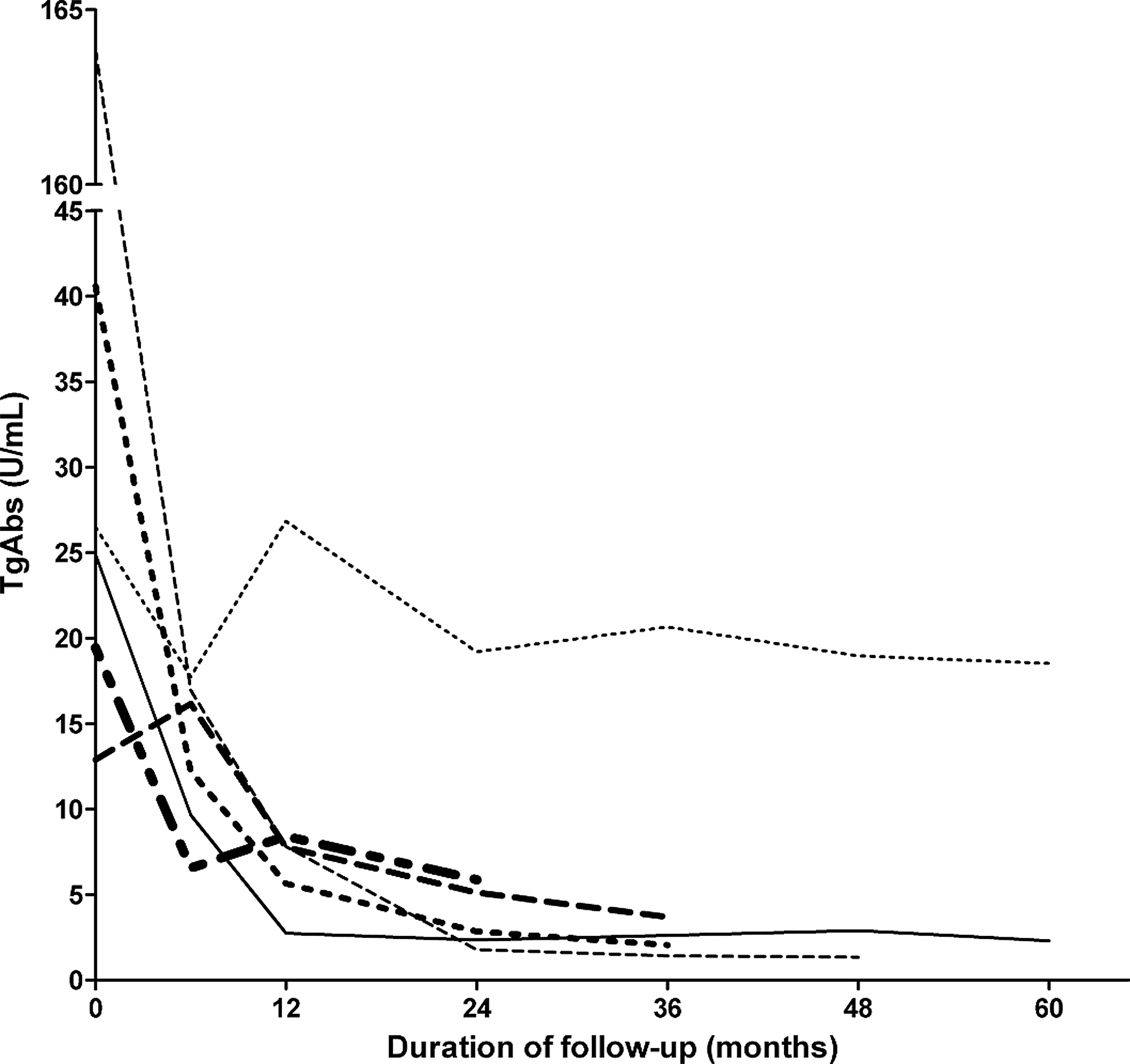
Changes in thyroglobulin autoantibody (TgAb) levels during follow-up of six patients classified as intermediate/high risk based on TgAbs.
Differences in Characteristics of Low-Risk Patients Classified According to Tumor Characteristics and TgAb Value
Data shown are median (IQR) or n (%). Serum Tg and TgAbs measured during THW shortly before 131I ablation therapy; patients with TgAb levels ≥10 IU/mL were considered intermediate/high risk. TgAb trends based on initial TgAb value and TgAb value after two years of diagnosis.
Discussion
This study demonstrates that as cutoff levels to define TgAb positivity in DTC patients during ablation therapy, the LoD and FS are not useful in clinical practice because they render Tg useless as a tumor marker, since almost all patients had TgAbs above these cutoff values. Using the MCO or ICO as a cutoff value for these patients is more reasonable in clinical practice. In this study, based on the MCO or ICO, the TgAb+ patients showed no differences in tumor characteristics and risk profiles compared to the TgAb− patients. This implies that TgAb positivity should not be considered a separate risk factor.
Latrofa et al. illustrated that low levels of TgAb can interfere with the Tg assay but that metastatic disease can be ruled out when TgAb levels are below the MCO and Tg is not detectable (26). They nicely illustrated the difference between analytical and clinical relevance regarding the interference of low TgAbs with the Tg assay. The study by Côrtes et al. demonstrated that low- or intermediate-risk patients with borderline TgAbs (TgAb values between FS and MCO), undetectable Tg, and normal ultrasound after initial treatment are not at a greater risk for tumor persistence or recurrence compared to patients with undetectable TgAbs (27). The present study shows that using the MCO or ICO, TgAb+ patients have significantly lower Tg values. This may, however, reflect an analytical interference that may not be of relevance in clinical decision making, as suggested by Latrofa et al. and Côrtes et al. (26,27).
Furthermore, as suggested in the recent literature, with the increasing availability and development of high-sensitive Tg assays and Tg quantification with liquid chromatography tandem mass spectrometry, Tg may be more reliably monitored even in the presence of TgAbs (28,29).
Related to this subject is the clinically relevant issue of whether TgAb positivity, using the MCO or ICO, led to a negative Tg measurement in the presence of structural disease. In the patient data, it was not found that the presence of TgAbs, based on the MCO and ICO, prevents or delays the detection of persistent or recurrent disease (data available on request). The TgAb+ patients with a concomitant Tg <1.0 ng/mL showed no structural disease, defined as lymph node or distant metastases revealed by ultrasound and 131I whole-body scans.
The relevance of detectable TgAbs during ablation therapy and their effect on the risk status of DTC patients has been a point of controversy in some guidelines and earlier studies (9 –11,30 –33). The present study demonstrates that patients with TgAbs during ablation therapy do not differ with regard to tumor characteristics and risk profile, and the data do not support their use as a separate risk factor. These findings are not in line with the study by Durante et al. in which 220 TgAb+ PTC patients were compared to a control group of 1020 TgAb− PTC patients. They concluded that TgAb+ patients differed concerning tumor characteristics and long-term clinical outcomes. At baseline, TgAb+ patients more often had extrathyroidal extension and were more frequently classified as high risk according to the ATA risk classification (32). However, this was a multicenter study with a heterogeneous patient population in which TgAb positivity was established after a range of 1–12 months after initial treatment, that is, (near)total thyroidectomy plus cervical lymph node dissection and/or radioiodine ablation. Furthermore, TgAb positivity was defined without specific details as to the assays and cutoff values used. Trimboli et al. found that positive TgAbs prior to 131I ablation therapy indicated a higher risk of poor prognosis (33). This is in contrast to the disease outcome in the present study, in which TgAb+ patients received more 131I as a result of national guidelines. This could possibly explain the equal disease outcomes in the TgAb+ and TgAb− patients. For this reason, conclusions regarding disease outcome could not be made in this study group.
As expected, HT was significantly more frequent in TgAb+ patients. Other studies also report a higher prevalence of HT in TgAb+ patients, which probably reflects the autoimmune process associated with HT (9,17). The prevalence of HT in DTC varies from 0.5% to 30%, depending, among other factors, on the population studied and the definition of HT (13,30,34 –39). The causal pathway between HT and DTC and the prognostic value of the presence of lymphocytic thyroiditis remain elusive (13).
Several DTC guidelines and original articles emphasize the use of TgAb levels as surrogate tumor markers. TgAbs appear to change in response to changes in the mass of Tg-secreting tissue, trends that could help to provide more certainty regarding the disease status (6,13,19 –22,40). Therefore, Tg and TgAbs always have to be measured concomitantly in all patients, and clinical decision making depends on the levels of these markers. Despite limited numbers, the results support the statement that TgAb trends are, over time, markers of disease activity. When comparing the change in TgAbs during follow-up with the disease state after the change, it was found that patients with an increase of TgAb were found to have persistent/recurrent disease and patients with decreasing TgAb values were in remission.
The six patients classified as high risk according to the national guidelines, with TgAb levels above the ICO but with low-risk tumor characteristics, showed all declining values during the two years of follow-up. These results also suggest that in low-risk patients with TgAbs, decreasing TgAb trends can be used to support less aggressive treatment.
This study has strengths and limitations. The data were taken from a homogenous patient group from a single institution using one Tg and TgAb assay during a long period of follow-up. Differences between TgAb assays are generally known. However, the main message of our study is the importance of the definition of TgAb positivity (i.e., the cutoff value of the TgAb assay), which is independent of the assay used.
In conclusion, the present data support the use of MCO or ICO cutoff values instead of the LoD or FS for TgAb positivity in the clinical setting. However, in accordance with the manufacturer, the use of the regional ICO for TgAb positivity is preferable to the MCO. Furthermore, TgAb positivity itself cannot be considered a separate risk factor and should presumably not be considered an independent risk factor for risk stratification.
Footnotes
Author Disclosure Statement
All of the authors can assure that the manuscript represents honest work and that no actual or potential financial interest is capable of influencing judgment.